
Abstract
Variations in the literature support the benefit of contact precautions for methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE) infections in the hospital setting. During personal protective equipment shortages throughout the COVID-19 pandemic, contact precautions were discontinued for MRSA and VRE-infected patients. Rates of hospital-acquired MRSA and VRE infections were compared before and after this intervention, along with hand hygiene proportions. Contact precaution discontinuation did not lead to an increase in hospital-acquired MRSA or VRE infections.
Keywords
Background
Gaps exist in the evidence supporting the benefits of contact precautions (CP) for the prevention of endemic methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE) infections. CP aims to decrease infectious transmission and is recommended for interactions with patients infected with multi-drug resistant organisms (MDRO), such as MRSA and VRE, in certain situations (Seigel et al., 2007). CP includes gowns and gloves as a form of personal protective equipment (PPE) worn by providers (Seigel et al., 2007). Although Siegel et al. (2007) advise CP for MRSA and VRE in acute care environments, results from other studies investigating hospital-acquired (HA) MRSA and VRE rates after CP removal (Bardossey et al., 2017; Bearman et al., 2018) draw into question whether CP in these patients is necessary.
The Centers for Disease Control and Prevention (CDC) allow CP suspension for MRSA and VRE in cases of PPE shortages, such as during the COVID-19 pandemic (CDC, 2020; CDC, 2021). As per CDC crisis guidelines, the use of gowns and gloves for patients with MRSA or VRE infections can be discontinued to conserve PPE for high-risk situations (CDC, 2020; CDC, 2021).
This study was implemented at a quaternary academic medical center (600 beds) in Texas. Our facility is a major referral center for solid organ transplantation and cardiovascular surgeries. Similar to hospitals worldwide, our facility saw an increase in the COVID-19 census of 40–110 patients during the study period. CP was discontinued due to the PPE crisis status.
We aimed to evaluate the impact of discontinuing CP on hospitalized patients with MRSA and VRE infections. We hypothesized CP discontinuation would not increase HA MRSA and VRE infection rates.
Methods
The pre-intervention period (March 2019–February 2020) included using CP for patients with confirmed MRSA or VRE infections at five hospitals in a healthcare system in Texas. The intervention period (March 2020–July 2020) included discontinuing CP for MRSA and VRE due to PPE shortages.
The study’s primary outcomes were the rates of HA MRSA and VRE infections per 10,000 patient days. Secondary outcomes comprised the rates of HA MRSA bacteremia per 10,000 patient days and hand hygiene percentage.
We calculated the monthly proportion of hand hygiene compliance with 95% confidence interval (CI), and the monthly rates of HA MRSA, HA MRSA bacteremia, and HA VRE per 10,000 patient days with 95% CI. We used the National Healthcare Safety Network definitions to identify infections. We obtained infections and patient days from TheraDoc Surveillance System (Premiere©, Salt Lake City, UT). Infection preventionists collected hand hygiene observations for patient room entry and exit.
Interrupted time series analysis with segmented regression analysis (Newey–West) was used to assess the effect of removing contact precaution on HA MRSA per 10,000 patient days, HA MRSA bacteremia per 10,000 patient days, HA VRE per 10,000 patient days (using Poisson regression), and hand hygiene percentage (using logistic regression).
The Institutional Review Board at Baylor College of Medicine approved this study under protocol number H-48949. R Version 4.2.2. (Vienna, Austria) was used for data analysis; statistical significance was calculated using a significance level of 0.05.
Results
Infection events and hand hygiene percentage.
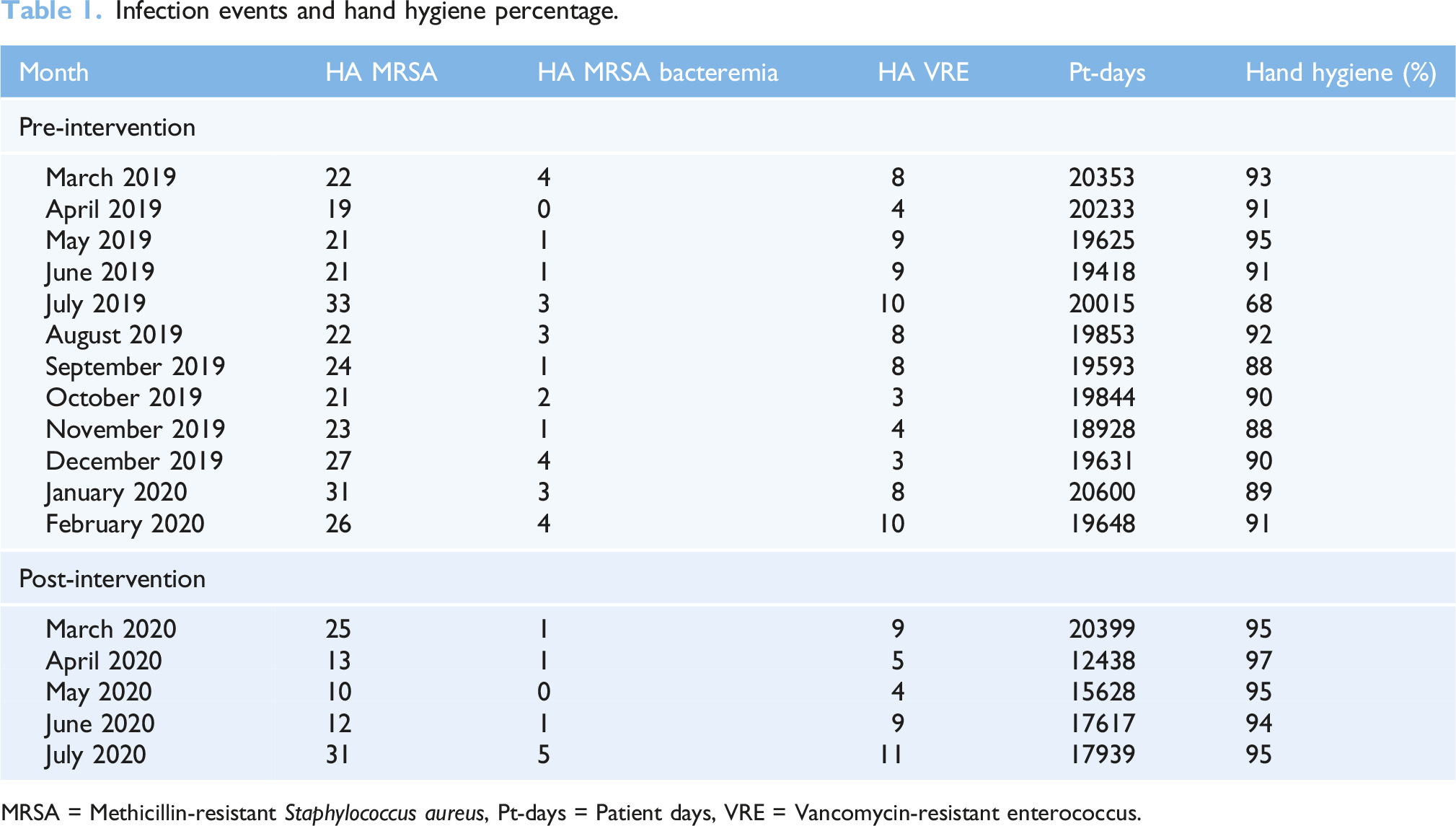
MRSA = Methicillin-resistant Staphylococcus aureus, Pt-days = Patient days, VRE = Vancomycin-resistant enterococcus.
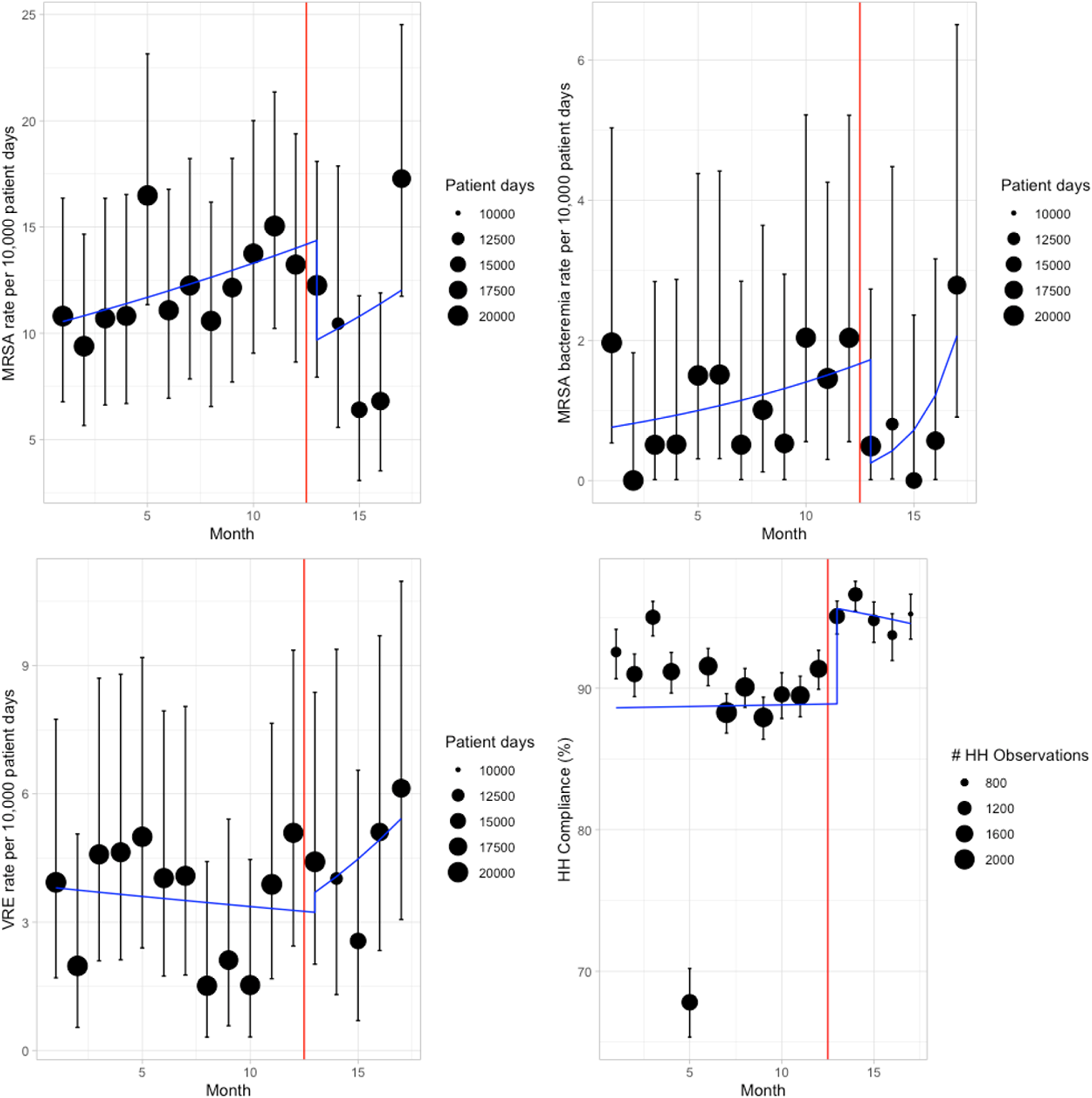
Interrupted time series analysis. This figure represents interrupted time series for hospital-acquired MRSA rate per 10,000 patient days (top left), hospital-acquired MRSA bacteremia rate per 10,000 patient days (top right), hospital-acquired VRE rate per 10,000 patient days (bottom left), and the percentage of hand hygiene (bottom right). Note: the intervention was implemented in March 2020. HH = Hand hygiene, MRSA = Methicillin-resistant Staphylococcus aureus, VRE = Vancomycin-resistant enterococcus.
Summary of Poisson and logistic models.
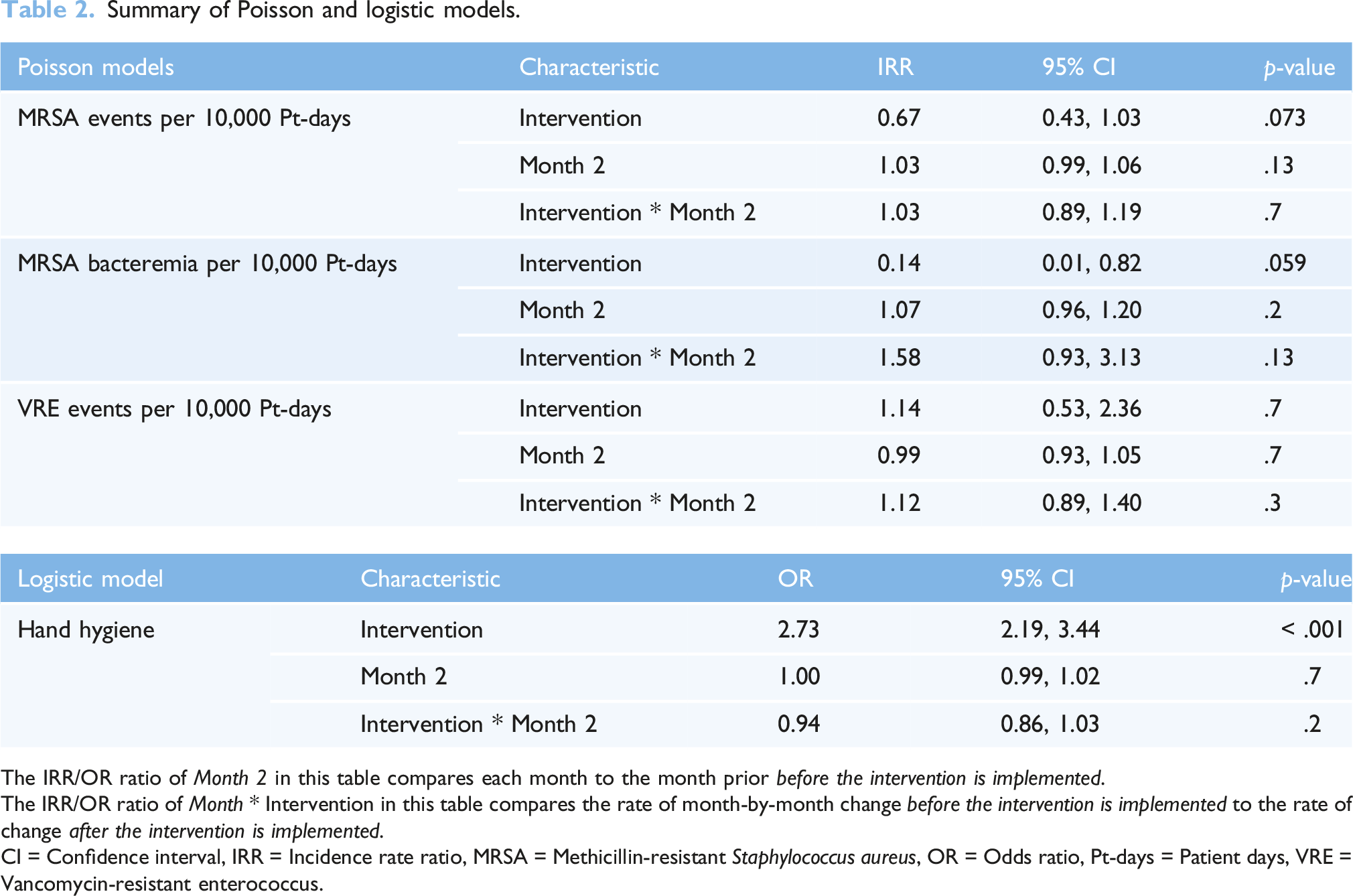
The IRR/OR ratio of Month 2 in this table compares each month to the month prior before the intervention is implemented.
The IRR/OR ratio of Month * Intervention in this table compares the rate of month-by-month change before the intervention is implemented to the rate of change after the intervention is implemented.
CI = Confidence interval, IRR = Incidence rate ratio, MRSA = Methicillin-resistant Staphylococcus aureus, OR = Odds ratio, Pt-days = Patient days, VRE = Vancomycin-resistant enterococcus.
The rate of HA MRSA bacteremia was 1.13 per 10,000 patient days in the pre-intervention period compared to 0.93 after the intervention. Similarly to overall MRSA infections, the change in predicted HA MRSA bacteremia rate due to the intervention was not significantly different in Month 13 with and without the intervention (1.61 vs 0.25 per 10,000 patient days, p = .059). The change between pre- and post-intervention slope on the log scale was also not significant (p = .13).
The rate of VRE infections was 3.5 per 10,000 patients before the intervention versus 4.44 after the intervention. There was no change in the predicted HA VRE rate due to the intervention in Month 13 (3.28 per 10,000 patient days before, 3.7 after the intervention, p = .7). The slope change on the log scale was not significant (p = .3).
In the pre-intervention period, the percentage of HH compliance was 93.31%, compared to 97.36% in the post-intervention. The predicted HH compliance increased due to the intervention in Month 13 (88.87% to 95.63%, p < .001). There was no change in the slope on the log odds scale (p = .2).
Discussion
Discontinuing CP for MRSA and VRE patients in the hospital setting did not lead to a statistically significant increase in HA MRSA or VRE infections. In fact, rates of HA MRSA trended down after CP discontinuation. These findings may be secondary to improvements in hand hygiene due to heightened awareness during the COVID-19 pandemic, thus limiting transmission between one patient to another despite the lack of gown and glove utilization. Other unmeasured factors may have impacted these findings, including potential changes to colonization pressures, case mix, and COVID-19 fatigue.
Existing literature demonstrates similar conclusions to our study. A systematic review by of 14 studies by Marra et al. (2018) investigated rates of MDRO infection after CP discontinuation. Pooled risk ratios found decreased rates of MRSA infection and significantly decreased rates of VRE infection with CP cessation (Marra et al., 2018). Kleyman et al. (2021) expanded this research in a larger systematic review that included 17 studies assessing mainly HA MRSA and/or VRE infections. Similarly, pooled risk ratios found no change in HA MRSA infection rates and a significant reduction in HA VRE infection rates with CP discontinuation (Kleyman et al., 2021).
A large retrospective study examining CP discontinuation performed by Bardossy et al. (2017) demonstrated no adverse effect on HA MRSA and VRE infection rates. Bearman et al. (2018) found no increase in device-associated HA MRSA or VRE infections after removal of CP in patients either infected or colonized with these species. These conclusions suggest there may be limited benefits of routine CP utilization in endemic MRSA and VRE-infected patients, which would be important in PPE shortages.
However, other studies have shown a role of CP in prevention of MRSA transmission. A multicenter cohort study at Veterans Affairs (VA) hospitals nationwide demonstrated a 47% reduction in MRSA transmission in patients with CP (Khader et al., 2021). Conclusions from this study may have differed from our own MRSA-related results due to differences in methodology and research focus. Our study only evaluated active infections, while that study assessed MRSA transmission linkage between patients as well as colonization data from surveillance testing (Khader et al., 2021). Additionally, this study utilized a modeling approach to estimate transmission effects, which required several assumptions, such as CP initiation within specific timeframes for patients testing positive for MRSA (Khader et al., 2021). Potential lags in CP initiation in the clinical setting could have impacted this study’s findings by over-estimating the role of CP in transmission prevention (Khader et al., 2021).
Contact isolation has also been associated with negative patient implications in terms of mental health and quality of care (Abad et al., 2010; Kuller et al., 2016). Patients in isolation experience negative psychological effects, decreased patient satisfaction, and less time with providers (Abad et al., 2010; Kuller et al., 2016). Given this evidence, CP discontinuation for MRSA or VRE-infected patients may result in improved patient care and psychological comfort.
For limitations, the lack of increase in HA MRSA and VRE infections could be explained by increased rates of hand hygiene or other COVID-19-related measures during the pandemic. In a non-pandemic setting, hand hygiene might decrease, potentially leading to increased HA MRSA and VRE infections. This study investigated rates of HA MRSA and VRE infections only, so the results cannot extrapolate to other pathogens requiring CP, such as Clostridiodes difficile. Additionally, rates of HA infections may differ in hospitals nationwide, and this sample population only involved patients in Texas. Furthermore, this pre-post study design did not include a control group, given the COVID-19 pandemic at the time of intervention implementation. It also did not assess for other confounders (e.g., case mix index, COVID-19 fatigue). Data for the post-intervention group was only collected for 5 months, which is a shorter follow-up period compared to the pre-intervention group.
Findings in this study contribute to existing evidence that utilizing CP for hospitalized patients with MRSA or VRE infection may not be necessary to prevent infectious transmission of these organisms. Furthermore, the unnecessary utilization of PPE can be regarded as medical waste, drawing cost considerations and environmental impact into clinical consideration. Further investigations may be aimed at establishing CP discontinuation policies for MRSA and VRE infections outside of critical PPE shortages.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.