
Abstract
Background:
Many investigations into the determinants of hand hygiene (HH) behaviour have explored only individual predictors or were designed according to arguably overly simplistic models of behaviour. Consequently, important influences on HH behaviour, including habit and emotion, are sometimes neglected. This study is the first to employ the Theory of Interpersonal Behaviour as a comprehensive model for understanding the determinants of HH behaviour.
Method:
A self-report questionnaire was conducted with staff from two large UK veterinary referral practices. Participants (n = 75) reported their HH behaviour and responded to statements rating the importance of social norms, self-protection, patient protection, time pressures, access to equipment, habit and disgust, to their HH behaviour.
Results:
Regression analysis showed that, overall, determinants explained 46% of variance (p < .001) in self-reported HH behaviour, with time constraints being the strongest predictor (β = −.47, p < .001) followed by difficulty finding equipment (β = −.21, p = .05).
Discussion:
Time constraints may be the most important influence on HH adherence among the determinants investigated. Future researchers should consider employing theoretical models to aid a more comprehensive understanding of the psychology underlying HH adherence and HH interventions.
Introduction
Hand hygiene (HH) is regarded as the most cost-effective means of reducing health-care associate infections, including those involving antimicrobial resistant organisms (World Health Organisation, 2016). Yet, in both human and animal healthcare, studies have shown that adherence with HH guidelines is inadequate and remains suboptimal even after interventions intended to improve adherence (Erasmus, 2010; Shea and Shaw, 2012). Consequently, considerable efforts have been made to understand the factors underlying HH behaviour, especially as the World Health Organisation has called for more theory-informed research to help design more effective interventions (WHO, 2016).
Following established methods in the behavioural sciences, several prominent studies have designed self-report questionnaires to investigate healthcare workers’ beliefs and motives, which are then used to predict observed or self-reported HH adherence (De Wandel et al., 2010; Larson and Killien, 1982; O’Boyle et al., 2001; Pessoa-Silva et al., 2005; Pittet et al., 2004; Sax et al., 2007). These studies have identified several important cognitive determinants, including beliefs about negative outcomes for patients and staff (Larson and Killien, 1982), social pressures from senior staff and colleagues (Pessoa-Silva et al., 2005) and perceived ability to perform HH (O’Boyle et al., 2001; Sax et al., 2007). Although systematically conducted, these studies were designed to measure cognitive determinants of behaviour within the constraints of Ajzen’s (1991) Theory of Planned Behaviour (TPB). However, this theory has been criticised (e.g. Sniehotta et al., 2014) because it treats all behaviour as the outcome of conscious deliberation and neglects non-conscious processes, such as habit and emotion, that are increasingly recognised as major influences on behaviour (Dyson et al., 2011; Sheeran et al., 2013). The current study used a more comprehensive theoretical model of behaviour – The Theory of Interpersonal Behaviour (TIB; Triandis, 1977) – to investigate both the conscious and less conscious determinants of HH behaviour. To the best of our knowledge, no previous study of the determinants of HH has used the TIB.
There is much overlap between the TPB and TIB, and both are intended as general-purpose theories of behaviour. Both agree that deliberate intentions to perform behaviour are influential and that these intentions are determined by several other variables, including beliefs about the anticipated positive and negative consequences of the behaviour (perceived consequences) and perceptions of what others think about the behaviour (social norms). However, according to the TPB, people’s conscious intentions are the immediate causes of behaviour, whereas the TIB additionally emphasises less conscious, more impulsive and automatic determinants, including habit and emotion. An additional difference is that the TPB emphasises people’s perceived control over behaviour, whereas the TIB acknowledges more objective facilitating conditions that impede or enable behaviour.
In recognising the importance of automatic influences on behaviour, the TIB is better aligned with contemporary theories of cognition (Mitchie et al., 2005; Sheeran et al., 2013; Sniehotta et al., 2014), and, in addition, we suggest that the TIB fits better with the available evidence on the determinants of HH. Although many of the most prominent quantitative studies have limited their investigation according to the constraints of the TPB (e.g., O’Boyle et al., 2001; Pessoa-Silva et al., 2005; Pittet et al., 2004; Sax et al., 2007), many other studies, especially interview-based qualitative studies, indicate that emotion, habit and concrete facilitating conditions, especially time constraints, are important influences on HH adherence (Chatfield et al., 2017; Dyson et al., 2011; Smiddy et al., 2015; Smith et al., 2018; Whitby et al., 2006).
The emotion most commonly implicated in studies of HH is disgust. Healthcare workers frequently report that feeling disgusted, dirty, or contaminated by what they have touched, and report that this often motivates them to engage in HH (Chatfield et al., 2017; Whitby et al., 2006).
Habits are learned behaviours that are performed automatically in response to stable situational cues (Gardner et al., 2012). Several studies indicate that HH may be performed most reliably in the contexts in which it is habitual (Curtis et al., 2009; Dyson et al., 2011; Smiddy et al., 2015; Whitby et al., 2006). Habit may be a particularly important determinant to investigate, because in busy clinical environments in which multiple tasks compete for practitioners’ conscious attention, automated behaviour has a better chance of being performed (Sax et al., 2007).
Finally, in numerous studies, healthcare workers report specific objective barriers, such as lack of access to infection prevention and control (IPC) equipment, as reasons why they do not perform HH more frequently. Time constraints and busy work environments are the most consistently mentioned barriers (Chatfield et al., 2017; Smiddy et al., 2015; Smith et al., 2018; Whitby et al., 2006) and may be important predictors of behaviour (De Wandel et al., 2010). This evidence suggests that the TIB model, which includes automatic determinants and specific barriers, rather than perceived control, may be a more suitable framework than the TPB for designing comprehensive investigations into HH behaviour.
Present research
The primary aim of the research reported here was to determine how well determinants based on the TIB predicted self-reported HH frequency. In line with previous systematic questionnaire-based studies of HH determinants (e.g., Sax et al., 2007), we designed self-report questions (items) to measure self-reported HH frequency and psychological determinants of HH.
Methods
Participants
Our questionnaire was sent to all staff in two large veterinary referral practices in the UK. One practice had 150 clinical staff and specialised in orthopaedics and neurology. The other had 45 staff and specialised in oncology and soft tissue surgery. Although most previous research into HH has been conducted in human practices, research suggests that similar determinants apply in veterinary settings, and the WHO’s five moments of HH have been recommended for use in veterinary practice (Anderson and Weese, 2016). The practices’ own IPC policies follow the WHO’s HH recommendations and WHO hand hygiene posters are displayed in prominent locations.
Materials and procedure
An email was sent to all staff at the practices inviting them to voluntarily participate in the online 20-min survey in exchange for the opportunity to win a monetary reward. A reminder email was sent after 2 weeks and data collection terminated after a further 2 weeks. All procedures were approved by the University of Surrey Ethics Board (ID: 353003-352994-35036673). The survey focused on HH and its determinants. We do not measure every component found on the TIB (such as intentions) because our focus was on understanding key determinants of HH within this context, rather than on testing the whole TIB, for which we did not have access to a large enough sample size. Measures relating to other aspects of IPC (e.g. disinfecting surfaces) were collected for use in a wider research project, but are not reported in the current article.
Self-reported HH behaviour
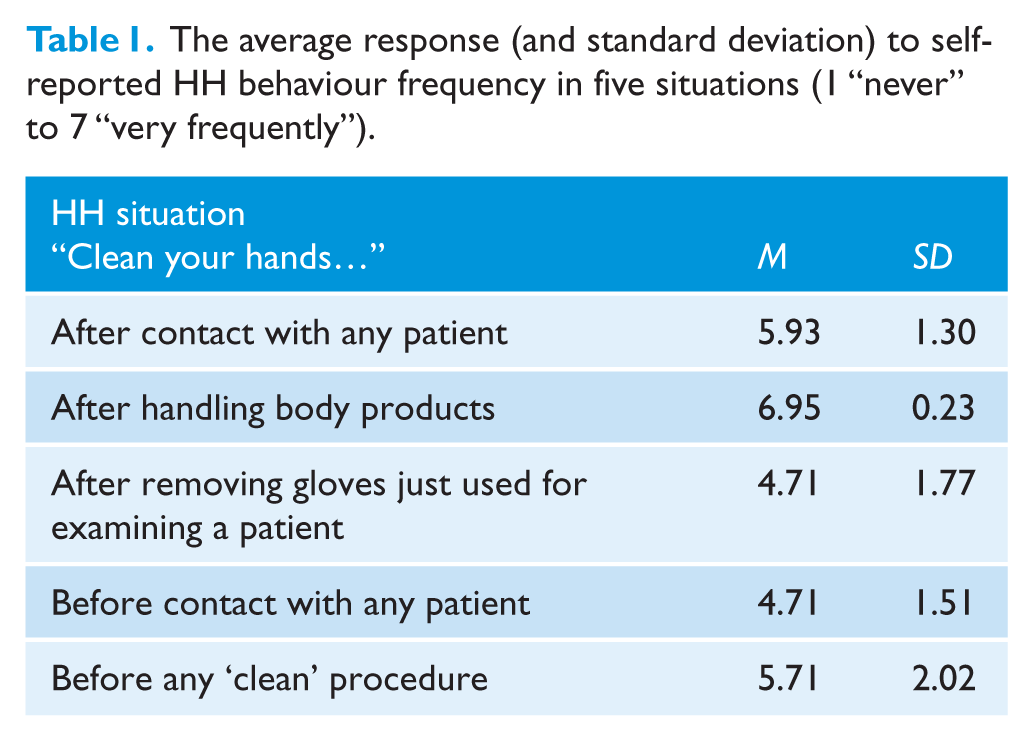
In order to develop and compare with previous research, we adapted existing items to examine self-reported HH behaviour. Based on Sax et al., 2007 in particular, participants were asked to estimate how frequently they perform several HH behaviours in their day-to-day practice by responding on a 7-point scale from 1 “never” to 7 “very frequently”. These items (see Table 1) assess the WHO five moments of HH (WHO, 2016).
The average response (and standard deviation) to self-reported HH behaviour frequency in five situations (1 “never” to 7 “very frequently”).
Determinants of HH behaviour
Participants then responded to several items designed to measure perceived importance of determinants of their self-reported HH behaviour. All items were rated on a 7-point scale from 1 “strongly disagree” to 7 “strongly agree”.
Social norms
Items were similar to those used in previous research (e.g. Sax et al., 2007): “My co-workers would be concerned if I failed to perform IPC behaviour”; “Carrying out IPC behaviours is not important to my colleagues” (negatively worded to avoid response bias); and “senior staff expect me to perform IPC behaviours”. Here and elsewhere the instructions explained that “IPC behaviours” included HH with alcohol-based hand rub, or hand washing with soap and water. Responses to these statements were then averaged to produce a measure for social norms. Cronbach’s α, calculated using SPSS 25, found that the items had a reliability of α = 0.74. This meets typical recommendations for minimum scale reliability of 0.6 to 0.7 (e.g. Streiner, 2003).
Perceived consequences
Previous research into the determinants of HH adherence suggests the most important beliefs, that is, the anticipated positive and negative consequences of the behaviour may be self-protection and patient-protection (Larson and Killien, 1982; Smiddy et al., 2015). Based on this research, we constructed items to be of similar format to the other items used in the current survey.
Self-protection
“I carry out IPC behaviours…to prevent myself from getting infections”, “…to protect my family from getting infections”, and “…to protect myself from contracting a disease” (α = 0.81).
Patient-protection
“I carry out IPC behaviours to…prevent animals from getting infections”, “…to protect vulnerable animals”, “…to avoid contaminating patients” (α = 0.82).
Facilitating conditions
Time constraints consisted of three items: “Carrying out IPC behaviours are too time-consuming to be strictly adhered to”; “When pushed for time it is often impractical to carry out IPC behaviours”; and “It is difficult to always perform IPC behaviours” (α = 0.58). Equipment access was measured with a single item: “It is often difficult to find equipment that enables me to carry out IPC behaviours (e.g. alcohol-based hand rub)”.
Habit
Items were adapted from the Self-Report Behavioural Automaticity Index (SRBAI, Gardner et al., 2012), a validated scale used widely in health psychology: “Carrying out IPC behaviours is something…I do without having to consciously remember”; “…I just do automatically in certain situations”; and “…I just do without thinking in some circumstances” (α = 0.64).
Emotion (Disgust)
Items were devised based on research into the subjective components of the emotion (e.g., Nabi, 2002): “Feeling disgusted often leads me to perform IPC behaviours”; “I often perform IPC behaviours if I feel contaminated”; and “I often perform IPC behaviours if I feel grossed out” (α = 0.67).
Analysis
We calculated and report average scores for each participant on HH frequency and all determinant scales. We then used regression analysis to reveal the contribution of each determinant to self-reported HH frequency. All analyses were conducted using SPSS version 25. All tests were two-tailed, and a p value < 0.05 was defined as statistically significant
Results
Participants
In total, 75 respondents (38% response rate) completed the survey (53 female; Mage = 33.63 years, SDage = 8.89). Of these, 27 were nurses, 16 auxiliaries, 17 veterinarians and 15 classified themselves as “other” (e.g. radiographer; physiotherapist). Respondents had worked in veterinary practice for a mean of 8.99 years (SD = 7.80) and at the practice for 3.18 years (SD = 2.55). On average, respondents estimated receiving 6.1 h (SD = 11.9) of IPC training over the course of their career.
Determinants of behaviour
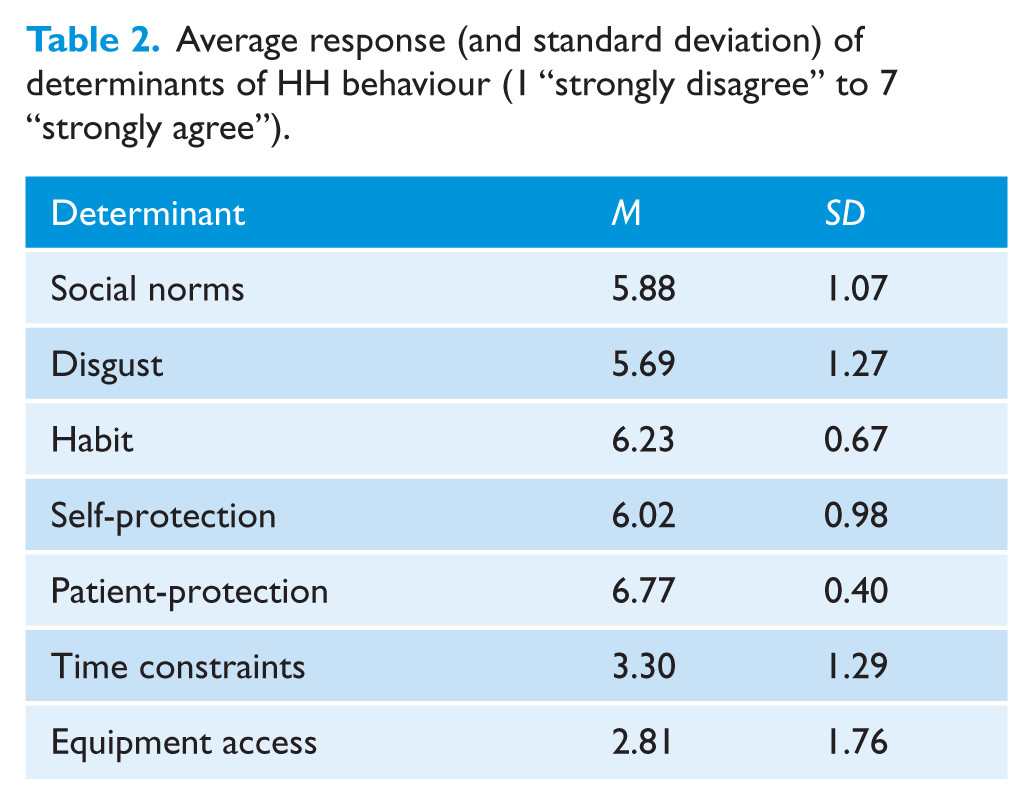
Descriptive statistics for self-reported frequency of HH in each situation are detailed in Table 1 and the descriptive statistics for the self-reported determinants of HH are detailed in Table 2. According to self-report, patient protection was the most important reason for performing HH, scoring close to the top of the 7-point scale. In contrast, time constraints and access to equipment were rated as relatively unimportant influences, both scoring below the scale midpoint.
Average response (and standard deviation) of determinants of HH behaviour (1 “strongly disagree” to 7 “strongly agree”).
A hierarchical regression analysis was conducted in which the single HH scale (i.e. the mean of the five HH items, which formed a reliable scale, α = 0.65) was regressed upon participant age and sex (the first step), then on the seven determinant variables (the second step) (Table 3). This approach allows for examination of the relationships between HH frequency and psychological determinants while controlling for demographics. Inspection of histogram plots revealed that the distributions of scores on several determinants were negatively skewed (i.e. majority of participants overall strongly agreed with the statements); however, inspection of residual plots and probability plots showed that residuals were normally distributed, meaning that the data met assumptions necessary for regression analysis.
Regression analysis, predictors of self-reported HH frequency.
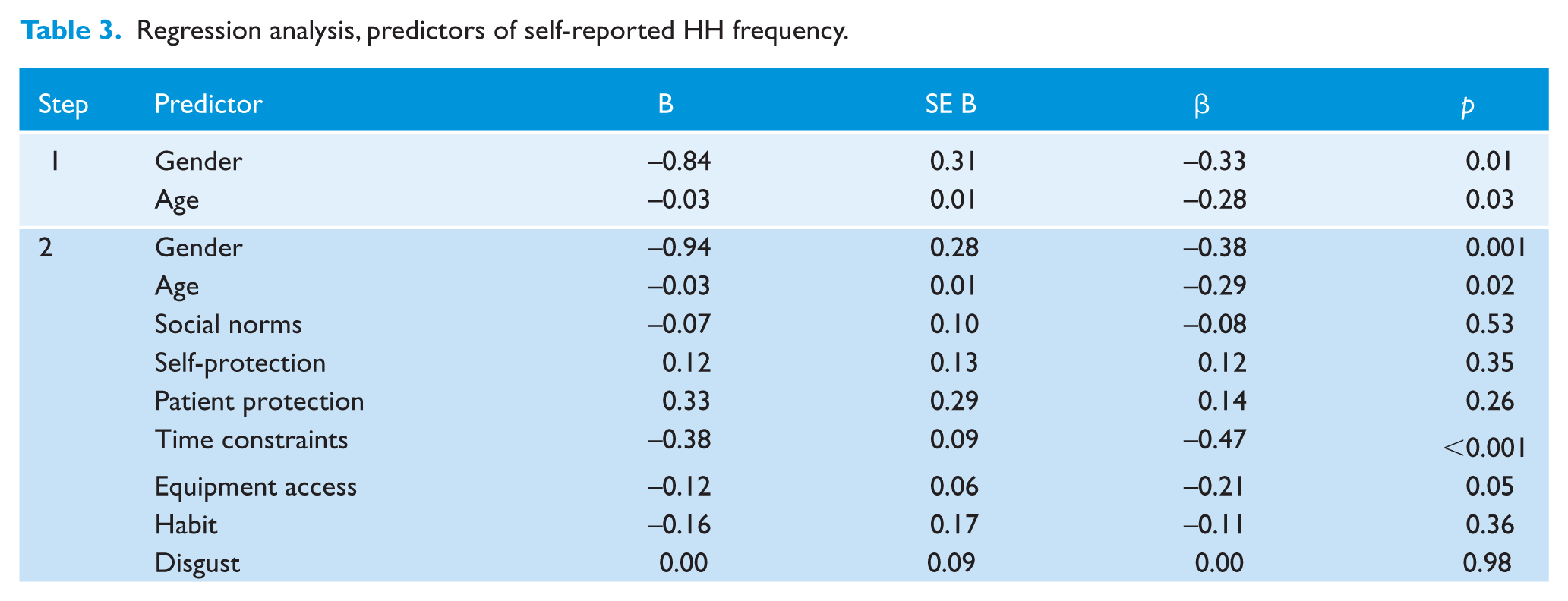
Age and gender produced a significant model predicting self-reported HH, F(2,62) = 4.77, p = 0.01, explaining 14% of the variance, but the model significantly improved by including TIB related determinants, ΔR2 = 0.33, F(2,62) = 4.59, p < 0.001, explaining 46% of the variance in HH. At the level of individual predictors, in contrast to the self-reported importance of determinants, only two TIB-related determinants were significant predictors: time pressures and difficulties accessing equipment. Higher agreement that these were important barriers was associated with lower self-reported HH frequency.
Discussion
Participants strongly agreed that they perform HH to protect patients and also agreed that self-protection, habit, disgust and social norms influence their HH behaviour, yet, according to regression analysis, only time constraints and difficulties accessing equipment significantly predicted self-reported HH frequency. One reason for this discrepancy could be the social desirability of agreeing that factors such as patient protection are important despite its lack of influence on HH. A related possibility is that when reflecting on their behaviour, participants genuinely believe that factors such as patient protection are most important, but in a busy clinical environment, such concerns have less salience.
One limitation of the present study, which is shared by previous studies (e.g. Sax et al., 2007), is that determinants of HH were asked across situations, rather than asking participants to respond to the items separately for each HH situation. It is possible that some determinants would emerge as significant predictors in more specific HH situations. For example, disgust and habit have been implicated as determinants of HH following contact with body fluids or contact with patients because of visible contaminants and dirt (Curtis et al., 2009; Whitby et al., 2006). Accordingly, as well as avoiding an overly simplistic approach to identifying determinants, the specific situations should also be examined in greater detail in future research.
Nevertheless, the finding that time constraints was the strongest predictor of self-reported HH coheres with several existing findings (e.g. De Wandel et al., 2010; Smith et al., 2018). Pessoa-Silva et al. (2005) and Sax et al. (2007) found that self-reported HH frequency among human medical professionals was most strongly predicted by the belief that relatively little effort was required to perform HH. However, these studies did not examine time pressures specifically, nor other determinants such as habit and disgust, because they followed the TPB model. Multiple qualitative studies based on interviews show that time pressures and high workload are frequently given as reasons for not performing HH (Chatfield et al., 2017; Smiddy et al., 2015), and behavioural observation studies have found that lower observed HH adherence is most strongly associated with actual or perceived workload (O’Boyle et al., 2002; Pittet et al., 2004). Although this evidence derives from human healthcare, other research suggests that time pressures may be equally important in veterinary settings (Anderson and Weese, 2016); in one veterinary study over 70% of participants gave “too busy” as the main reason for not performing HH (Nakamura et al., 2012).
These findings have implications for interventions intended to improve HH adherence, suggesting that they could be designed to address perceived and actual constraints on time. One way to achieve this might be to factor in time for HH into healthcare workers’ schedules. Another might be to seek to develop HH into a habit, because once behaviour becomes automatic, actual and subjectively experienced attentional demands are reduced (Gardner et al., 2012).
By controlling the setting, the resulting sample size was not appropriate to run further analyses to test the entirety of the TIB model. It also means that we cannot know for certain how our findings generalise to other samples, such as healthcare workers in human medicine. It is also possible that findings would not generalise from self-reported behaviour to observed behaviour because some items, such as HH frequency, may be subject to social desirability bias. Despite these limitations, our results demonstrate that the TIB may have predictive utility. Together with its coherence with contemporary theories of cognition (Sheeran et al., 2013; Sniehotta et al., 2014), this suggests that the TIB may be a useful model for understanding the psychology of HH behaviour in medical and veterinary settings.
Footnotes
Acknowledgements
The authors would like to thank Shona Noble and Matthew Poyade for their input into the study and the overall research project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported here was funded by an Arts and Humanities Research Council (AHRC) Antimicrobial resistance (AMR) grant (grant number: AH/R002088/1).
Peer review statement
Not commissioned; blind peer-reviewed.