
Abstract
Background:
Prostatitis can be challenging to treat. In refractory cases, prostatitis can be treated surgically with transurethral resection.
Objectives:
To examine the safety and efficacy of holmium laser enucleation of the prostate (HoLEP) as treatment in patients with prostatitis.
Design and methods:
Patients who underwent HoLEP at a single center between January 2021 and August 2023 were retrospectively reviewed. Preoperative, intraoperative, and postoperative parameters were collected and analyzed. Patients with an ICD-10 diagnosis of prostatitis were identified and contacted postoperatively to evaluate for recurrent symptoms. Statistical significance was defined as p < 0.05.
Results:
We identified 918 patients, of whom 26 (2.8%) had a diagnosis of prostatitis. There were no differences in baseline characteristics between patients with and without prostatitis. Patients with prostatitis were less likely to have a history of a neurologic disorder (p = 0.035), less likely to be catheter-dependent (p = 0.005), and less likely to have a preoperative positive urine culture (p = 0.040). There were no significant differences in intraoperative and postoperative parameters between the two groups. There were 23/26 (88.5%) patients with follow-up. There were no episodes of recurrent prostatitis and one episode of UTI after surgery, with a mean follow-up of 19.39 months (range: 7.45–30.19, SD: 7.38).
Conclusion:
Prostatitis patients undergoing HoLEP had comparable safety and efficacy profiles to those who did not have prostatitis. On follow-up, 100% of patients with prostatitis did not experience recurrent prostatitis, suggesting that HoLEP may have a role in the management of prostatitis in the presence of benign prostatic enlargement.
Introduction
Prostatitis is a common diagnosis in the United States, with an estimated 2 million visits in 1 year. 1 Epidemiological studies estimate an 8.2% prevalence of prostatitis-like symptoms across multiple countries and age ranges. 2 Multiple types of prostatitis that have been identified: acute and chronic bacterial prostatitis, nonbacterial prostatitis, and prostatodynia. 3 These types have further been classified into four categories: acute bacterial (category I), chronic bacterial prostatitis (category II), chronic pelvic pain syndrome (CPPS) (category III), and asymptomatic prostatitis (category IV). 4 Treatment for prostatitis varies based on type. Category I and II prostatitis are treated with antibiotics. 5 Category III prostatitis, also known as chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), is the most common type of prostatitis. 4 There is a lack of consensus on the etiology of this type of prostatitis, making unimodal treatment difficult.4,6 Treatment involves antimicrobials, alpha-blockers, anti-inflammatories, and other medical therapies. Category IV is less commonly diagnosed, due to patients being asymptomatic. 4 It can be treated with antibiotic therapy, although the advantages relative to no treatment remain unclear. 7
Surgical treatment modalities of prostatitis have been explored. Transurethral resection of the prostate (TURP) is more effective in bacterial types of prostatitis than in CP/CPPS. 8 Other minimally invasive therapies for chronic prostatitis have been tried, such as heat therapy, laser therapy, injection therapy, balloon dilation, and electromagnetic therapy. 9 However, due to inconsistencies in study methods, applications, and outcomes, these treatments have not become standard of care.
Holmium laser enucleation of the prostate (HoLEP) has emerged as a size-independent treatment for benign prostatic hyperplasia (BPH). 10 It has been shown to have improved operative time, length of stay, and catheter duration than open simple prostatectomy and robotic simple prostatectomy in large prostates. 11 HoLEP and other enucleation procedures have been shown to have operative and clinical superiority to TURP. 12 Limited studies have explored surgical modalities as curative treatments for prostatitis. While medical therapy for prostatitis is the least invasive modality, patients who are refractory to this therapy may benefit from surgical options. Herein, we explore prostatitis outcomes in patients who underwent HoLEP at our institution.
Methods
Study design and population
After Institutional Review Board (IRB) approval, we obtained written consent to enroll patients undergoing HoLEP at our institution were in a prospective study database (STU00213284). A retrospective review of all patients undergoing HoLEP at our institution and who were enrolled in the database between January 2021 and June 2023 was conducted. Our HoLEP technique has been previously described by Assmus et al. 13 Inclusion criteria were adult male patients who underwent HoLEP for BPH and had a charted diagnosis of prostatitis, defined as an International Classification of Disease (ICD) diagnosis code of N41.9, which is an ICD-9 code utilized for non-bacterial prostatitis. All patients with a history of prostatitis, positive urine culture, or who had an indwelling catheter or performed self-catheterization were treated with 1 week of culture-specific antibiotics before and after surgery. This ensured that no patient had an active prostatitis flare at the time of the procedure. Patients who did not meet the above criteria were administered IV antibiotics only at the time of surgical intervention. Patients under the age of 18 and over 89 were excluded from this study. Patients without the diagnosis code N41.9 were not included in the prostatitis group.
Clinical data included age, BMI, prior history of neurological diagnosis, prior history of diabetes, prior BPH history (surgery, medication), medication history, prostate size, history of prostatitis, and history of UTI. Symptomatic data were collected using the International Prostate Symptom Score (IPSS) and Michigan Incontinence Symptom Index (M-ISI) before and after surgery. Operative factors collected include procedure times, laser energy, weight resected, postoperative discharge, postoperative catheterization, and postoperative complications. Enucleation efficiency and morcellation efficiency were also calculated and are defined as the weight resected divided by enucleation and morcellation times, respectively. At postoperative follow-up, functional outcomes such as catheterization, post-void residual (PVR), medications, and continence status were recorded.
For routine follow-up, patients are evaluated by phone postoperatively at 1 week and later in the clinic at 3 months (Table 2). A research coordinator contacted patients with a prior diagnosis of prostatitis postoperatively. Patients were administered a modified NIH-CPSI survey and monitored for recurrent symptoms postoperatively. Data were collected on recurrent prostatitis, recurrent urinary tract infection (UTI), and discomfort and pain in the pubic area since the surgery.
Outcome measures
The primary outcome was the recurrence of prostatitis after surgery. Secondary outcomes included comorbidities, perioperative factors, and symptom recurrence as described above.
Statistical analysis
Statistical analysis was conducted on SPSS (IBM Corporation, Armonk, NY) software. Categorical variables were analyzed using chi-square tests and Fisher’s exact test as indicated. If data were missing from a certain category, it was excluded from that analysis, and the sample size was adjusted to account for available data. Continuous variables were analyzed with Student’s t-tests. Significance was defined as p < 0.05.
This study was conducted per the guidelines of the Declaration of Helsinki. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental Material).
Results
Baseline characteristics
There was a total of 918 patients who underwent HoLEP without concurrent endourologic procedures during our study period. There were 26 (2.83%) patients who had prostatitis, and there were 892 patients who did not have a history of prostatitis, which were used as the control group. The average age of the population with prostatitis was 68.5 (SD: 7.31). There was no difference in age (p = 0.156) or BMI (p = 0.455) (Table 1) between the prostatitis and control groups. Patients with prostatitis were less likely to have a history of a neurologic disorder (p = 0.035), less likely to be catheter-dependent (p = 0.005), and less likely to have a preoperative positive urine culture (p = 0.040). There were no significant differences in intraoperative and postoperative parameters between the two groups (Table 2). Patients were not less likely to utilize preoperative BPH medications (p = 0.410) or have prior BPH surgery (p = 0.158). There were no differences in prostate size between the two groups (p = 0.653) or preoperative PVR (p = 0.741).
Baseline demographic and perioperative outcomes for patients undergoing HoLEP.

BPH, benign prostatic hyperplasia; HoLEP, holmium laser enucleation of the prostate; IPSS, International Prostate Symptom Score; M-ISI, Michigan Incontinence Symptom Index; PVR, post-void residual. Bolded p-values indicate statistical significance.
Intraoperative and postoperative characteristics of patients undergoing HoLEP.

BPH, benign prostatic hyperplasia; HoLEP, holmium laser enucleation of the prostate; IPSS, International Prostate Symptom Score; M-ISI, Michigan Incontinence Symptom Index; PVR, post-void residual.
Primary outcomes
Mean follow-up for administration of the modified National Institutes of Health – Chronic Prostatitis Symptom Indes NIH-CPSI questionnaire in the prostatitis group was 19.39 months (range: 7.45–30.19, SD: 7.38). The follow-up questionnaire had an 88.5% response rate (23/26 patients). No patients in the prostatitis cohort reported a recurrent episode of prostatitis since surgery. There was one (4%) postoperative UTI reported in the prostatitis cohort compared to 37 (3.8%) in the control group. In the prostatitis group 4 (17%), patients reported having residual pain in the urethra and penile area, which was quantified to be between 2 and 4 on a 10-point scale by all patients (Table 3). However, two of these patients reported that this pain was like the pain experienced prior to surgery. Another patient reported that the pain was infrequent. The last patient reported that the pain had improved “a lot” since surgery.
Modified National Institutes of Health – Chronic Prostatitis Symptom Index (NIH-CPSI) questionnaire.

% represents the percentage of patients who responded to the questionnaire.
Secondary intraoperative and postoperative outcomes
There were no differences in HoLEP procedure time (p = 0.852), enucleation time (p = 0.805), and morcellation time (p = 0.925) between patients with and without prostatitis. There was also no difference in enucleation efficiency (p = 0.663) and morcellation efficiency (p = 0.867) between the two groups. The average postoperative catheterization time in the group of patients with prostatitis was 0.29 ± 0.85 days and 0.51 ± 1.5 days in the control group (p = 0.476). Complications were graded according to the modified Clavien Classification System. 14 Complications at 90 days after surgery occurred for 5 (19.2%) patients in the prostatitis group and 161 (18.0%) patients in the control group (Table 4). There were more Clavien IIIa complications in the control group (p < 0.00001). Readmissions at 90 days post-op occurred for 3 (13%) patients in the prostatitis group and 43 (5.3%) patients in the non-prostatitis group (p = 0.130). At 90 days post-op, 4 (15.4%) patients in the prostatitis group and 132 (15.3%) patients in the control group had an emergency department visit for any cause (p = 1.000). There were no visits related to recurrent prostatitis. Patients with prostatitis had an average baseline IPSS of 19.38 ± 5.45, and the control group had a baseline of 19.13 ± 7.50 (p = 0.897). Postoperatively, patients with prostatitis had an average IPSS score of 8.07 ± 4.91, and the control group average was 8.22 ± 5.65 (p = 0.927). The average change in IPSS was −11.09 ± 8.25 for the patients with prostatitis and −9.81 ± 8.78 for the control group (p = 0.632). The average baseline M-ISI Score for patients with prostatitis was 5.92 ± 5.25 and 5.69 ± 5.58 for the control group (p = 0.891). The average postop M-ISI score was 5.33 ± 5.27 for patients with prostatitis and 6.14 ± 6.40 for the control group (p = 0.707).
Complications of patients who underwent HoLEP were separated by history of prostatitis.
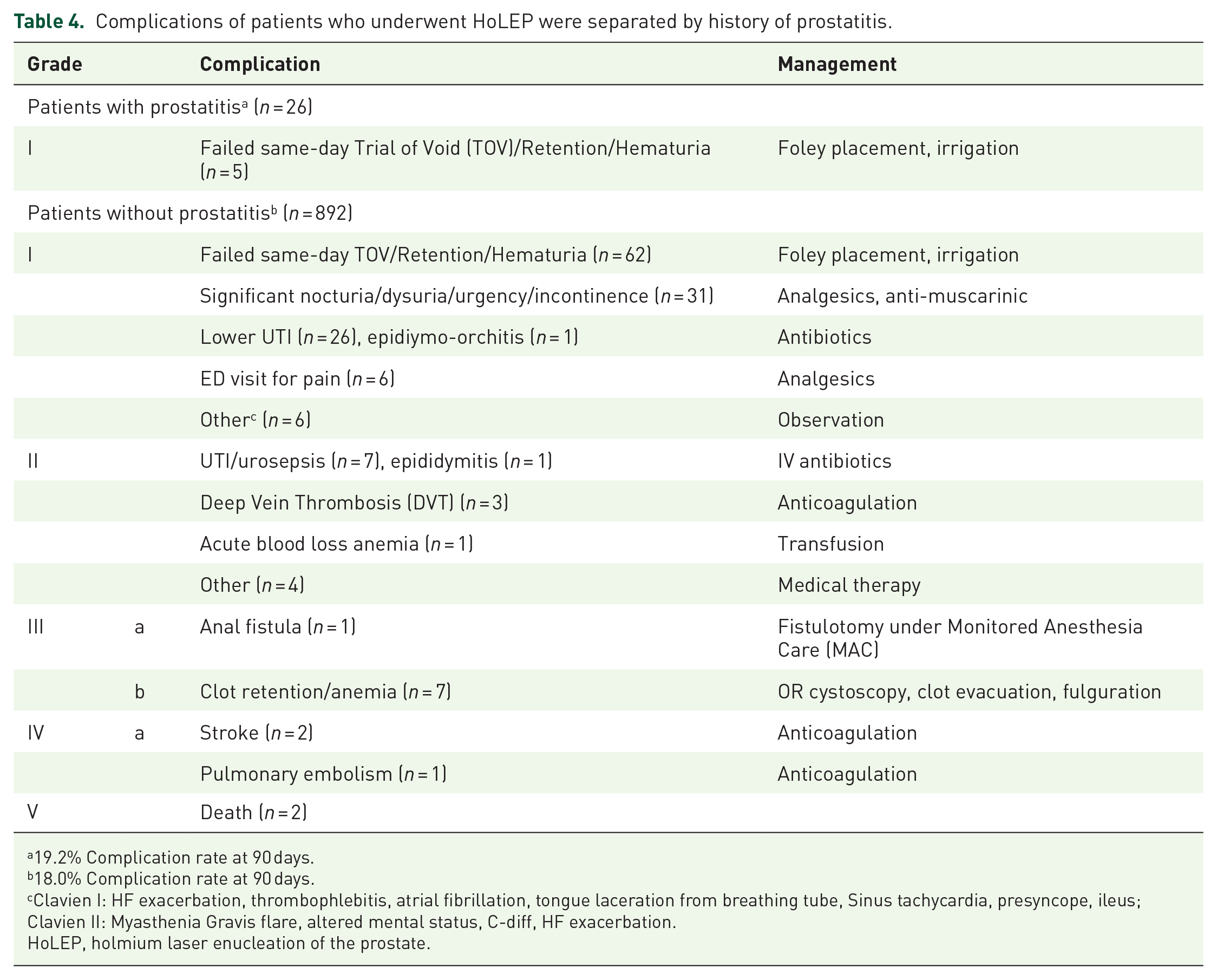
19.2% Complication rate at 90 days.
18.0% Complication rate at 90 days.
Clavien I: HF exacerbation, thrombophlebitis, atrial fibrillation, tongue laceration from breathing tube, Sinus tachycardia, presyncope, ileus; Clavien II: Myasthenia Gravis flare, altered mental status, C-diff, HF exacerbation.
HoLEP, holmium laser enucleation of the prostate.
Discussion
This study is one of the first to evaluate HoLEP as a possible adjunct therapy for prostatitis. In our review of patients with prostatitis undergoing HoLEP, we found that no patient had a prostatitis episode recurrence after surgery. We found that prostatitis patients undergoing HoLEP were less likely to have a neurological diagnosis, preoperative catheterization, or positive preoperative urine culture. Patients with prostatitis were otherwise similar to patients without prostatitis undergoing HoLEP.
There is limited literature assessing surgical treatments for prostatitis. Schoeb et al., in a systematic review, found that TURP had a 70% success rate for curing NIH type 2, NIH type 3, and patients classified as “chronic symptomatic prostatitis” across 110 patients in 6 studies. 15 The same study examined radical prostatectomy and found it to be 95% curative, with some patients reporting adverse side effects of erectile dysfunction and incontinence. 15 Chopra et al. 16 utilized robotic radical prostatectomy for CP/CPPS patients refractory to medical treatment and found that patients were able to recover continence with pre-prostatectomy counseling for Kegel exercises; however, the majority of patients reported low confidence in their ability to achieve erection. Similarly, Krongrad et al. 17 found that laparoscopic radical prostatectomy improved CPSI scores for patients, but had variable impacts on erectile function at 1 year. In both studies, patients were treated surgically after medical therapies had been exhausted unsuccessfully; however, there is no standardization of preoperative treatment, which necessitates a larger controlled study.16,17
There have been other interventional therapies attempted for treating prostatitis. Transurethral heat therapy and balloon dilation for chronic nonbacterial prostatitis had shown initial short-term results, but long-term efficacy was poor, and the treatment was associated with adverse events such as urinary retention, retrograde ejaculation, hematuria, urethral stricture, and worsening of symptoms. 18 Mené et al. 19 evaluated transurethral microwave hyperthermia for chronic non-bacterial prostatitis and found promising improvement with multiple sessions, reporting few adverse effects that self-resolved. Similarly, Nickel et al. conducted a controlled study on transurethral microwave thermotherapy in Category III prostatitis patients and found that the treatment group had improved symptoms. 20 Transurethral needle ablation has also been shown to be effective in improving patient symptoms for chronic nonbacterial prostatitis. 21 Ultimately, studies evaluating minimally invasive heat therapy methods have not standardized regimens and used validated symptom measures as a way to measure efficacy, making it hard to compare effectiveness. 22
Utilizing TURP as a curative treatment for prostatitis after patients have failed non-operative therapy has shown promising results. 15 Barnes et al. conducted a review of 49 patients who had undergone TURP for “chronic prostatitis” and found that approximately two-thirds of patients reported no residual symptoms. 23 Of the patients who failed to have symptom improvement, incomplete resection was cited as a cause of failure of treatment. HoLEP has recently emerged as an effective BPH treatment with superior functional outcomes for patients than TURP. Magistro et al. 12 found that enucleation techniques such as HoLEP and bipolar enucleation of the prostate (bTUEP) had a higher percentage of tissue retrieved than TURP, in medium-sized prostates.
In our study, we found that no patient had recurrent prostatitis, indicating that HoLEP may be more effective at this indication than existing modalities, which can be expected of a treatment with a superior tissue removal percentage. Furthermore, HoLEP is a size-independent treatment, 24 which enables it to be used for a wider patient population. Given that CP/CPPS has a mean yearly cost of $3017.00 per person, not including lost wages, it is important to find a curative therapy for patients with refractory symptoms. 25 There are limited studies that use a validated questionnaire to evaluate symptom recurrence, which is necessary to quantify the true efficacy of treatment. 15 In their systematic review, Schoeb et al. 15 only found 4 out of 16 studies that utilized the NIH-CPSI questionnaire to quantify symptoms for patients with prostatitis, and others utilized symptoms without a validated measurement. While symptomatic improvement of LUTS can be attributed to the HoLEP’s effect on BPH, as the NIH-CPSI pain score and IPSS total score are correlated, 26 our patients who have a history of prostatitis reported no new episodes of prostatitis since their procedure. This indicates that there is a possible therapeutic benefit for prostatitis symptoms in this patient population.
The secondary outcomes of this study were evaluated and found minimal differences between patients with and without prostatitis who underwent HoLEP. While the indication for all patients undergoing this procedure was BPH symptoms, refractory to medical therapy, our study prompts investigation into other possible therapeutic benefits for HoLEP. Complication rates were less than 20% in both cohorts, with primarily Clavien I complications (Table 4). There was also no difference in morcellation or enucleation efficiency between the two groups, which may indicate that inflammatory changes in the prostate do not make the HoLEP procedure more technically challenging in these patients, making it a feasible therapy.
There are a few limitations to our study. It is a retrospective study conducted at a single institution. However, HoLEP volume is high enough at our institution to generate enough cases for an exploratory study such as this one. Since this was an exploratory study, no power analysis was done to determine a sample size. This could be done in a prospective study designed to understand long-term outcomes of prostatitis in patients undergoing HoLEP. It is important to note that the retrospective nature of this study limits our ability to classify the kind of prostatitis diagnosis for each patient. Most diagnoses of prostatitis were done by other practitioners, and some were done at outside hospitals, making it infeasible to find the exact type of prostatitis and the prior therapies that patients had undergone. Further review of pathology for patients with prostatitis showed that 16 of the 26 patients diagnosed with prostatitis had commentary regarding chronic inflammation in their pathology report. Since this is not sufficient to diagnose chronic prostatitis, we illustrate the need for a controlled study that specifically recruits people with a diagnosis classified by prostatitis type. Patients were contacted postoperatively regarding symptoms, which are subject to recall bias. However, except for the prostatitis surveys, all data were retrieved from a prospectively managed database. Given that much of chronic prostatitis is based on a subjective assessment of symptoms, the type and severity of prostatitis cannot be assessed. Some patients did report recurrent pain in the penis, bladder, testicles, or pubic area; however, since they answered that they did not have recurrent prostatitis, they can likely distinguish this pain from prior prostatitis pain. Residual pain in the area could be due to other causes. In a future study, patients could be evaluated in a clinic to better elucidate whether the recent pain is related to prostatitis or another cause. Given the limited literature with validated questionnaires in this population, a prospective study with use of validated symptom measures could better outline the improvement that patients gain from undergoing HoLEP. Since our enrollment period was close to the time of evaluating the result of this study, the follow-up period for the most recent HoLEPs may be limited. However, for patients with chronic prostatitis, symptoms would likely recur in the 7-month period of follow-up, which was the shortest period of follow-up in this study. A further study with a larger prostatitis cohort with longer follow-up could be conducted to further evaluate this. Finally, HoLEP has a significant learning curve; thus, the efficacy of HoLEP will depend on the operator. As HoLEP becomes more widely adopted, there will be more practitioners able to offer their patients this treatment.
Ultimately, this study shows the potential for HoLEP to provide a surgical therapy for chronic prostatitis. Current therapies are lacking for patients with recurrent disease. There are few studies evaluating surgical therapy for chronic prostatitis, and the lack of standardization of the evaluation of these patients makes it difficult to determine which treatments are superior for chronic prostatitis. In the future, a controlled study with better prostatitis classification and longer follow-up will need to be conducted to determine whether HoLEP can be utilized as a curative therapy.
Conclusion
Our study indicates that HoLEP can be a helpful treatment for patients with prostatitis and symptomatic BPH. We found that none of the patients with prostatitis experienced a recurrent episode after their HoLEP at a mean follow-up of 19 months. This study lays the foundation for further exploration of HoLEP as a therapy for patients refractory to prostatitis treatment.
Supplemental Material
sj-docx-1-tau-10.1177_17562872251338430 – Supplemental material for Outcomes of holmium laser enucleation of the prostate in men with a history of prostatitis: a retrospective study
Supplemental material, sj-docx-1-tau-10.1177_17562872251338430 for Outcomes of holmium laser enucleation of the prostate in men with a history of prostatitis: a retrospective study by Meera Bhanu Ganesh, Perry Xu, Nicholas Dean, Kyle Tsai, Jamie Michael, Alyssa McDonald, Devyn Taylor Coskey, Nabila Khondakar, Allaa Fadl-Alla and Amy Elizabeth Krambeck in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.