
Abstract
Over the past two decades, there have been significant developments in paediatric urodynamic studies focusing on less-invasive monitoring devices, as well as re-defining normative values. This article reviews current paediatric urodynamic study methods and their reliability, and discusses new emerging ambulatory urodynamics and novel telemetric urodynamic devices. Traditional urodynamic studies are performed in specialised suites in real-time with artificial bladder filling. Ambulatory models allow for measurements in a more authentic environment and with natural bladder filling. Novel implanted telemetric monitoring devices provide a catheter-free solution but are inherently invasive in nature. Exploration of indirect measurements to obtain urodynamic data warrant further investigation. Definitive progress will require strong and sustained collaboration between end users and developers.
Introduction
Urodynamics (UDS) is an umbrella term for techniques that assess the lower urinary tract, ranging from clinical assessments, uroflowmetry to videocystometrography. 1 Urodynamic studies aim to detail and document the child’s bladder physiology during storage and voiding phases to allow identification of pathological patterns. 2 Urodynamic testing should provide the best available information to directly influence management of lower urinary tract disorders in children; both functional and structural. However, reproducibility is limited, and consistent study techniques are difficult due to a wide variety of challenges. Examples of this are numerous in uroflowmetry and cystometrography (CMG). For instance, interpretation of simple uroflow curves is hampered by marked inter-observer variability (0.21–0.64). 3 Furthermore, in a recent multicentre North American study on paediatric neurogenic bladder (UMPIRE study), there was only 50% agreement regarding bladder evaluation using CMG. Specifically, assessment of bladder risk category and risk of subsequent upper tract damage varied significantly between institutions. 4
Despite its’ shortcomings, CMG remains the current gold standard for defining lower urinary tract disorders in children, including those with complex urological and neurological disorders.5,6 This may be explained by historical context and subsequent development of a surrounding evidence-base rationalising CMG. Much of this fundamental understanding was established by Maguire et al. in the 1980s with systematic investigation of children with neurogenic bladders utilising video cystometrography. These studies related elevated detrusor leak point pressure and low-compliance bladders with a high rate of upper tract deterioration.7 –9
Despite its’ limitations (non-physiological quality, and propensity for artefact 4 ) many significant clinical decisions are currently based on CMG with far-reaching consequences for the child. For example, the largely irreversible decision to proceed with augmentation cystoplasty brings with it >20% risk of bladder urolithiasis, long-term risk of malignancy and a risk of bladder rupture/perforation that may be life-threatening. 10 Furthermore, if the child ultimately requires kidney transplantation, the combination of immunosuppression and the increased bacterial load following augmentation cystoplasty can make recurrent urinary tract infection (UTIs) highly problematic. Similarly, formation of a catheterisable channel carries a high complication rate (>50%). 10
New technologies including ambulatory urodynamic monitoring and telemetric ambulatory urodynamic monitoring are currently in development. These techniques allow for physiological evaluation in real-time as the child moves freely and the study continues remotely and catheter-free. 11 The main objective of this article is to review current paediatric urodynamic study methods and their reliability; to understand the deficits intrinsic to the current paradigm. This leads to a narrative review of new and emerging urodynamic techniques that have been (or may be) applied to paediatric patients.
Review of modality: Uroflowmetry ± electromyography
Uroflowmetry remains the current first-line diagnostic tool for evaluation of children with voiding disorders, lower urinary tract symptoms, or in those children with known structural or functional pathology. However, only 36% of uroflowmetry traces are correctly interpreted, with poor intra-observer agreement (41%). 12
Although notoriously inconsistent and subjective, more recently objective and quantitative approaches of interpreting uroflowmetry have been developed in children.13,14 The introduction of electromyography (EMG) and voiding lag time may further enhance the diagnostic capabilities of uroflowmetry. 15 Uroflowmetry devices have also been developed that can be used on normal toilets at the patient’s home and data uploaded via the cloud, for example, Homeflow (Minze Health, Belgium).
Review of modality: Conventional cystometrography studies
Traditional CMG usually requires the child to lay flat (although it may be performed in the seated or standing position) whilst the bladder is slowly filled with warmed fluid via a urethral catheter with a concurrent rectal catheter (and may include EMG surface electrodes). 16 The major advantage of invasive UDS is direct observation; it allows the practitioner to mark down events (such as coughing, crying, pain or the urge to void) and relate these to bladder activity. Additionally, as the bladder is emptied at the beginning of the study and artificially filled, accurate bladder volumes throughout the study are conferred.
In paediatric patients, the urethral catheter is placed through the external urethral sphincter. This could theoretically alter detrusor leak point pressure (DLPP). 11 In adults, the presumptive diagnosis based on patient reported symptoms and eventual CMG diagnosis showed poor concordance (19%–44%). 17 Moreover, artificial bladder filling can cause false impressions of incontinence due to over filling, rapid filling or filling with cold fluid and can trigger aberrant detrusor activity. 18
The hospital environment causes anxiety in young children, relating to a strange environment, instruments and equipment. 19 Crying and movement can cause artefact in the pressure transducers and EMG. Many children (60%) display at least one interfering behaviour during their first CMG. 20 Potentially interfering behaviours may include intense verbal/vocal distress, screaming, shouting, tensing of muscles, clenching, flinching or gritting or grinding of teeth. Definitively interfering behaviours include escaping, disrupting, avoiding or aggressing. 20
The exact role of CMG in the management of neurogenic bladder lacks consensus. This is despite many iterative historical studies that have proved and disproved the utility of early CMG, risk stratification based on outlet resistance/synergy of detrusor and sphincter and pro-active treatment of hypocompliance.21 –26 The ultimate goal of CMG in this context is to identify ‘dangerous’ or ‘high risk’ bladder dynamics that may ultimately put the upper urinary tract (and kidney function) at risk and require escalation of treatment. However, contemporary methods of CMG yield highly variable results. There was poor inter-rater reliability in diagnosing detrusor overactivity (Fleiss kappa 0.35). 27 However, the UMPIRE study group highlighted critical disparities in the risk categorisation of neurogenic bladder. When externally validated, only 50% agreement (79/157) was found with the initial local interpretation. 4 This may be due to differences in practise and technique, variations in the application of International Children’s Continence Society (ICCS) definitions and guidelines, and a general lack of consensus on what constitutes a ‘dangerous bladder’. More recently, studies on CMG have focused on analysing new metrics such as work (PAUC, pressure-adjusted area under the curve). PAUC captures a richer data outcome from CMG studies, formulated from the ratio of area under the cystometry curve to a DLPP-adjusted total area. 28 This was shown to be more predictive of upper tract changes and acquired kidney damage than more traditional metrics such as DLPP and compliance. 28
CMG studies cause physical and emotional distress to both children and their guardians. Finkelstein et al. reported a significantly elevated mean patient anxiety score prior to CMG (compared to afterwards) in children over 5 years old. This highlights that the anticipation of the study itself was anxiety provoking. One of the most distressing steps was urethral catheterisation. 16
By combining traditional urodynamics with fluoroscopic imaging, video-CMG allows for dynamic assessment of the urological tract during bladder filling and emptying.29,30 The added financial cost, availability and radiation exposure must be considered. Overall, fluoroscopy exposure time and effective radiation dose is less than a micturating cystourethrogram.31,32 Direct financial costs of video-CMG have never been published. 33
Review of modality: Ambulatory urodynamics through catheter devices
The introduction of AUM allows for physiological, antegrade bladder filling and enables the child to perform normal activities with catheters in situ. AUM enables the observation of ‘real life’ triggers in the child’s usual environment to be observed and documented (e.g. giggle incontinence, physical activities, temperature changes), without the requirement for a practitioner to be present (Figure 1). The drawbacks of AUM include its reliance on traditional catheters and pressure transducers, and the inability to continuously and accurately monitor bladder volumes. Moreover, the accuracy of the data is reliant on patient reporting which may produce misleading results. 32 The cost of AUM is likely to be higher than traditional UDS, 34 although no formal economic or cost–benefit analysis are available for either modality.

Ambulatory urodynamic tracing in an 8-year-old child that confirms that detrusor pressure stays close to baseline albeit with phasic detrusor overactivity. This child was known to have poor compliance on CMG.
AUM allows for longer data recording sessions, which may be advantageous yet also burdensome, as hours of UDS traces are accrued without labelled event markers. These needs to be reviewed and interpreted (similar to 24-h telemetry). Embracing machine learning algorithms may overcome the problem of data smog. Hobbs et al. detected detrusor overactivity using machine learning with good sensitivity (84%) and specificity (86%). 35
There is an emerging full spectrum of novel technologies that are moving towards at-home UDS. These less-invasive diagnostics will not necessarily need to replace their counterparts (or provide equal or superior diagnostic accuracy). The priority will be to develop modalities that are as accurate as current invasive methods, or spare sub-groups of patients invasive CMG by early and accurate triaging early in the treatment pathway. 36
The ICCS notes that currently AUM is not widely utilised in children, and furthermore, may be time-consuming and impractical in most centres. 16 However, the period of data recording can be optimised to address the specific urodynamic question posed. For example, if the question is around the safety of the bladder during its storage phase, three-four cycles (recorded over 8–12 h) may suffice. However, if the intent is to understand the cause of urinary incontinence, and this only occurs once a day, then 48 h may be required. Notably, AUM does not increase diagnostic specificity when compared to traditional CMG in adult women with bladder symptoms. 37 Disadvantages of AUM include catheter displacement and potential power failures. Setting the sensitivity of the sensors is problematic, specifically balancing the detection of clinically significant events and excessive artefactual activity. Increased utilisation of AUM may define more precisely a host of sub-clinical dysfunctional bladder disorders 38 or may call into question our concept of bladder compliance altogether. 34 Bladder compliance is defined as the change in bladder volume divided by the change in passive detrusor pressure and has been suggested to be an artefactual measurement by authors that have studied ambulatory studies in some detail. 16
Yeung et al. have utilised natural filling urodynamics by incorporating infrared relay technology. This allows for the child to play within a cubical whilst the practitioner makes observations remotely. The infrared system provided reliable and effective continuous ambulatory urodynamic monitoring. When compared with conventional CMG, natural-fill infrared telemetry detected a lower pressure rise with filling (13 cmH2O vs 8 cmH2O, respectively, p < 0.01). 39 A lower pressure rise is a ‘better result’, but the ultimate goal is to detect a clinically relevant phenomenon (that portends a poorer prognosis and requires treatment). It is unclear if either of these modalities (or in fact both) are more prognostic.
AUM relies heavily on patient participation in event recording, as the child is not observed by the practitioner. The use of event recording devices worn by the child can overcome event-labelling challenges. Deshpande et al. studied a portable, Bluetooth-enabled device LUNA™ (Medical Measurement Systems, Gladbeck, Germany), which was linked to a Bluetooth-enabled uroflowmeter and a digital event diary. Each period of observation lasted 24 h and pressure tracings were monitored every 3 h. The study diagnosed detrusor overactivity (DO) in 86% more children than conventional UDS. Eight children were treated based on these results, and 63% showed clinical improvement through therapeutic strategies based on the ambulatory UDS findings. 34 The pressure rise seen in poorly compliant bladders during invasive CMG was not observed during ambulatory UDS. 34 Instead, it is replaced by phasic detrusor overactivity. The voiding pressures during ambulatory UDS are also reported to be higher than during conventional UDS in both, adults and children. 34 These discrepancies are difficult to contextualise in the current paradigm. Are the properties we see in ‘high-risk’ bladders during invasive CMG (e.g. hypocompliance) a product of the way the investigation is conducted? Even if this is the case, it remains illustrative of a property intrinsic to certain bladder types. Is it indicative of phasic detrusor overactivity in a more physiological scenario? These questions will require clarification with time.
Bioimpedance techniques and near-infrared spectroscopy have been trialled; however, have been limited by poor accuracy of measurements, motion artefact and variable urine-dependent properties. Near-infrared spectroscopy also assumes that the optical and electrical properties of pelvic organs are constant, and that measured variations relate the bladder filling.40 –42 The use of ultrasound bladder vibrometry has been investigated as a non-invasive method to detect DO. In a pilot study, DO was detected from timestamped urodynamic bladder volume (UBV) measurements, (70% sensitivity and 75% specificity). Further refinement to this experimental setup (including dense and regular temporal sampling) is likely to enhance its non-invasive detection capabilities. 43 The study’s substantial limitation lies in the irregular and relatively large sampling intervals between UBV measurements, leading to episodic and irregularly sampled data, potentially contributing to false positives and false negatives. 43
Wearable bladder technology which is currently available includes SENS-U kids (Novioscan, Nijmegen, The Netherlands) and DFree (Triple W, CA, USA). In a paediatric study, the SENS-U kids wearable bladder scanner (Figure 2) successfully detected a full bladder in 90% of the study population. 44 There are no studies piloting the use of DFree in children. However, these devices measure bladder length not volume. The recognised error rate of current bladder ultrasound techniques is 14%–22%, highlighting the need for improvement. 45

SENS-U kids wearable bladder scanner.
Accuracy of bladder ultrasound techniques may be improved by integrating machine learning algorithms, multiple observation points (probes) and real-time monitoring. Additionally, standardising protocols, enhancing software tools may further reduce error rates. For example, traditional bladder volume measurement utilises maximum dimensions in three planes and approximates to the shape of a sphere to estimate volume. This technique of bladder volume assessment is known to introduce errors, as bladder shape in children may be round, ellipsoid, cuboid, triangular or undefined. 46 Spherical volume approximation can introduce errors of 10%–15%, and this error increases with smaller bladders. 47 By increasing the number of probes and/or coordinates measured a more accurate and individualised model may be used. 48
Paediatric patients with neurogenic bladder develop abnormalities in detrusor smooth muscle, which lead to decreased elasticity and poor compliance detectable via elastography. Ultrasound shear wave elastography (US + SWE) effectively predicts detrusor overactivity and hypocompliance with a specificity of 83% (p < 0.05). 49 Colour Doppler, used with the Bernoulli effect, identifies bladder outlet obstruction in adults. 50 Recent research shows that even optimised ultrasound models have low predictive value for kidney anomalies or vesicoureteric reflux (VUR) in children post-febrile UTI, especially in those with neurogenic bladders, where VUR correlates with kidney cortical loss. 51
A study on home-monitoring of bladder pressure to improve management of children with neurogenic dysfunction on clean intermittent catheterisation (Figure 3) found most families easily learn to record pressures and volumes at home. Comparing home-based measurements with the current gold standard (traditional CMG) was favourable (100% sensitivity and 80% specificity). Maximal bladder pressures >20 cmH2O measured at home were most sensitive for predicting high detrusor pressures on CMG and hydronephrosis (SFU grade 3–4).52,53 Involvement of families can be hugely empowering, reduce anxiety and provide comfort, and lead to improved therapeutic alliances.
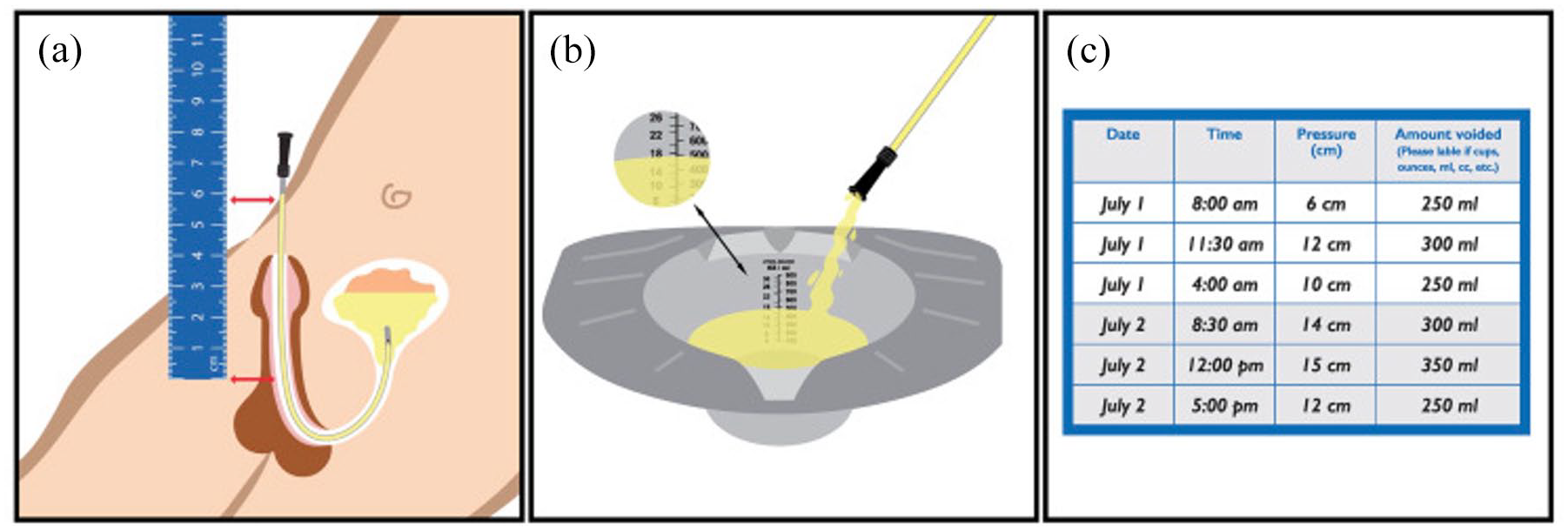
Adapted illustration of home bladder pressure and volume measurements in a male patient. 53
Review of modality: Telemetric ambulatory urodynamic monitoring through implantable devices
Telemetric ambulatory urodynamic monitoring (TAUM) utilises catheter-free technology. These systems can be wireless or wired, battery-powered or externally charged and can store data on board or transmit data to a receiver. TAUM devices are inserted transurethrally or surgically, 8 either as an intravesical, intradetrusor or transdetrusor device. Fifteen distinct catheter-free pressure sensors have been developed over the past 20 years. 54
Intravesical TAUM devices (Figure 4) are designed to float in the bladder lumen, and although they are the least invasive of the TAUM devices 54 they can theoretically be expelled during voiding or cause outlet obstruction. They are made of a vacuum-sealed chamber with a suspended silicone membrane and transducer. The transducer measures pressure differences relative to the vacuum-filled chamber. Currently, the devices used are intended for insertion through an adult cystoscope. These devices have diameters ranging from 15 to 21 French (Fr). Devices intended for surgical insertion can be as large as 48 Fr. 45 These devices are likely to be engineered with the adult patient in mind, and there are important differences in patient and pathology when applying them to children. Insertion may be more challenging and have a different complication profile. Current magnetic techniques used to aid insertion and removal of stents in the paediatric population 55 could be adapted to aid TAUM insertion and retrieval. Current intravesical devices vary in accuracy, data resolution and sampling rates. Intravesical devices producing pressure measurements with an accuracy of ±2.5 cmH2O are considered sufficient for TAUM. There are solitary examples of pilots in humans indicating that this type of medical device is on the doorstep of clinical practice, but most pilots have been in animal models (porcine). 56 Bench testing of the ‘Bladder Pill’ demonstrated agreement of pressure measurement with catheter-based methods (a difference of 0.3 cmH2O). 57 Data sampling rates range from 0.5 Hz (one reading every 2 s) for capturing of rapid physiological changes, to 0.003 Hz (one reading every 5 min) for monitoring over extended periods. Sampling rates can be adjusted based on the clinical question, for example, determining the safety of bladder storage would require less-frequent observation points.

The bladder pill, an implantable TAUM, that floats within the bladder lumen.
The capability for onboard data storage and transmission is indeed an advantage of Telemetric AUM (automated urodynamic monitoring). This feature facilitates continuous data collection without the need for proximity to a data hub, enhancing patient comfort and compliance. It also enables real-time remote monitoring and timely interventions, potentially improving clinical outcomes.
Intravesical devices allow for onboard data storage and transmission of data, facilitating continuous data collection without requiring the patient to be physically present. Allowing for at home testing may enhance patient comfort and provide more representative results. Down-sizing for the paediatric population has not yet been explored. However, modifications must ensure that the device is small enough to fit through a paediatric cystoscope, and after insertion not occlude the urethra/bladder neck or occupying the entire bladder.
Intradetrusor TAUM devices are inserted via cystoscopy by raising a flap of urothelium and lamina propria and can also be implanted surgically. Since the devices are not exposed to urine, they are protected from becoming encrusted or eroded.58,59 However, the difficulty in creating a device that is small enough to insert through a paediatric cystoscope, yet powerful enough to communicate results, is a major challenge. Moreover, the risk of erosion of the sensor through the detrusor muscle into the bladder lumen or perivesical space has been demonstrated in animal models. 58 Studies in animal models have shown that by 4 weeks the devices were either in the bladder lumen or expelled. Most non-invasive UDS studies in children last no more than 48 hours so this may not be a clinical problem, so long as the device does not expel or erode differently in humans. Currently, intravesical and intradetrusor TAUM devices do not measure intra-abdominal pressure and are subject to artefact. Data processing algorithms have overcome this challenge with 97% improvement in detection accuracy, producing results comparable to catheter-based CMG. 60 If the need for a separate abdominal sensor can be eliminated from clinical practice, the scope for smaller TAUM devices is feasible.
Transdetrusor TAUM devices can be inserted through the abdominal wall under ultrasound guidance. They traverse the entirety of the bladder wall and enter the bladder lumen to measure intravesical pressure directly and concurrently measure abdominal pressure with a second sensor. 58 Transdetrusor devices comprised an external, percutaneous component and an internal portion. Externalising the storage and battery component enables the internal portion to be downsized. Separating the TAUM into two parts allows for a larger external component carrying more storage and a long battery life. Current investigational devices are 4–14 Fr.58,61
Real-time data transmission is advantageous for research but requires external components and antennas near the implanted device. Current externally powered devices have functional distances of 2–12 cm. This functional distance makes application problematic in patients with obesity and may prevent testing in some children. 45
Embracing TAUM models of UDS allows for natural bladder filling and observation of everyday events, without the impedance of catheters, artificial environments and stressors associated with conventional studies. TAUM devices allow for prolonged data-recording and big data collection. However, some devices require a more invasive approach than catheter-based testing (e.g. intradetrusor and transdetrusor TAUM). The benefit of the prolonged data provided by TAUM devices must be weighed against the risks of surgical insertion, bleeding, infection and migration. Moreover, the insertion of TAUM devices would likely expose the child to a general anaesthetic for both insertion and removal. Both catheter-based UDS and TAUM require placement of foreign devices that may inherently cause bladder overactivity and false-positive results.
Discussion: advancements and challenges in urodynamic modalities
This article explores the strengths and weaknesses of various urodynamic modalities. Uroflowmetry, characterised by its non-invasiveness and cost-effectiveness, offers a practical diagnostic approach but grapples with issues of poor reproducibility and reliability. Traditional CMG despite its strengths has proved fallible as a gold standard test in children due to inherent challenges, frequent motion artefact, challenging behaviours and poor acceptance. It excels in directly measuring bladder volume and real-time artefact recording but faces challenges due to its invasive nature and artificial study environment. It has several acknowledged shortcomings: it is time-consuming and resource-intensive. It requires an experienced team, dedicated facilities and knowledge of the specific UDS question, and furthermore there are concerns regarding reproducibility and diagnostic failures.
Some of the most central features of CMG (e.g. compliance) have been recently called into question. Standard paediatric urodynamic practice is time-consuming and fraught with inaccuracy. Lack of universally applied parameters causes confusion; ultimately leading to inaccuracies and variability in results. Until the paediatric urologic community has a well-defined standard for technique and interpretation, it is critical that studies clearly describe how traditional CMG was performed, e.g. how parameters (e.g. detrusor sphincter dyssynergia) were measured, and how bladder hostility is defined. 63 The use of catheters is inherently problematic and can cause symptoms that may not occur at home (e.g. bladder irritation and muscarinic receptor-mediated involuntary contractions of bladder smooth muscle). 64 Improvements in current testing can be made by embracing technological advances and adapting to new methods of data collection. AUM and TAUM have the potential to improve diagnostic capability and positively impact the patient’s experience.
Ambulatory UDS utilise natural filling and extended observation. However, the invasive nature of this modality and difficulties in dynamic bladder volume assessment limit widespread use. Furthermore, interpretation is problematic as there is the possibility for un-labelled background artefact from the child moving around. This may also make interpretation of the study data challenging. Finally, as this is a novel study understanding what the study means in terms of prognosis remains unknown, for example, compliance may not be present to the extent that is seen in traditional CMG.
Wearable bladder technologies emerge as promising adjuncts for natural fill UDS, with success in pilot studies. Nevertheless, challenges such as sensor displacement, limited functionality in obese patients, and the need for improved accuracy warrant further refinement. Ultrasound technology is ubiquitous and modifications of current usage will likely be available shortly. Among these technologies, bioimpedance measurements show promise in accurately measuring bladder volume with an error rate of less than 5%.40,41 This accuracy is substantially higher than the current bladder ultrasound techniques, which have error rates between 14% and 22%. 45 Integrating machine learning algorithms and real-time monitoring can potentially enhance the accuracy of bladder ultrasound, suggesting a pivotal area for future research and development. In a pilot study, timestamped bladder volume measurements detected detrusor overactivity (DO) with a sensitivity of 0.7 and specificity of 0.75, indicating moderate accuracy. 43 These metrics highlight the need for further refinement to enhance non-invasive detection capabilities.
TAUM devices introduce prolonged data recording and avoid catheter impedance. However, these are still in the trial phase and are complex to insert, present challenges when applied to paediatric patients, and have the potential for foreign body-related complications. These challenges require ongoing resolution and validation. Moreover, TAUM requires a general anaesthetic for insertion which is not necessary for other modalities. Given the potential for infection and erosion through the bladder wall, further studies are required to determine the feasibility of TAUM in humans. The devices for paediatric UDS currently range in size from 15 to 21 French (Fr) for insertion through an adult cystoscope, and up to 48 Fr for surgical insertion. 45 The capability for onboard data storage and transmission is a significant advantage of TAUM, facilitating continuous data collection without the need for constant physical presence. This feature enhances patient comfort and compliance and enables real-time remote monitoring, potentially improving clinical outcomes. However, downsizing for the paediatric population needs exploration to ensure devices fit through paediatric cystoscopes without occupying the entire bladder.
Adequacy of data storage with decreased device size remains a concern. Furthermore, data processing algorithms have the potential to enhance data interpretation when this is vast and dense. 58 By embracing these algorithms, the difficulty of data overload may be mitigated. For example, a context aware thresholding algorithm has been developed to identify bladder contractions and distinguish these from abdominal pressure events using signal-processing methods in the absence of simultaneous abdominal pressure measurement from rectal or vaginal catheters. 64
The results of UDS guide treatment and may commit children to major surgical intervention and long-term morbidity. 7 Current management based on traditional CMG (the gold standard) may result in either under- or over-treatment as demonstrated by the disparities in categorisation in the UMPIRE study. 4 Accurately identifying the care necessary to protect future kidney function and facilitate social continence are the ultimate end-points of urodynamic-based risk stratification. It is therefore imperative that standardised, reliable and reproducible UDS testing is achieved. Table 1 presents a summary of the various current urodynamic study types with practical considerations, strengths and weaknesses. Table 2 presents the test properties for these study types.
Summary of the various urodynamic study types with practical considerations, strengths and weaknesses.

CMG, Cystometrography; DO, Detrusor overactivity; EMG, Electromyography; mins, minutes; hrs, hours; UDS, Urodynamic study; UTI, Urinary tract infection; y, year.
Summary of the test properties for various urodynamic study type in children.

Kappa result interpretation: 0.01–0.2 indicates none to slight agreement, 0.21–0.40 indicates fair agreement, 0.41–60 indicates moderate agreement, 0.61–0.8 indicates substantial agreement, 0.81–1.00 indicates almost perfect agreement.
Definitions in this study were as per the ICCS with bell-shaped curves regarded as normal, and all other subtypes as abnormal (e.g. interrupted, plateau, staccato, tower).
CMG, Cystometrography; UDS, Urodynamic study.
In the future, permanently implanted devices could facilitate patients with neurogenic bladders to monitor and control bladder pressures more tightly (like blood sugar levels in diabetic patients). Moreover, a potential major advantage of TAUM devices could be to inform patients in real-time when to perform catheterisation. This may involve mobile app alerts and gamifications to reduce parental burden and improve patient observance (particularly during adolescence). This has been well applied to the field or urotherapy, with user experience design.65,66 Exploring less-invasive options such as shear wave elastography or surrogate measures through algorithms may reduce or even eliminate the need for catheter-based testing.
Future research should focus on refining these technologies to enhance accuracy, safety and overall clinical utility.
Conclusion
Over the past two decades, there have been significant developments in paediatric urodynamic studies focusing on less-invasive monitoring devices, as well as re-defining normative values. Traditional urodynamic studies are performed in specialised suites in real-time with artificial bladder filling. Alternatively, ambulatory models allow for measurements in a more authentic environment and with natural bladder filling. Novel implanted telemetric monitoring devices provide a catheter-free solution but are inherently invasive in nature. Exploration of indirect measurements to obtain urodynamic data warrant further investigation. An innovative approach is needed to further advance urodynamic studies in the paediatric population, with direct and sustained efforts from both end-users and developers. This will require the paediatric urologist to be an active participant in advancing technology and maintaining standards as the paradigm shifts.