
Abstract
Background:
The Optilume® paclitaxel drug-coated balloon (DCB) is a relatively new-to-market alternative in the management of male anterior urethral stricture disease. The pivotal trial excluded patients with a history of urethroplasty, although these strictures may be amenable to endoscopic management. Therefore, we sought to assess the efficacy of the DCB in the management of recurrent strictures following urethroplasty.
Methods:
A retrospective, multi-institutional review of male patients undergoing DCB dilation from 1/1/2022 to 11/1/2023 by five surgeons at four institutions was performed. Patients were stratified by history of urethroplasty; demographics, stricture characteristics, and outcomes (surgical success, time to recurrence). Success was defined as freedom from re-intervention in patients with at least 3 months of follow-up.
Results:
Among the 122 cases assessed, 33 (27.0%) had previously undergone urethroplasty. Patients in the urethroplasty group were younger than those in the control group (51.6 vs 58.8 years, p = 0.022). The two groups were otherwise similar with regard to background characteristics and comorbidities. Patients in both groups had similar stricture characteristics with short bulbar strictures being the most common. When compared to the control group, those with a history of prior urethroplasty had a greater median number of interventions prior to DCB treatment (3 vs 1, p < 0.001). Postoperative cystoscopy was performed in 37 cases, with similar patency rates between groups (p > 0.999). Early success rates were similarly high in both groups (80.0% post-urethroplasty vs 88.9% control, p = 0.338), although follow-up was limited to a median of 3.5 months in the urethroplasty group and 2.9 months in the control group (p = 0.069).
Conclusion:
Despite a greater number of prior surgical interventions, patients with a history of urethroplasty achieve similarly high success rates after treatment with DCB compared to those without a history of urethroplasty.
Plain language summary
The Optilume drug coated balloon (DCB) is a dilating balloon coated in the medication paclitaxel, which helps to inhibit scar formation. It has recently been approved by the FDA to be used to treat men to have urethral stricture (scar tissue) disease. The initial studies did not include patients who had undergone surgical treatment via a urethroplasty in the past, and thus our goal was to assess how well this new technology performs in this setting. We looked at 122 patients who underwent treatment with the DCB, 33 of whom had undergone urethroplasty in the past and 89 who had not. The two groups were similar with regards to things like age, other medical problems, and the location and length of their stricture. We found that patients who had urethroplasty in the past did similarly well after dilation with the DCB: 80% of people in the urethroplasty group were successfully treated compared to 89% of those who had not had urethroplasty. One limitation of the study is that the follow-up is short; that is, patients have not been seen for a long time after surgery to make sure they are still doing well. Another is that there were relatively few patients considered. A strength of the study is that the study includes patients from different hospitals treated by different urologists which makes the results more likely to be applicable to the general population. This is an early study and we will need to continue to follow these patients over time to see how they do long-term.
Introduction
The Optilume® paclitaxel drug-coated balloon (DCB) system (Laborie Medical Technologies Corp., Portsmouth, NH) was granted Food and Drug Administration (FDA) approval in late 2021 for the management of male anterior urethral strictures. 1 The 2-year results of the ROBUST III trial comparing the safety and efficacy of the DCB system versus standard endoscopic management revealed a significant improvement in International Prostate Symptom Score, Qmax, post-void residual, and freedom from reintervention in the treatment arm. 2 These results were maintained over the follow-up period. Additional follow-up is planned to extend out to 5 years. Notable exclusion criteria from the ROBUST III included men with complex etiology including lichen sclerosis, history of hypospadias repair, and prior urethroplasty. Prior pelvic radiation was an exclusion criterion in the ROBUST I study 3 but not the ROBUST III study. 2 Given the challenges of repeat urethroplasty, options for more effective endoscopic management are enticing. We thus sought to assess the efficacy of the DCB in the management of urethral strictures in those with a history of urethroplasty.
Methods
Study design
A multi-institutional retrospective review of male patients who underwent Optilume DCB dilation from 1/1/2022 to 11/1/2023 was performed. Each institution obtained institutional review board approval; studies were as follows: STU-2019-1454 (UT Southwestern), 160822007 (University of Alabama), Pro00027075 (University of South Florida), and 00115897 (Atrium Health). Any patients who had posterior urethral strictures, prior DCB dilation, or a history of pelvic radiation were excluded. Patients were then stratified based on whether they had a history of urethroplasty. Surgeries were performed by five surgeons at four institutions.
Procedures
After a baseline urethrogram, patients underwent stricture pre-treatment at the discretion of the operating surgeon (direct vision internal urethrotomy vs dilation vs none). The diameter and length of DCB were chosen by the operating surgeon based on urethrogram characteristics. The DCB was advanced across the stricture and inflated to the rated burst pressure, where it was held for 5 min. Thereafter, the balloon was maximally deflated and removed, and a urethral catheter was passed into the bladder. Catheters remained in place for a median of 3 days postoperatively (IQR 2–4), based on clinic availability and surgeon discretion.
Data collection and endpoints
The two groups were compared with regard to demographics, comorbidities, and surgical history. Stricture characteristics (length, location, and etiology) were collected, as were the intraoperative details including the use of pre-dilation, DCB size, and catheter duration postoperatively. Outcomes included functional success—which was defined as lack of symptomatology and freedom from reintervention in patients who had at least 3 months of follow-up—and time to stricture recurrence.
Statistical analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences software package, version 24 (IBM Corporation, Armonk, NY). Shapiro–Wilk and Levene tests were used to assess normalcy and variance, respectively. Parametric, continuous variables were assessed with Student’s t-test, while nonparametric continuous variables were assessed with Mann–Whitney-U. Chi-squared and Fisher’s exact tests were used for categorical variables as indicated. A p-value of 0.05 was used to determine statistical significance.
Results
During the study period, 213 DCB dilations were performed at the four institutions, of which 91 were excluded (Figure 1). Of the remaining 122 cases, 33 (27.0%) had previously undergone urethroplasty while 89 (72.9%) had not and were utilized as controls. Patients in the urethroplasty group were younger than those in the control group (51.6 vs 58.8 years, p = 0.022). The two groups were otherwise similar with regard to background characteristics (Table 1).

Study inclusion/exclusion flowsheet.
Patient and stricture background characteristics.
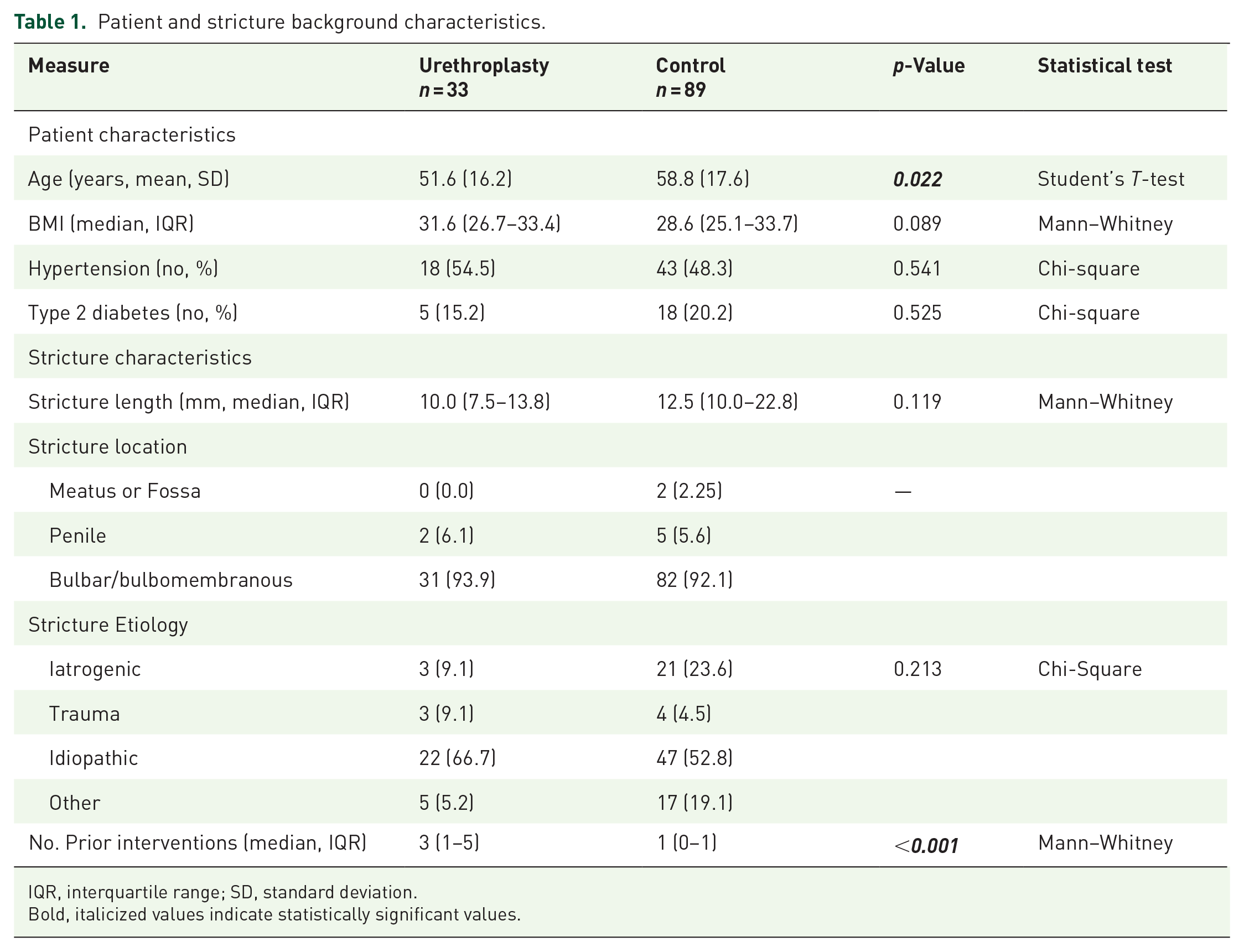
IQR, interquartile range; SD, standard deviation.
Bold, italicized values indicate statistically significant values.
Most patients had short strictures; the median stricture length in the urethroplasty group was 10.0 mm (IQR 7.5–13.8) while that in the control group was 12.5 mm (10.0–22.8, p = 0.119, Table 1). Strictures in both groups overwhelmingly involved the bulbomembranous urethra (31/33 patients in the urethroplasty group and 82/89 patients in the control group). Over half of the strictures in each group were idiopathic in nature, with no significant difference in stricture etiology between the two groups. Those with a history of prior urethroplasty had undergone a median of 3.0 interventions prior to undergoing DCB dilation (IQR 1.0–5.0) versus only 1.0 interventions (IQR 0.0–1.0) in the control group (p < 0.001).
With regard to operative characteristics, a similar number of patients in each group underwent pre-dilation (66.7% in the urethroplasty group vs 66.3% in the control group, respectively; p = 0.969, Table 2). Nearly all patients in both groups were treated using the 30Fr DCB (33/33 in the urethroplasty group, 87/89 in the control group). There was no significant difference in postoperative catheter duration, with a median catheter duration of 3.0 days in both groups (p = 0.503). In those with at least 3 months of follow-up, functional success—defined as lack of obstructive symptoms and freedom from surgical re-intervention—was seen in 16/20 patients (80.0%) in the urethroplasty group and 40/45 patients (88.9%) in the control group (p = 0.338). The median follow-up duration was similar at 3.5 months (IQR 1.3–8) in the urethroplasty group and 2.9 months (IQR 0.0–4.7) in the control group, respectively (p = 0.069).
Operative characteristics and outcomes.

IQR, interquartile range; SD, standard deviation.
Discussion
The Optilume paclitaxel-coated balloon system is a promising, minimally invasive option for the management of recurrent anterior urethral stricture disease. Long-term data are limited given that the system only recently gained FDA approval in December 2021. 1 Moreover, the ROBUST III trial, the prospective, randomized, single-blind trial on which FDA approval was based, excluded patients with a history of urethroplasty. 4 Given the increased challenges of reoperative urethroplasties, the potential for an effective method of endoscopic management of recurrent stricture post-urethroplasty is enticing for patients and surgeons alike. To our knowledge, this study is the first to evaluate outcomes of Optilume DCB dilation for stricture recurrences after urethroplasty. Our early results suggest that patients with a history of urethroplasty appear to enjoy similarly high freedom from re-intervention to those without, at least after short-term follow-up. Time will tell if these results are maintained longer term.
Urethroplasty remains the gold standard for the management of anterior urethral stricture disease. A wide array of approaches are available, based on stricture location, etiology, severity, length, and surgeon preference. Long-term data suggest success rates of around 85%; however, recurrence is more likely in those with longer strictures, strictures in the penile urethra, and those with a history of pelvic radiation.5,6 Invariably, defining success is challenging given no universally accepted definition; some studies focus on freedom from re-intervention, while others focus on patency during cystoscopy, improvement in uroflowmetry parameters, or symptom improvement on patient-administered questionnaires.5,7,8
Management of failed urethroplasty
In some respects, it is easier to define urethroplasty failure; symptoms such as recurrent straining, incomplete emptying, or recurrent urinary tract infections mandate further workup with retrograde urethrography, cystoscopy, or both. When failure is confirmed by one of the above methods, management options include chronic indwelling catheter (urethral or suprapubic), intermittent self-catheterization, endoscopic management, re-do urethroplasty, or perineal urethrostomy.9–13 The choice of which option to pursue is nuanced, depending on the location and severity of the recurrent stricture and patient preference.
Traditional endoscopic management of recurrent urethral strictures, either via direct vision internal urethrotomy or axial urethral dilation, is appealing given its minimally invasive nature. These techniques may be appropriate to consider for short-segment recurrences anywhere in the anterior urethra. 9 It is well established that repeated attempts at traditional endoscopic management are ineffective in the initial stricture treatment course and accepted that after an initial failed attempt at endoscopic management, patients should undergo urethroplasty.10,14 Success rates for internal urethrotomy after urethroplasty failure are reported from 51.2% to 66.3% of cases over 1-year follow-up.6,9 Long-term (i.e., 5 and 10 years) results in this population are lacking; however, success rates do appear to drop with time. After 24-month follow-up, one study reported success rates for DVIU of only 35% after failed EPA urethroplasty and 27% after failed substitution urethroplasty. 15 Success rates may be higher when internal urethrotomy is combined with injection of mitomycin C and followed by a self-catheterization regimen; one study reported 12/15 (80.0%) of patients with bulbar strictures and 5/5 (100.0%) of those with penile strictures had no recurrence at 23-month follow-up. 16 However, these results must be tempered by the small sample size.
Repeat urethroplasty has been associated with high levels of success and improvement in patient-reported quality of life.12,17 One study found salvage excision and primary anastomosis of bulbar strictures were associated with a 95% success rate over a mean follow-up of 41.5 months. 12 This technique is not appropriate for longer strictures or those in the penile urethra, which may require the use of a fasciocutaneous flap, buccal mucosa graft, or other augmentation techniques. 17 Salvage penile urethroplasty is associated with lower success than bulbar urethroplasty, but success rates are still reported as high as 68.8%.11,17 For those with extensive recurrent stricture disease or those seeking more definitive management, perineal urethrostomy offers success rates as high as 95.1% with a median follow-up of 40 months.18,19 Despite some patients initially having hesitation regarding urinary diversion via perineal urethrostomy, this option has been associated with improved urinary function and quality of life. 20
A new treatment option
In December 2021, the Optilume DCB system was approved for the management of male urethral strictures. In contrast to other endoscopic stricture management options which only mechanically open the urethral lumen, the drug-coated balloon additionally delivers paclitaxel directly to the strictured area. 4 A microtubule inhibitor, paclitaxel directly inhibits cell proliferation and thus scar regrowth. 21 Early results of the ROBUST I and ROBUST III clinical trials have demonstrated a significant reduction in stricture recurrence in those men who have failed prior endoscopic intervention.2,3 Notably, both trials excluded those patients with a history of prior urethroplasty.
Our early results suggest that Optilume performs well in the post-urethroplasty population with failure only noted in 12.1% of patients over a median follow-up of 3.5 months. This was not significantly different from the 7.9% failure rate of the control group, and notably better than the failure rates of nearly 50% noted for traditional endoscopic management methods. 9 Patients undergoing Optilume post-urethroplasty had notably short strictures with a median length of only 1.0 cm and had undergone a median of three interventions for their stricture disease prior to Optilume dilation.
Given the limited follow-up, it will be necessary to continue following these patients over the coming years to better evaluate long-term efficacy. The most recent results of the ROBUST III trial reveal Kaplan–Meier point estimates for freedom from reintervention of 86.9% at 1 year and 78.5% at 2 years. It remains to be seen whether post-urethroplasty patients will enjoy similarly high success rates with more prolonged follow-up. Future prospective studies will answer this question more comprehensively but will likely be a few years away. Other challenging populations (i.e., those with penile, post-radiation, or vesicourethral anastomotic strictures) may also benefit from this treatment modality although this remains to be studied.
Limitations
This study is limited by its retrospective nature. Given the multi-institutional design, there was some heterogeneity between the sites with regard to practice patterns. For example, at some sites, all patients were pre-dilated with a non-drug-coated balloon prior to Optilume dilation; at others, no patients received pre-dilation. On a theoretical level, we would not expect a brief pre-dilation with a smaller-caliber balloon—the majority of pre-dilated patients are pre-dilated with 24Fr non-drug-coated balloon—to alter the functional success rate. We acknowledge this has yet to be proven and we expect this to be the subject of future studies. The choice of diameter and length of the Optilume balloon was made at the surgeon’s discretion. However, the vast majority of patients were dilated with a 30Fr drug-coated balloon.
We also recognize that the definition of success used in this study (lack of obstructive symptoms and no need for repeat intervention) is not as strong as some others. In the absence of symptom recurrence, we prefer to avoid the invasiveness and discomfort of urethral calibration using a catheter, and the additional financial burden to the patient of routine cystoscopy. While an attempt is made to obtain uroflowmetry studies at the 3-month visit, many patients void just prior to arrival, and it is (in our opinion) unnecessarily cumbersome on the clinic workflow to force patients to stay until flow studies can be performed.
These results may not be generalizable to all patients with recurrent stricture after urethroplasty. Given the nuance of urethral stricture disease, some strictures—such as those that are particularly long—may not be amenable to balloon dilation. Small sample size and short follow-up are expected limitations given the recent FDA approval of the drug-coated balloon system. As these patients are followed over the coming years, more insight will be gained regarding the durability of these early results. Even so, this study represents the first evaluation of this new endoscopic option for the management of recurrent strictures after urethroplasty failure and may help guide patient counseling.
Conclusion
Patients with a history of failed urethroplasty appear to achieve similarly high success rates for the management of recurrent urethral stricture using the Optilume drug-coated balloon system compared to those without a history of urethroplasty over short-term follow-up.