Impact of transperineal treatment planning biopsy for confirmation of candidacy for partial gland cryoablation
Hunter Hernandez, Kevin Pineault, Eli Rapoport, James Wysock
Department of Urology, NYU Grossman School of Medicine, New York, New York, USA
Introduction: Due to limitations in defining disease margin on MRI, partial gland prostate cryoablation (PGCA) often includes an estimated margin applied to the MR lesion boundary. Transperineal saturation biopsy (TPBx), offering the most accurate tissue assessment short of radical prostatectomy, may enhance this process by providing more detailed intraprostatic disease distribution and volume information. This study evaluates the impact of a pre-treatment TPBx on refinement of candidate selection for PGCA for men diagnosed with unilateral, biopsy confirmed, MR-visible intermediate risk prostate cancer on transrectal biopsy.
Methods: Retrospective review identified consecutive men diagnosed with unilateral MR-visible pT1c-pT2b, Gleason Grade (GG) 2/3 electing to pursue PGCA who underwent subsequent TPBx. TPBx was performed with 5mm template sampling according to Barzell’s Zones. Disease volume was assessed, and candidate failure rates were calculated. Candidate failure was defined as GG >3, stage pT2c, or disease within posterior midline zone. Logistic regressions were used to assess whether clinical factors (i.e., age, PSA, MRI lesion size/location and PI-RADS score, transrectal biopsy GG, contralateral GG=1 disease) predicted candidate failure. Two-sided hypothesis testing was conducted at an alpha of .05. All analyses were conducted using R, version 4.0.5.
Results: 105 men met inclusion criteria. TPBx identified 34 (32%) as candidate failures, of whom 3 (9%) upgraded to GG>3, 18 (53%) had clinically significant disease in the posterior midline zone, and 21 (62%) were upstaged to pT2c. Patient age, PSA, PI-RADS score, laterality of lesion, number of lesions, transrectal biopsy GG, and contralateral GG=1 disease were all not predictive of candidate failure. Only MRI lesion size (defined by largest diameter) was predictive of candidate failure (OR=1.14, 95% CI: 1.03-1.27).
Conclusions: Addition of a pre-treatment TPBx improves candidate selection of PGCA, identifying candidate failures in approximately one third of men with biopsy proven, MR visible GG 2/3 disease on diagnostic biopsy. Clinical features on MRI and TR biopsy did not perform well in predicting candidate failure on TPBx, suggesting that routine TPBx may be beneficial for optimal treatment selection and surgical planning.
Artificial Intelligence Interpretation of Stimulated Raman Histology Can Provide Near Real-Time Intraoperative Margin Assessment During Partial Gland Ablation of Prostate Cancer
Miles P. Mannas1,2, Fang-Ming Deng3, Adrian Ion-Margineanu4, Christian Freudiger4, James Wysock3, Daniel A. Orringer3, Samir S. Taneja3
1University of British Columbia, Vancouver, British Columbia, Canada, 2Vancouver Prostate Centre, Vancouver, British Columbia, Canada, 3NYU Langone Health, NYC, NY, USA, 4Invenio Imaging Inc, Santa Clara, CA, USA
Introduction: In field recurrence after partial gland ablation of prostate cancer (PCa) remains an ongoing concern. Stimulated Raman histology (SRH) is a novel microscopic technique allowing real time interpretation of label-free, high-resolution microscopic images of unprocessed tissue. We evaluated surgical team and AI interpretation of SRH for real-time pathologic feedback in the planning and treatment of PCa with partial gland cryosurgical ablation (PCGA).
Methods: 12 subjects underwent lesion directed prostate mapping biopsies during PGCA with 4-7 prostate biopsies from: tumor (1), 1cm margin from MRI lesion (2), and treatment margin during PGCA (1-4). Biopsies were immediately scanned in a SRH microscope using two Raman shifts. Real time image interpretation was performed by the surgical team. An Inception-ResNet-v2 convolutional neural network (CNN) was used to interpret prostate biopsy SRH to assign a diagnosis: benign or PCa. The cores were processed and H&E-stained as per normal pathologic protocols and used for ground truth pathologic assessment. Change in treatment and diagnostic accuracy for detection of PCa on SRH relative to final pathology was tested for both the surgical team and CNN interpretation.
Results: Surgical team procedural interpretation of SRH revealed a 98.1% accuracy, 100% sensitivity, and 97.3% specificity for identification of PCa. CNN interpretation of SRH revealed identical results to the surgical team for identification of Gleason grade group >1 PCa. When considering any PCa, the diagnostic characteristics of the CNN showed an accuracy of 94.6%, 88.2% sensitivity and 97.4% specificity. SRH interpreted by the surgical team resulted in 3 subjects’ treatment modification after PCa was visualized lateral to an expected MRI predicted tumor margin or at an untreated cryosurgical margin, example shown in Figure 1.
Samples 1-5 represent stimulated Raman histology (SRH) of fresh prostate mapping biopsies obtained during focal cryosurgical ablation of prostate cancer (PCa). Samples A represent SRH, while samples B represent SRH with artificial intelligence color overlay (red indicates possible area of tumor, green benign and purple low quality or non-tissue). Percentages under each image represent the AI tumor prediction. All diagnosis were confirmed on the samples after routine processing, hematoxylin and eosin staining +/- immunohistochemistry, and genitourinary pathologist interpretation. Prostate biopsies 1 and 2 were taken 1cm from the margin predicted by pre-operative magnetic resonance imaging; sample 1 and 2 show Gleason grade group (GGG) 1 and 2 PCa, respectively. Sample 3 of a prostate biopsy obtained from subject’s MRI identified tumor shows GGG2 PCa. With PCa identified lateral to the 1cm expected PCa margin, the treatment zone was widened. Finally, prostate biopsies 4 and 5 were obtained lateral to the cryosurgical treatment zone and show benign prostate tissue.
Conclusion: SRH interpreted by both a surgical team and artificial intelligence can improve tumor modeling, beyond MRI and biopsy findings, during the conduct of PCa PGCA, resulting in real-time margin adjustment to maximize tumor destruction. Further testing is required to assess the effects on oncologic outcomes.
Disclosures: Miles P Mannas holds grant funding from the province of British Columbia and the Canadian Urologic Association to investigate stimulated Raman spectroscopy for prostate cancer. Christian Freudiger is an employee, shareholder, director of Invenio Imaging and hold patents on stimulated Raman spectroscopic microscopy that are independently licensed. Daniel A Orringer is a medical advisor and shareholder of Invenio Imaging, who also holds an RO-1 grant to investigate stimulated Raman spectroscopy. Steve Pastore is an employee and shareholder of Invenio Imaging. Adrian Ion-Margineanu is a shareholder of Invenio Imaging.
Focal therapy versus radical prostatectomy and external beam radiotherapy as primary treatment options for non-metastatic prostate cancer: results of a cost-effectiveness analysis
Deepika Reddy1, Marieke van Son2, Max Peters2, Mariana Bertoncelli Tanaka3, Tim Dudderidge4, Emma Cullen1, Carmen Lok Tung Ho1, Richard G Hindley5,6, Amr Emara5, Stuart McCracken7, Clement Orczyk8, Iqbal Shergill9, Stephen Mangar3, Raj Nigam10,11, Jaspal Virdi12, Caroline M Moore8,13,14, Manit Arya3,8, Taimur T Shah1,3,Mathias Winkler1,3, Mark Emberton8,13,14, Alison Falconer3, Jonathan Belsey15, Hashim U Ahmed1,3, 14, 16
1Imperial College, London, UK, 2Amsterdam University Medical Centers, The Netherlands, 3Imperial College NHS Healthcare Trust, London, UK, 4University Hospital Southampton NHS Trust, Southampton, UK, 5Hampshire Hospitals NHS Foundation Trust, UK, 6BMI The Hampshire Clinic, Basingstoke, UK, 7Sunderland Royal Hospital, Sunderland, UK, 8University College London NHS Foundation Trust, London, UK, 9Wrexham Maelor Hospital, Wrexham, UK, 10Royal Surrey NHS Foundation Trust, Guildford, UK, 11BMI Mount Alvernia Hospital, Guildford, UK, 12Princess Alexandra Hospital NHS Trust, Harlow, UK, 13Princess Grace Hospital, London, UK, 14King Edward VII Hospital, London, UK, 15JB Medical Limited, Sudbury, UK, 16Cromwell Hospital, UK
Aims: Focal therapy treats individual areas of tumour in non-metastatic prostate cancer in patients unsuitable for active surveillance. The aim of this work was to evaluate the cost-effectiveness of focal therapy versus prostatectomy and external beam radiotherapy (EBRT).
Materials and methods: A Markov cohort health state transition model with four health states (stable disease, local recurrence, metastatic disease and death) was created, evaluating costs and utilities over a 10-year time horizon for patients diagnosed with non-metastatic prostate cancer. National Health Service (NHS) for England perspective was used, based on direct healthcare costs. Clinical transition probabilities were derived from prostate cancer registries in patients undergoing radical prostatectomy, EBRT and focal therapy using cryotherapy (Boston Scientific) or high-intensity focused ultrasound (HIFU) (Sonablate). Propensity score matching was used to ensure at-risk populations were comparable. Variables included age, prostate-specific antigen (PSA), International Society of Urological Pathology (ISUP) grade group, maximum cancer core length (mm), T-stage and year of treatment.
Results: Focal therapy was associated with a lower overall cost and higher quality adjusted life year (QALY) gains than either prostatectomy or EBRT, dominating both treatment strategies. Positive incremental net monetary benefit (NMB) values confirm focal therapy as cost effective versus the alternatives at a willingness to pay (WTP) threshold of £30,000/QALY. One-way deterministic sensitivity analyses revealed consistent results.
Limitations: Data used to calculate the transition probabilities were derived from a limited number of hospitals meaning that other potential treatment options were excluded. Limited data were available on later outcomes and none on quality of life data, therefore, literature-based estimates were used.
Conclusions: Cost-effectiveness modelling demonstrates use of focal therapy (cryotherapy or HIFU) is associated with greater QALY gains at a lower overall cost than either radical prostatectomy or EBRT, representing good value for money in the NHS.
Prostate Biopsy Cores with SmartBxTM Downloading System Have Improved Core Length and Integrity Versus Standard Downloading
Jamie S. Pak, Fang-Ming Deng, James S. Wysock
NYU Langone Medical Center, New York, New York, USA
Introduction: During prostate biopsies, the handling of the cores from the biopsy needle to pathologic examination is critical in preserving the quality of the specimens. The standard handling of the cores is prone to loss of tissue length, fragmentation, and loss of tissue orientation. With the advancement of active surveillance and image-guided focal therapy, these biopsy core parameters may be critical to the individualized management of prostate cancer. A novel biopsy core downloading system (SmartBxTM, UC-Care, Israel) utilizes a cassette designed to preserve core length and integrity, and prior studies have suggested that SmartBxTM leads to higher cancer detection rates. We hypothesize that biopsy cores handled with the SmartBxTM system have longer core length on pathology slides, lower fragmentation rates, and higher percentage of orientable cores compared to cores handled by standard procedure.
Methods: This is a retrospective analysis of all patients who underwent prostate biopsies utilizing the SmartBxTM system from June 2021 to August 2022. Patients with SmartBxTM utilized for at least one biopsy core were included in this study. All prostate biopsies were performed by one fellowship-trained urologic oncologist. Outcomes of interest included core length on pathology slides, core fragmentation rate, and percentage of orientable cores. Core fragmentation was defined as a gap in the core present at all slices in a slide. Cores were considered orientable if the two ends of the biopsy core maintained polarity. Chi-squared analysis and t-tests were performed.
Results: A total of 14 patients underwent prostate biopsy with at least one core utilizing the SmartBxTM system: 10 patients had only SmartBxTM cores and 4 patients had both SmartBxTM and standard cores. Median age at biopsy was 65.9 years (IQR 62.8-70.3) and median PSA was 4.9 ng/mL (IQR 4.3-7.2). Of the 14 patients, there were a total of 425 SmartBxTM cores and 79 standard cores. The average slide core lengths were 1.25 cm and 0.96 cm for SmartBxTM and standard biopsy cores, respectively (p<0.001). The rates of fragmentation were 12% (53/425) in SmartBxTM cores and 32% (25/79) in standard cores (p<0.001). The percentages of orientable cores were 100% (425/425) in SmartBxTM cores and 59% (47/79) in standard cores (p<0.001).
Conclusions: The SmartBxTM biopsy core downloading system was associated with longer slide core length, lower rates of core fragmentation, and higher rates of orientable cores versus standard protocol. These results support the utility of SmartBxTM in preserving the quality of prostate biopsy core specimens.
Ezequiel Becher, Hernando Rios Pita, Victor Chernobilsky, Edgardo F Becher, Luis Montes de Oca, Marcelo Borghi
CDU – Centro de Urología, Buenos Aires, Argentina
Introduction and Objective: The objective of this study is to report the oncologic, perioperative, and functional outcomes of a men treated with salvage high-intensity focused ultrasound (sHIFU) hemi-ablation for radiorecurrent prostate cancer (PCa).
Methods: Our prospectively maintained HIFU outcomes registry was queried. Inclusion criteria were: history of radiotherapy, prostate anteroposterior length ⩽4cm, and no extra-prostatic disease. All patients were treated using the Sonablate system, and urethral-sparing techniques. Follow-up included PSA every 3 months for the first two years and then biannually, multi-parametric MRI at day 7 and month 6 followed by a biopsy. Choline or (later) PSMA PET was also warranted for concerning PSA kinetics. Postoperative complications were assessed using Dindo-Clavien classification.Failure was defined as a positive follow-up biopsy or progression to metastatic disease, and clinically significant PCa (csPCa) was defined as Gleason grade (GG)⩾2.
Results: From January 2010 to July 2022, 151 patients underwent sHIFU at our institution. Median Age was 72 years (IQR: 71-77). Oncologic, and perioperative outcomes are shown on Table 1. Median follow-up was 32 months with 50% of patients having no disease upon biopsy. Even though 23 patients refused a repeat biopsy, 78% of them remain free from biochemical recurrence. Six out of 15 patients undergoing repeat sHIFU remain free from biochemical recurrence. Of those recurring after repeat sHIFU, only two developed metastases and five were started on androgen depravation therapy (ADT). The remaining are still on surveillance.ADT or whole gland treatment was safely spared on 125 men.
Conclusions: sHIFU is a safe alternative for select patients with localized radiorecurrent PCa. This treatment modality has allowed most of our patients to delay their initiation of ADT, and has even rendered many disease free. It has an acceptable toxicity profile and very low peri-operative morbidity. Further prospective trials are warranted to validate these results.
Oncologic and perioperative outcomes of sHIFU (n: 151).
Salvage Seminal Vesicle Ablation with High-Intensity Focused Ultrasound for Radiorecurrent Prostate Cancer
Ezequiel Becher, Hernando Rios Pita, Victor Chernobilsky, Edgardo F Becher, Luis Montes de Oca, Marcelo Borghi
CDU – Centro de Urología, Buenos Aires, Argentina
Introduction and Objective: The objective of this study is to report the oncologic, perioperative, and functional outcomes of a cohort of men treated with salvage seminal vesicle (SV) high-intensity focused ultrasound (sSV-HIFU) for radiorecurrent prostate cancer (PCa) in the SV.
Methods: A prospectively maintained outcomes registry was queried for patients who underwent sSV-HIFU. Patients with biochemical recurrence were evaluated with CT, multi-parametric magnetic resonance imaging (mpMRI), and Tc99 bone scan to rule out extra prostatic disease. F18 Choline PET was also used in the later patients of the cohort.Patients with suspicion for SV recurrence were biopsied in a transrectal fashion. The SV suspicious for recurrence was biopsied every 5mm to map the extent of disease. A 12-core systematic biopsy and of the contralateral SV were also obtained. Treatment plan included a 5mm margin (distal to the SV and to the prostatic base).Follow-up was done with PSA every 3 months for the first two years and then biannually, mpMRI at day 7 and month 6 followed by a biopsy. IPSS and IIEF-6 questionnaires were filled-out at baseline and in every visit. Postoperative complications were scored using the Dindo- Clavien classification. Failure was defined as a positive biopsy or progression to metastatic disease.
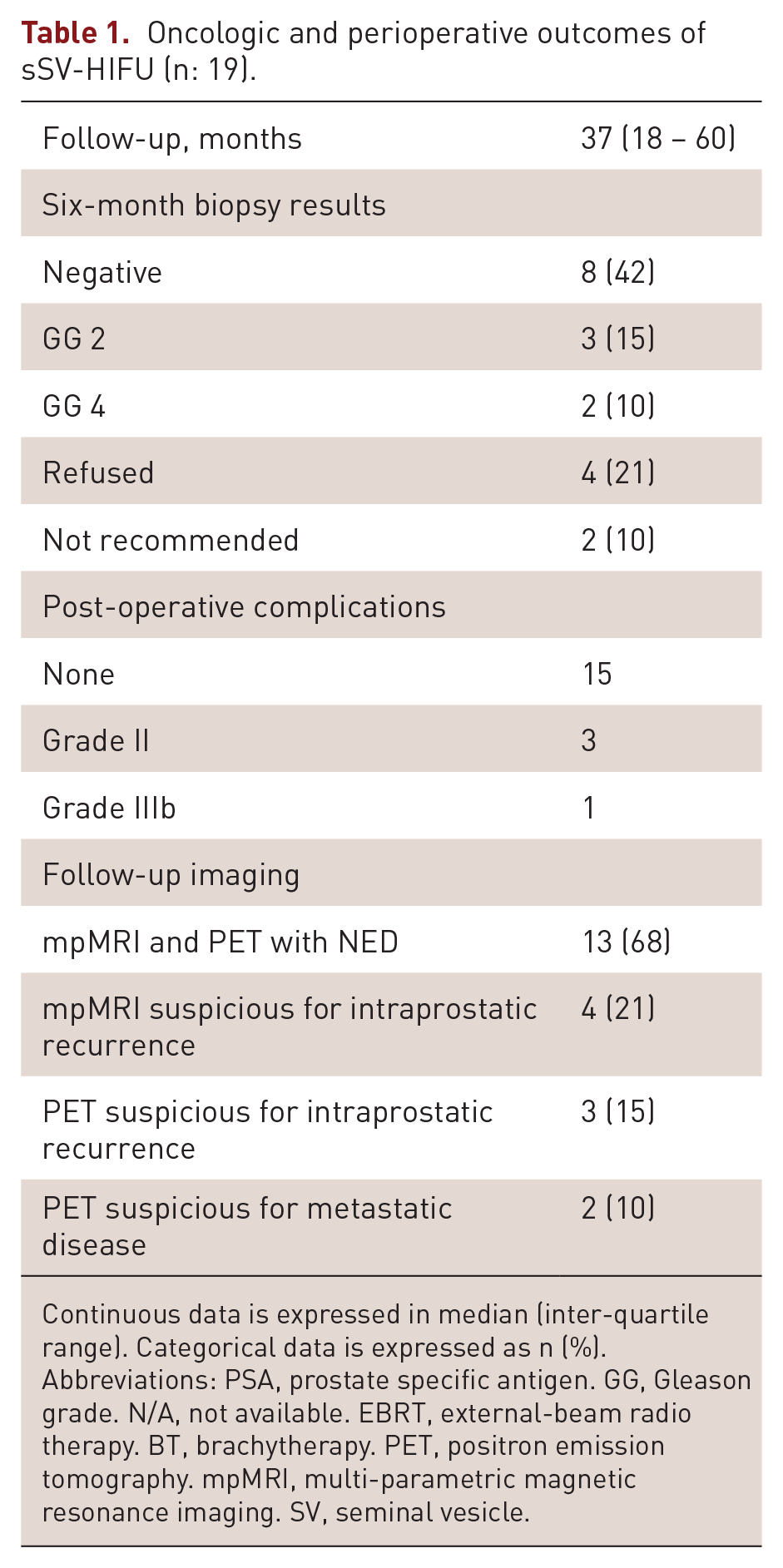
Results: From May 2016 to July 2021, 19 patients underwent sSV-HIFU. Median age was 70 years (IQR: 61-80). Median PSA was 6.4 ng/ml (IQR: 4.1 – 11). SV ablation + 5mm base margin was done on 10 patients, and an ipsilateral ablation was added on 9 patients. Procedure outcomes are shown on Table 1. Five patients refused the follow-up biopsy due to favorable PSA response, and one was not biopsied due to finding of metastatic disease. Salvage radical prostatectomy was performed in 2 / 3 patients with positive biopsy. Both of them progressed rapidly to metastatic disease. Full continence was maintained in 88% of patients, and 83% did not show a decrease in IIEF-6 score.
Conclusions: sSV-HIFU is a safe alternative treatment for select patients with localized radiorecurrent PCa that enables a delay in the initiation of androgen depravation. Further trials are warranted to validate these results.
Oncologic and perioperative outcomes of sSV-HIFU (n: 19).
Follow-up, months
37 (18 – 60)
Six-month biopsy results
Negative
8 (42)
GG 2
3 (15)
GG 4
2 (10)
Refused
4 (21)
Not recommended
2 (10)
Post-operative complications
None
15
Grade II
3
Grade IIIb
1
Follow-up imaging
mpMRI and PET with NED
13 (68)
mpMRI suspicious for intraprostatic recurrence
4 (21)
PET suspicious for intraprostatic recurrence
3 (15)
PET suspicious for metastatic disease
2 (10)
Continuous data is expressed in median (inter-quartile range). Categorical data is expressed as n (%).
Abbreviations: PSA, prostate specific antigen. GG, Gleason grade. N/A, not available. EBRT, external-beam radio therapy. BT, brachytherapy. PET, positron emission tomography. mpMRI, multi-parametric magnetic resonance imaging. SV, seminal vesicle.
Oncologic Outcomes of Partial Gland Ablation using Focal Intensity Focused Ultrasound after Additional Confirmatory Transperineal Mapping Biopsy in Men with Prostate Cancer
Wan Song and Hyun Moo Lee
Department of Urology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Introduction: Partial gland ablation (PGA) using focal intensity-focused ultrasound (HIFU) is a treatment option for localized prostate cancer (PCa). Accurate localization of PCa is important for improving oncologic outcomes. Transperineal mapping biopsy (TPMB) is useful for the diagnosis and management of PCa because it enables the detection of PCa by 30% compared to transrectal ultrasound (TRUS)-guided biopsy. Therefore, in this study, we evaluated the oncological outcomes of PGA using HIFU after additional TPMB in men with localized PCa.
Materials and Methods: We retrospectively reviewed patients with PCa who underwent PGA using HIFU between January 2020 and June 2022. After multiparametric magnetic resonance imaging (mpMRI), all men underwent TRUS-guided, cognitive-targeted biopsy and systemic biopsy. For men eligible for PGA using HIFU, confirmatory TPMB was additionally performed. After PGA using HIFU, prostate-specific antigen (PSA) level was checked every 3 months, and mpMRI and TRUS-guided biopsy were performed 1 year after PGA using HIFU. The change in treatment plan after confirmatory TPMB was analyzed, and the results of 1-year follow-up biopsy after PGA using HIFU were evaluated.
Results: A total of 96 patients with a follow-up period of at least 1 year were analyzed. The median (IQR) age at PGA using HIFU was 65.0 (60.0-72.0) years. The median PSA and prostate volume were 5.20 (3.71-7.81) ng/ml and 34.6 (25.5-46.1) ml, respectively. The median number of total and positive cores on TRUS-guided biopsy were 12.0 (12.0-12.0) and 1.0 (1.0-2.0). The Gleason grade (GG) on TRUS-guided biopsy were as follows: GG1 = 86 (89.6%), GG2 = 8 (8.3%) and GG3 = 2 (2.1%). For TPMB, Median number of total and positive cores were 26 (24.0-36.0) and 2.0 (1.0-3.0), respectively. After confirmatory TPMB, the treatment plan was changed in 13.5% (13/96) of patients from unilateral to bilateral PGA using HIFU. The 1- year follow-up TRUS-guided biopsy revealed that any PCa (regardless of GG) was identified in 13 (13.5%) patients, and 7 (7.3%) patients had clinically significant PCa (csPCa, GG ⩾ 2). The infield and outfield positive rates were 8.3% (8/96) and 3.1% (3/96) for any PCa and 3.1% (3/96) and 2.1% (2/96) for csPCa, respectively.
Conclusions: The PGA using HIFU can provide acceptable oncological outcomes in patients with localized PCa. Confirmatory TPMB plays an important role in analyzing the location and extent of PCa, thus affecting the treatment plan. Therefore, Confirmatory TPMB should be considered to improve oncological outcomes in patients with localized PCa eligible for PGA using HIFU.
Baseline characteristics.
Variables
Value
Total number
96 (100)
Age, years
Median (IQR)
65.0 (60.0-72.0)
Mean (SD)
65.3 (8.7)
Body mass index, kg/m2
Median (IQR)
24.8 (22.8-26.8)
Mean (SD)
24.9 (2.6)
Hypertension, n (%)
48 (50.0)
Diabetes mellitus, n (%)
21 (21.9)
PSA, ng/dL
Median (IQR)
5.20 (3.71-7.81)
Mean (SD)
6.69 (5.60)
Prostate volume, mL
Median (IQR)
34.6 (25.5-46.1)
Mean (SD)
38.1 (18.6)
PSA density
Median (IQR)
0.12 (0.10-0.21)
Mean (SD)
0.16 (0.19)
Number of cores on TRUS-guided biopsy, n (%)
Median (IQR)
12.0 (12.0-12.0)
Mean (SD)
12.2 (1.7)
Number of positive cores on TRUS-guided biopsy, n (%)
Median (IQR)
1.0 (1.0-2.0)
Mean (SD)
1.8 (1.5)
Number of target cores on TRUS-guided biopsy, n (%)
Median (IQR)
2.0 (2.0-3.0)
Mean (SD)
2.2 (2.1)
Number of positive target cores on TRUS-guided biopsy, n (%)
Median (IQR)
1.0 (1-2)
Mean (SD)
1.5 (1.4)
Biopsy Gleason grade on TRUS-guided biopsy, n (%)
Gleason grade 1
86 (89.6)
Gleason grade 2
8 (8.3)
Gleason grade 3
2 (2.1)
Maximal tumor involvement on TRUS-guided biopsy, %
Median (IQR)
10 (5.0-25.0)
Mean (SD)
17.3 (18.6)
Number of cores on transperineal mapping biopsy, n (%)
Median (IQR)
26.0 (24.0-36.0)
Mean (SD)
29.2 (5.8)
Number of positive cores on transperineal mapping biopsy, n (%)
Median (IQR)
2.0 (1.0-3.0)
Mean (SD)
2.1 (2.1)
Biopsy Gleason grade on transperineal mapping biopsy, n (%)
Benign
25 (26.0)
Gleason grade 1
60 (62.5)
Gleason grade 2
9 (9.4)
Gleason grade 3
2 (2.1)
Maximal tumor involvement on transperineal mapping biopsy, n (%)
Median (IQR)
10.0 (2.5-25.0)
Mean (SD)
18.5 (24.9)
Clinical stage
cT1
25 (26.0)
cT2a
32 (33.3)
cT2b
22 (22.9)
cT2c
17 (17.8)
PI-RADS score in preoperative mpMRI
1-2
25 (26.0)
3
57 (59.4)
4
14 (14.6)
IQR, interquartile range; SD, standard deviation; PSA, prostate-specific antigen; TRUS, transrectal ultrasound; mpMRI, multiparametric magnetic resonance imaging.
The suitability of hemi-ablation for patients diagnosed with localised prostate cancer following multiparametric MRI targeted and non-targeted transperineal prostate biopsy
Deepika Reddy1, David Eldred-Evans1, Mathias Winkler1,2, Taimur T Shah1,2, Hashim U Ahmed1,2,3
1Imperial College London, UK, 2Imperial College Healthcare NHS Trust, London, UK, 3Cromwell Hospital, London, UK
Introduction: Evidence reporting comparable medium-term outcomes following focal therapy versus radical treatment modalities for localised prostate cancer is growing. Within the UK and Europe, despite being permitted if outcomes are prospectively collected, focal cryotherapy and High Intensity Focussed Ultrasound (HIFU) is only available in select centres. It is possible that not all patients suitable for focal therapy are referred for consideration for such treatment at select tertiary centres as the proportion of potentially suitable patients once diagnosed with localised prostate cancer is not widely understood. We determined how many patients diagnosed with localised prostate cancer following MRI and transperineal prostate biopsy in multiple prospective observational studies could be suitable for hemi-ablation.
Methods: Patients recruited into PICTURE trial, PROMIS trial, and RAPID pilot pathway were evaluated. Suitability was determined in a stepwise nature according to the Delphi Consensus criteria: PSA </=20ng/ml, </=rT3aN0, Gleason Grade Group (GGG) </=3, if highest (GGG) was 1 then cancer length must be >/=6mm, and treatment pattern allowed up to unilateral hemi-ablation and spared at least 1 neurovascular bundle. Primary outcome allowed up to 5mm GGG1 to be untreated, secondary outcome allowed up to 5mm GGG1 +/- 1 core of 3+4 to remain untreated. Each study obtained local or external Research and Ethics approval.
Results: 200/330 (61%) of patients recruited into PICTURE were diagnosed with </=rT3aN0 prostate cancer with PSA </=20ng/ml. 146/200 (73%) had either GGG 2 or 3, or 1 with MCCL>/=6mm, 3 had GGG>3, 51 had GGG1 <6mm. When allowing for GGG1 <6mm to remain untreated 96/200 (48%) patients had disease suitable for hemi-ablation, 63 would have untreated disease. When allowing for 5mm GG1+/- 1 core of 3+4 to remain untreated 114/200 (57%) were suitable for hemi-ablation. Within PROMIS 406/740 (55%) patients had </=rT3aN0 prostate cancer and PSA </=20ng/ml. 277/406 (68%) had either GGG 2 or 3, or 1 with MCCL>/=6mm, 24 had GGG>3, 91 had GGG1 <6mm. When allowing for GGG1 <6mm to remain untreated 159/277 (57%) patients had disease suitable for hemi-ablation, 81 would have untreated disease. When allowing for 5mm GG1+/- 1 core of 3+4 to remain untreated 177/277 (64%) were suitable for hemi-ablation. 612/2372 (26%) of patients in RAPID were diagnosed with </=rT3aN0 disease and PSA </=20ng/ml. 423/612 (46%) had either GGG 2 or 3, or 1 with MCCL>/=6mm, 83/612 had GGG>3, 103/612 had GGG1 <6mm. When allowing for GGG1 <6mm to remain untreated, 309/612 (50%) had disease suitable for hemi-ablation, 41 of whom would have untreated disease. When allowing for 5mm GG1+/- 1 core of 3+4 to remain untreated 313/612 (51%) were suitable for hemi-ablation.
Conclusions: Independent of varying incidence of prostate cancer within the cohorts evaluated, once diagnosed with localised disease between 5 and 6 patients out of 10 could be considered suitable for focal treatment, thus patients should be counselled and referred accordingly.
Disclosures: Deepika Reddy has received funding from Prostate Cancer UK for research and travel grants from Sonablate Corp and Imperial College Healthcare Charity. Eldred-Evans received funding from the Urology Foundation, the BMA Foundation for Medical Research, Imperial Health Charity and the Royal College of Surgeons of England. Mathias Winkler receives a travel grant and previously a loan of device from Zicom Biobot. Taimur T Shah has received funding from Prostate Cancer UK and the St Peters Trust for clinical research and has received funding for the conference attendance from Astellis, Ferring and Galil Medical. Hashim U Ahmed is supported by core funding from the United Kingdom’s National Institute of Health Research (NIHR) Imperial Biomedical Research Centre. Ahmed currently receives funding from the Wellcome Trust, Medical Research Council (UK), Cancer Research UK, Prostate Cancer UK, National Institute for Health Research (UK), The Urology Foundation, BMA Foundation, Imperial Health Charity, NIHR Imperial BRC, Sonacare Inc., Trod Medical and Sophiris Biocorp for trials in prostate cancer. Ahmed was a paid medical consultant for Sophiris Biocorp in the previous 3 years. Ahmed is a proctor for HIFU, cryotherapy and Rezum and is paid for training other surgeons in these procedures.
Urinary Retention After High Intensity Focused Ultrasound for Prostate Cancer: Changing Practice at a High-Volume Center
Michael West, Dhaval Jivanji, Yitzchak Katlowitz, David Silver, Ariel Schulman
Division of Urology, Maimonides Medical Center, 745 64th St. 4th Floor, Brooklyn, NY, USA
Introduction: High Intensity Focused Ultrasound (HIFU) has been used for the treatment of localized prostate cancer in the United States for several years and our institution was an early adopter. We used the FocalOne® robotic HIFU system. We maintained an IRB-approved prospective database of these patients. As we gained more experience with HIFU, we noticed that post-treatment urinary retention (UR) was a major issue that needed to be addressed. Our objective is to characterize UR after HIFU and report on strategies we employed for prevention and management.
Methods: We reviewed our database of 55 unique patients who underwent a total of 63 HIFU treatments for prostate cancer for demographic data, prostate size, development of UR and management thereof.
Results: Mean age at time of treatment was 68 years (range 51-84), mean BMI was 28.4 Kg/m2 (range 19.8-38.6), mean prostate size was 45.6 cc (range 9-214). 3 (4.8%) were low risk, 51 (80.9%) were intermediate risk, and 8 (12.7%) were high risk. Patients developed UR in 15 (23.8%) treatments. Younger age, higher BMI, and treatment in the first 30 cases were found to be statistically significant predictors of UR (table 1). An outlet procedure was needed after 6 (9.5%) of cases. Given the high rate of UR early in our series, we began routinely placing a suprapubic catheter (SPC) just prior to HIFU, which was removed when the patient began voiding per urethra. After this, only 2/33 remaining treatments (6.0%) were complicated by UR. In addition, we began offering outlet procedures to patients we felt had a high risk of UR, namely those with a large prostate and/or lower urinary tract symptoms at baseline.
Conclusions: UR was a major challenge early on when our institution began offering HIFU. We began routinely placing SPCs at the time of HIFU. After this, we noticed a significant reduction in UR events, including those requiring an outlet procedure.
Patient characteristics and their association with UR.
All(n=63)
UR(n=31)
No UR(n=12)
p Value
Average Age (IQR)
68.7 (64-75)
63.3 (60-67)
70.4 (64-75)
0.003
BMI (IQR)
28.3 (25-31)
30.7 (28-34)
27.6 (25-30)
0.015
Prostate Size (IQR)
45.6 (25-48)
36.1 (22-48)
48.3 (28-51)
0.287
Risk Stratification
0.537
Low
3
0
3
Intermediate
51
11
39
Favorable Intermediate
20
6
14
Unfavorable Intermediate
31
5
25
High
8
3
5
Treatment in First 30 Cases?
0.0005
Yes
30
13
17
No
33
2
31
Retrospective analysis of MRI-guided transurethral ultrasound ablation (TULSA) in men with prostates larger than 90 cc
Joseph J. Busch Jr., Kathy Busch, Roland Rose, Jessica Pendergraft
Busch Center, Alpharetta GA, USA
Introduction: Prostate size is an important consideration when selecting patients for minimally invasive treatments for prostate cancer (PCa) and benign prostatic hyperplasia (BPH).
The TACT pivotal trial studied whole-gland MRI-guided transurethral ultrasound ablation (TULSA) in men with localized PCa, excluding patients with obstructive BPH or prostate volume larger than 90 cc. Here we report our single-center functional, imaging, and cancer surveillance outcomes in men with PCa and/or BPH who had prostate glands
larger than allowed in the TACT study.
Methods: Men whose prostate volume exceeded 90 cc on pretreatment diagnostic MRI were identified among 218 men with at least 6 months follow-up after undergoing TULSA at our center. Treatment plans were defined based on disease extent and patient
preference, using intraoperative DWI and ADC maps in addition to T2-weighted imaging.
Routine post-operative course for large ablation volumes included prophylactic antibiotics, foley catheterization for 2 weeks, ibuprofen, and alfuzosin. Patients were followed with daily communication for 2 weeks, PSA test every 3 months, IPSS, IIEF, and post-TULSA mpMRI at 6-9 months.
Results: 34 patients with pre-TULSA prostate volume exceeding 90 cc were identified. 59% of this subgroup were seeking combined treatment for PCa plus BPH, 41% for BPH alone. The median age was 68 (IQR 63-72) years, with follow-up availability of 11 (7-19) months.
The proportion of men with primary Grade Group 1-5 PCa were: 5%, 44%, 22%, 5%, 22%. The maximum prostate volume was 275 cc; 17 men had prostate volume greater than 120 cc. Whole-gland ablation was performed in 12 patients, subtotal in 19, and hemi- ablation or less in 3 cases. 16 treatments included ablation of a protruding median lobe, and 11 cases used a two-part ablation for target regions longer than the 5 cm active window. Overall procedure times for these complex cases were median 3.7 (IQR 3.2-4.2) hours, including ablation times of 87 (IQR 73-114) minutes. PSA decreased from median 7.6 (IQR 5.6-9.1) to 1.5 (0.6-4.2) ng/mL. Of 13 patients who had follow-up mpMRI, 10 had no evidence of residual disease, 2 had out-of-field lesions, and 1 had in-field recurrence. Prostate volume decreased by a median of 56%. All patients are pad-free; two experienced urine leakage that resolved within 2 months. 80% maintained baseline erection firmness sufficient for penetration (IIEF Q2⩾2). IPSS urinary symptom scores improved 60% from median 17 (IQR 14.5-21.0) to 6 (5-8). One patient had DVT resolved with anticoagulants as well as urethral stricture requiring endoscopic intervention; one patient had Grade 3 GU infection resolved with intravenous antibiotics. No grade ⩾4 events and no rectal injuries occurred.
Conclusions: This retrospective analysis demonstrates promising real-world safety and efficacy of TULSA for the ablation of prostate cancer and relief of obstructive urinary symptoms in patients with prostate volumes larger than those studied in regulatory trials.
Disclosures: Profound Medical assisted with technical analysis and figure 1 preparation.
Whole-gland TULSA targeting Grade Group 2 prostate cancer and enlarged transition zone in a patient with a 107 cc gland.
Assessing the outcomes of repeat biopsy in patients with high grade prostatic intraepithelial neoplasia and atypical small acinar proliferation using a large multi-institutional collaborative; can mpMRI be used in lieu of a repeat prostate biopsy?
Steven Leonard1, Emma Helstrom1, Spencer Bell2, Alberto Castro-Bigalli1, Leilei Xia3, Bobby Wang1, Robert Uzzo1, Rosalia Viterbo1, David YT Chen1, Richard E. Greenberg1, Marc Smaldone1, Elizabeth Handorf4, Alexander Kutikov1, Andres Correa1, Raju Chelluri1 on behalf of PURC Collaborators
1Fox Chase Cancer Center, Philadelphia, PA, USA, 2University of Kentucky College of Medicine, Lexington, KY, USA, 3University of Southern California Keck School of Medicine, Los Angeles, CA, USA, 4Rutgers University School of Public Health, New Brunswick, NJ, USA
Introduction: The NCCN suggests repeat prostate needle biopsy (PNBx) for high-grade prostatic intra-epithelial neoplasia (HGPIN) and atypical small acinar proliferation (ASAP) within 12 to 24 months of diagnosis. The landscape for managing NCCN low-risk disease has changed dramatically but questions remain regarding optimal management of men who harbor such lesions without a finding of prostate cancer (PCa). Further, prior studies have not evaluated the role of current technological advancements, including multiparametric magnetic resonance imaging (mpMRI) of the prostate. Our objective was to determine the incidence of clinically significant prostate cancer (csPCa) in the Pennsylvania Urologic Regional Collaborative (PURC) database after an initial PNBx showed ASAP, HGPIN, or both without any PCa. We then aimed to investigate the association of mpMRI to findings to csPCa at repeat PNBx. (126/150)
Methods: We performed a retrospective review of PURC, a multi-institutional dataset of PCa patients. Men found to have ASAP, HGPIN, or both as their first pathologic finding on a PNBx (the index PNBx) who had a repeat PNBx within 1 year were included. Tabulated data included demographics, laboratory, imaging, and pathologic findings. We determined the number of visible mpMRI lesions, the highest PI-RADS score, and lesion size, as well as adverse imaging features. mpMRI was deemed high-risk if the PI-RADS score was ⩾4. Detection of csPCa (Gleason⩾3+4 or Gleason Grade 2) on repeat PNBx was the outcome of interest. We performed the Fisher exact test for association to determine the relationship of imaging parameters to the detection of csPCa. (118/150)
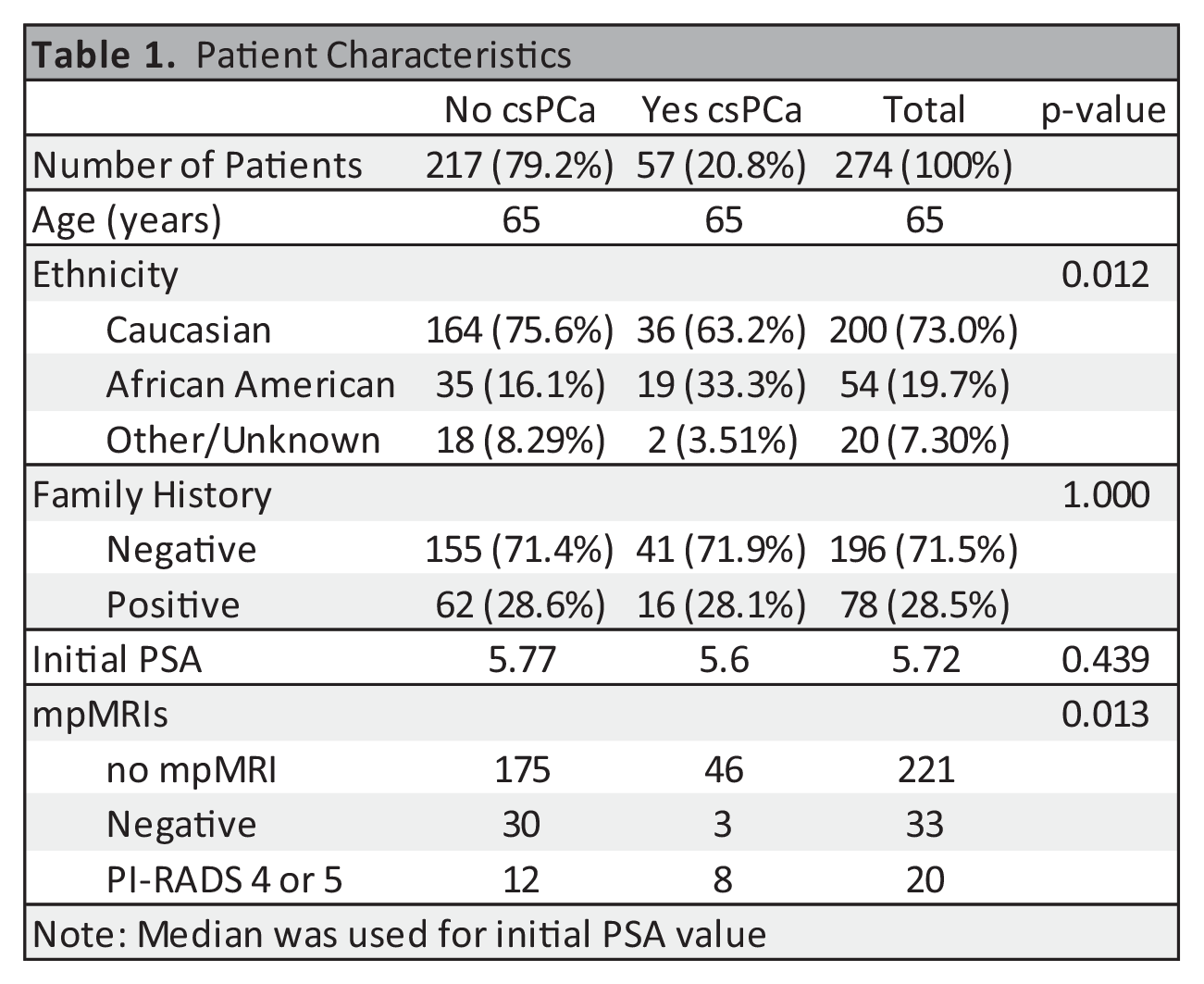
Results: From an initial cohort of 14,272, we identified 274 patients who had an index PNBx showing ASAP, HGPIN, or both without PCa who then had a subsequent confirmatory PNBx within one year. Overall, the median age was 65 and the median initial PSA was 5.72 (Table 1). Of the 274 patients, 57 (20.8%) harbored csPCa on repeat PNBx. Fifty-three of the 274 patients had an mpMRI between their index PNBx and repeat PNBx. Eleven of the patients with csPCA had qualifying imaging with eight demonstrating PI-RADS ⩾4 lesions. Forty-two of the patients without csPCa on repeat PNBx had qualifying imaging with 12 mpMRIs demonstrating PI-RADS ⩾4 lesions. The association of high-risk mpMRI to the finding of csPCa was statistically significant (P=0.013), with a specificity of 0.7273 and a sensitivity of 0.7143. The maximum lesion size and number of lesions between the two cohorts was also statistically significant (Table 2). (149/150)
Conclusions: We conclude that mpMRI may be tool to recognize csPCA in patients whose index PNBx showed ASAP, HGPIN, or both without PCa. The next step in our investigation is to determine the ability of mpMRI findings to predict csPCa with regression modelling. Limitations of our study include its retrospective nature, limited sample size, and restriction to one geographic region/cohort of patients. Further research is warranted to validate our findings in a prospective manner. (73/150).
Conflicts of interest: None of the authors have any direct or indirect conflicts of interests pertaining to this research.
Prostate ablation for management of prostate cancer: A single-center experience
1Division of Urology, Department of Surgery, University of Cincinnati College of Medicine, Cincinnati, OH, USA, 2Division of Biostatistics and Bioinformatics, University of Cincinnati College of Medicine, Cincinnati, OH, USA, 3Department of Radiology, University of Cincinnati College of Medicine, Cincinnati, OH, USA
Introduction: Prostate ablation has emerged as a significant advancement in the management of prostate cancer (PCa). While whole-gland ablation has historically been associated with higher rates of morbidity and is often offered to older men with declining health as an alternative to radiation, newer forms of targeted therapy have demonstrated efficacy with reduced side effect profile and are more appropriate for use in younger patients. These treatments have revolutionized treatment of PCa, leading to improved outcomes and enhanced patient experiences; nonetheless, the need for additional data remains high. This study aimed to evaluate effectiveness and functional impact of various forms of prostate ablation as treatment options for managing intermediate risk PCa.
Methods: 151 participants underwent either whole-gland or focal ablation guided by MRI-US fusion using various modalities such as high intensity focused ultrasound (HIFU), cryotherapy, or irreversible electroporation (IRE) at a single center between 2018 and 2023. Follow up monitoring and assessment of oncological outcomes varied based on type of ablation used. Patients who received whole-gland ablation underwent regular quarterly prostate-specific antigen (PSA) testing to assess for biochemical failure (BF). Those receiving targeted therapy were monitored with additional follow-up 6-9 months later consisting of multiparametric magnetic resonance imaging (mpMRI) and a combination of targeted and systematic biopsies using MRI-US guidance to track imaging and pathological failure (PF), respectively. Additionally, functional outcomes were measured by tracking reported rates of urinary incontinence and erectile dysfunction via the American Urologic Association Symptom Score (AUA-SS) and Sexual Health Inventory for Men (SHIM) indices.
Results: 89/150 men received cryotherapy, the most used treatment modality in our study population. Of these patients, 39 (43.8%) had whole-gland ablation. HIFU and IRE were used by 40 (26.6%) and 21 (14.0%) patients, respectively. Whole-gland ablation was less common in HIFU group (10/40, 25.0%), and all patients receiving IRE were treated with focal therapy. Of the 101 patients undergoing focal ablation, 16 (15.84%) experienced PF (4 HIFU, 2 IRE, 10 cryotherapy). This contrasted with the whole- gland ablation cohort, where only 3/49 (6.12%) showed PF, all of whom received cryotherapy. Imaging failure was seen in 20 patients: 4 whole-gland and 16 focal (10 cryotherapy, 5 HIFU, 1 IRE). BF occurred in 12 patients, predominantly in the focal ablation group (10/12) (7 cryotherapy, 1 HIFU, 2 IRE). Both BF cases in whole-gland received cryotherapy. Patients receiving whole-gland cryoablation were most likely to have loss of potency and had the highest chance of incontinence.
Conclusion: Our findings align with the current body of evidence supporting ablation as a safe option for PCa, with minimal short/intermediate-term morbidity and satisfactory oncological outcomes. Our data highlights several significant differences between whole-gland and focal therapy as well as across different modalities in areas such as complication rates, side effects, and recurrence. Most notably, whole-gland cryoablation was associated with a lower recurrence rate but higher rate of overall complications, in line with our hypothesis. To better inform and optimize management of intermediate- risk PCa using all subtypes of ablation future studies are essential to document key outcome measures over time.
Conflict of interest: The authors declare that there was no conflict of interest with this article.
Disclosure of financial funding: The authors declare that there was no external funding received for this article.
Racial disparity in prostate cancer diagnosis: a comparison of prostate biopsy results in african american and white men using an mri-based biopsy strategy
Ali Kasraeian1, Miguel Alcantara1, Kaitlyn Mola Alcantara1, Sean Parsons1, Madison Crosby1, Joshua Yellin2, Adam Brochert3, Jamie Cesaretti, Ahmad Kasraeian1
1Kasraeian Urology, Jacksonville, USA, 2Insite Radiology, Jacksonville, Florida, USA, 3Precision Imaging Centers, USA
Introduction: African American (AA) men in the United States have an increased burden of morbidity and mortality from prostate cancer (PCa). The roles of factors related to both racial disparities and intrinsic biological traits remain to be determined. We quarried our prospective database of standard and MRI fusion biopsies (tMRI/US FPB) to determine if any pre-biopsy characteristics predicted adverse tumor pathology.
Methods: Between January 2017 and October 2022, 828 men underwent prostate biopsy (PBx) using an MRI based algorithm. Men with negative MRI underwent standard PBx (n=433), while those with lesion on mpMRI underwent tMRI/US FPB (n=395). All patients underwent mpMRI of the prostate, interpreted by a single radiologist using the PIRADS scoring system. 3D rendering of the regions of interest was performed by the radiologist prior to tMRI/US FPB performed by a single urologist using the Invivo UroNav Fusion Biopsy System. A standard 14-core PBx was performed at the same time in all tMRI/US FPB cases. Prospective data was collected and analyzed.
Results: Of 828 men who underwent standard and tMRI/US FP with 14Bx, 824 presented with rise in PSA and 264 had a suspicious digital rectal exam. 367/608 (60%) of White men and 104/147 (71%) of AA men were found to have PCa (p=0.00443). 224/608 (37%) of White men and 74/147 (50%) of AA men had a Gleason score of 7-10 (p=0.019). Age, DRE status, PIRADS score, and incidence of Gleason score 6 PCa were not found to be significantly different by race. 163/605 (27%) of White men and 20/146 (14%) of AA men had a PSA upon presentation of 0-3.9 ng/ml (p=0.001). Of the 73/828 men who identify as not White and not Black, no significant difference was found for any tested factor but 26% presented with PSA between 0-3.9 ng/ml (p=0.053) which was similar to that seen in White men.
Conclusions: In this dataset, AA men had a higher positive biopsy rate and presented with a higher PSA than White men. We did observe a higher incidence of Gleason 7 and higher PCa which one would expect in a cohort of patients who presented for biopsy in the community with a significantly higher PSA presentation. Continuing education of primary care providers regarding the importance of PSA testing in the AA community should be emphasized by both the urological and primary care professional medical societies.
Disclosures: none
A Single Institution Experience with Subtotal Gland Cryoablation for Primary Prostate Cancer Treatment: 3-Year Functional and Oncologic Outcomes
Paul Horning, Bernadette Zwaans, Bradley Rosenberg
William Beaumont University Hospital, Corewell Health East, USA
Introduction: Prostate cancer remains a common malignancy and major cause of cancer deaths in men. The gold standard of localized prostate cancer treatment has been whole gland treatments such as radiation and radical prostatectomy, however these therapies can have significant morbidity. Focal treatments appear to have a more favorable side effect profile, and acceptable oncologic outcomes, especially in patients with lower-risk disease. As subtotal gland cryoablation is still considered a developing technique, we aim to report on all our patients with at least 3-year follow-up to assess oncologic and functional outcomes.
Methods: A retrospective chart review was performed on 145 patients who underwent subtotal cryoablation for prostate cancer between 2016 to 2023 at a single institution by a single physician. There were 95 total patients with at least 3 year follow-up. 79 patients had cryoablation as their primary treatment, while the others had salvage cryoablation. All patients had limited prostate cancer diagnosed on biopsy, and underwent treatment with 2 freeze/thaw cycles of the biopsy proven area (most were hemigland ablations). Cancer recurrence was the primary endpoint and defined as biopsy proven clinically significant recurrence (GG2 or higher), or persistently rising PSA with positive imaging. The prompt for biopsy was usually a rising PSA. Secondary outcomes included pre and post operative quality of life measures of LUTS and erectile function using AUASS and SHIM scores, respectively.
Results: Of the 79 patients, 18 (23%) had recurrence at 3 years. There were 49 (62%), 20 (25%), and 10 (13%) patients with GG ⩽2, GG=3, and GG ⩾ 4, respectively. Recurrence rates for GG ⩽ 2, GG = 3, and GG
⩾ 4 were 14%, 30%, and 50%, respectively. Of the 21 (27%) patients that were biopsied within the 3 year follow up period, 15 (71%) of those patients had clinically significant recurrence (GG2 or higher). Of those positive biopsies, 7 (47%) had in treatment field recurrence, 6 (40%) had out of treatment field recurrence, and 2 (13%) had both in and out of treatment field recurrence. In patients with GG ⩾ 4 disease compared to GG ⩽ 2 disease, there was a significantly higher risk of recurrence (RR 3.5, 95% CI 1.4 - 8.8). In patients with GG=3 compared to GG ⩽ 2, there was also a higher risk of recurrence (RR 2.5, 95% CI 1.05-6.1). There was no significant difference between pre and post operative AUASS and SHIM scores (p=0.07 and p=0.13, respectively).
Conclusions: Focal cryoablation for GG2 prostate cancer provides acceptable 3-year recurrence free survival and is well tolerated without significant changes in AUASS and SHIM scores. In patients with higher risk disease (GG ⩾ 3), our data showed higher risk of recurrence at 3 years. Limitations include the retrospective nature of this study, and relatively small sample size. Longer term follow-up data, and ongoing investigation of optimal patient selection and post operative monitoring would be helpful to continue improving focal therapy outcomes for prostate cancer.
Oncologic and Functional Outcomes At 3 Years.
Oncologic Outcomes
Number of Recurrence at 3 years(%)
Relative Risk with 95% Cl
p-value
GGl (Gleason 3 + 3)
0 (0)
GG2 (Gleason 3 + 4)
7 (15)
GG3 (Gleason 4 + 3)
6 (30)
GG4 (Gleason 8)
3 (60)
GG5 (Gleason 9 - 10)
2 (40)
Treatment faiiire of GG = 3 vs GG :<:; 2
2.5 (1.05 - 6.1)
0.04
Treatment failure of GG 4 vs GG :<:; 2
3.5 (1.4 - 8.8)
0.02
Functional outcomes
Pre-Operative Average (SD)
Post-Operative Average (SD)
p-value
AUASS
7.9 (6.7)
7.1 (4.1)
0.07
SHIM
15.9 (9.4)
12.6 (8.3)
0.13
Artificial intelligence for automated segmentation of prostate cancer and pelvic anatomy
Sakina Mohammed Mota1, Joshua Shubert1, Alan Priester1,2, Tom Summers1, Matthew Salvador1, Shyam Natarajan1,2
1Avenda Health, Inc, USA, 2David Geffen School of Medicine, Department of Urology, USA
Introduction: A reliable distinction of anatomy within and adjacent to the prostate is critical for diagnosing and treating prostate cancer (PCa). Manual localization of pelvic anatomy and PCa is tedious, subjective, and often inaccurate due to variability in prostate MRI scans. Hence, we developed artificial intelligence (AI) models to segment pelvic anatomy and cancer automatically and effectively.
Methods: AI-based PCa region of interest (ROI) and pelvic anatomy segmentation was performed using a nnUNet architecture. The PCa ROI segmentation model was trained using 1500 mpMRI cases (obtained from the 2022 “PI-CAI” challenge) and their corresponding AI-predicted zonal anatomy labels as inputs. All PCa ROI labels had a PI-RADS score ⩾ 4. Four additional AI models were trained individually using 912, 89, 833, and 332 T2W MRI cases for automated segmentation of prostate zones, pelvic bone, urethra, and other structures, respectively. Prostate zones consisted of the peripheral zone (PZ), central zone (CZ), and anterior fibromuscular stroma (AFS). Other structures included the rectum, bladder, and seminal vesicles (SV). Training labels for pelvic anatomy were manually defined using ITK-SNAP and 3D Slicer. All models were trained using 5-fold cross- validation and independently tested on 25 “Prostate158” challenge cases. ROI, PZ, and CZ test set labels were derived from Prostate158, and all others were manually generated by three imaging scientists. Another senior imaging scientist reviewed all test data.
Results: AI models achieved DICE score and max Hausdorff distance (mm) means of [84%, 2.5] for PZ, [91%, 3.0] for CZ, [63%, 3.4] for AFS, [97%, 2.0] for bladder, [99%, 0.2] for bone, [96%, 3.8] for rectum, and [77%, 4.4] for SV. Mean and max centroid distances (CD, mm) for urethra segmentation were 1.92 and 7.42. Lastly, the AI model segmented PCa ROIs with an AUC of 0.83 and 42% average precision.
Exemplary image (test case 11) showing AI performance for automated segmentation of PCa and pelvic anatomy (prostate zones, pelvic bone, urethra, rectum, bladder, and SV) compared to ground truth.
Conclusions: AI can accurately and automatically segment pelvic anatomy and prostate cancer, potentially streamlining prostate cancer management. Among many potential applications, this could improve cancer diagnostic accuracy and help clinicians avoid damage to critical structures during interventions.
Conflicts of Interest: Mota, Shubert, Priester, Summers, and Salvador are employees of Avenda Health. Natarajan is a cofounder of Avenda Health.
Artificial Intelligence-Based Cancer Mapping To Aid In Prostate Cancer Therapy
Sakina Mohammed Mota1, Alan Priester1,2, Joshua Shubert1, Jeremy Bong1, James Sayre3, Brittany Berry-Pusey1, Wayne Brisbane2, Shyam Natarajan1,2
1Avenda Health Inc, USA, 2David Geffen School of Medicine, Department of Urology, USA, 3University of California, Los Angeles, Department of Radiological Sciences and Biostatistics, USA
Introduction: Focal therapy (FT) for prostate cancer is gaining prominence as an alternative to whole-gland treatment. FT efficacy relies on predicting disease margins, but their underestimation and patient-specific optimization remain largely unaddressed problems. An artificial intelligence (AI)-based cancer mapping and decision support tool was built using pre-biopsy MRI, targeted biopsy data, and PSA to aid urologists in identifying cancer margins. A reader study was conducted to compare this AI-based software against the standard of care (SOC) in determining clinically significant prostate cancer (csPCa) extent.
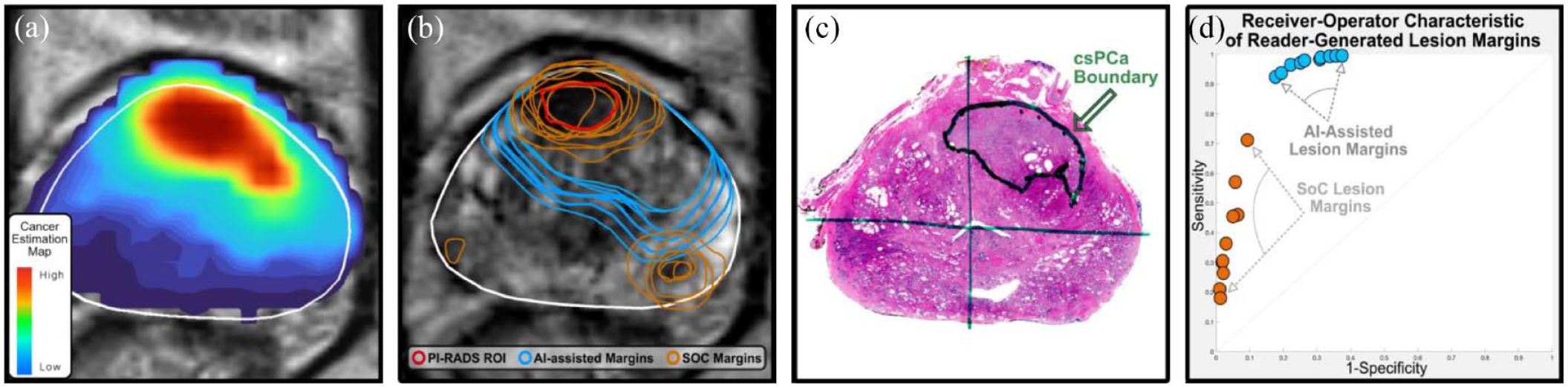
Methods: Seven urologists and three radiologists from five institutions with 2 – 23 years of expertise each evaluated 50 prostatectomy cases (total of 1000 reads). Cases were prospectively eligible for FT, with GG 2-3 csPCa, ⩾1 region of interest (ROI), and disease that appeared localized to a single hemisphere or the anterior gland. Each case included T2-weighted MRI, ROI segmentation, and pathology reports with conventional locations. Readers were asked to produce contours on each image that prioritized the inclusion of all csPCa, excluding non-csPCa tissue as a secondary objective. First, readers manually defined margins using all given data (SOC). Then, after ⩾4 weeks had passed, readers produced AI-assisted margins using custom software (Unfold AI, Avenda Health, CA) [Fig. A]. Margins from each method [Fig. B] were evaluated against WM pathology [Fig. C] as ground truth. Statistical tests were performed using generalized estimating equations.
(A) AI-generated cancer estimation map for an exemplary case, which is thresholded by readers to define AI-assisted lesion margins; (B) the same example case displaying SOC and AI-assisted lesion margins produced by the readers (N=10), with the prostate boundary shown in white; (C) whole mount ground truth for the same case; (D) ROC curve illustrating sensitivity versus specificity measures for each reader, averaged across all lesion margins produced using AI-assisted and SOC methodology. In this instance and overwhelmingly throughout the study, AI-assisted margins more effectively and consistently encapsulated the tumor than SOC margins.
Results: AI margins had superior sensitivity (97.4% vs. 38.2%, p < 0.0001) to SOC margins in classifying csPCa [Fig. D]. AI-assisted margins also had superior balanced accuracy, i.e. (specificity + sensitivity)/2, to SOC margins (84.7% vs. 67.2%, p < 0.0001). On average, AI-assisted margins completely encapsulated csPCa in 72.8% of cases, compared to only 1.6% of cases with SOC methods (p < 0.0001). Furthermore, the average time spent fell from 3.5 minutes (SOC) to 2.0 minutes (AI-assisted, p < 0.0001).
Conclusions: AI-assisted cancer mapping helps address the systematic underestimation of csPCa by SOC methods. This study establishes that AI-assisted margins greatly improve csPCa encapsulation, which could improve oncological efficacy for focal treatments.
Research Support/Funding: Funded in part by the National Cancer Institute at the National Institutes of Health, Grant R01CA158627
Conflicts of Interest: Mota, Priester, Shubert, and Bong are employees of Avenda Health. Berry-Pusey and Natarajan are cofounders of Avenda Health. Sayre consults for Avenda Health.
Tumor Size Estimation Using An Artificial Intelligence Prostate Cancer Mapping Algorithm
Alan Priester1,2, Joshua Shubert1, Sakina M. Mota1, Shyam Natarajan1,2
1Avenda Health, Inc, 2University of California, Los Angeles, USA
Introduction: Accurate estimation of prostate cancer tumor size is critical for assessing risk and determining treatment strategies. Since conventional clinical and imaging estimates are weakly correlated with tumor size, an artificial intelligence (AI) model was used to map clinically significant prostate cancer (csPCa, i.e. Gleason grade group ⩾ 2) risk in 3D and estimate tumor volume.
Methods: Cases with at least one csPCa-bearing MRI-visible lesion and no ablative treatment prior to prostatectomy were retrospectively selected for study inclusion. Whole mount (WM) pathology slides were registered to preoperative MRI, and pathologist-defined csPCa contours were interpolated to define ground- truth tumor volume (Fig B,D). MRI and simulated biopsy was then used to generate a 3D cancer map (Fig A,C) for each case using AI software (Unfold AI, K221624). The sum of estimated csPCa probability for voxels throughout the prostate was correlated to WM tumor volume using linear regression. For comparison, 6 conventional metrics derived from prostate serum antigen (PSA), biopsy results, and PI-RADS regions of interest (ROIs) were likewise correlated to tumor volume. The accuracies of linear regression fits were compared using Wilcoxon signed-rank tests with α = 0.05.
(A,C) Cancer estimation maps and (B,D) Ground-truth whole mount histopathology slides for a large tumor (top row) and a smaller tumor (bottom row). (E) plots the correlation between AI model output (the sum of estimated cancer probability in voxels throughout the prostate) and ground-truth tumor volume, R2 = 0.81.
Results: 97 patients met study eligibility criteria. AI cancer maps were strongly correlated to WM tumor volume with R2 = 0.81 (Fig E). Using a linear regression model to predict tumor volume, all conventional metrics were significantly less accurate than AI including: PSA (R2 = 0.27, p < 0.001), PSA density (R2 = 0.26, p < 0.001), number of csPCa-positive cores (R2 = 0.57, p < 0.001), maximum csPCa core length (R2 = 0.51, p < 0.001), total length of csPCa in all cores (R2 = 0.69, p = 0.005), and PI-RADS ROI volume (R2 = 0.33, p < 0.001).
Conclusions: AI was highly predictive of tumor volume, outperforming conventional clinical measures. More accurate tumor volume assessments may improve risk assessment and treatment strategy selection, particularly when defining margins for focal ablation or radiation dosing. This promising technique warrants further study, with the potential to improve prostate cancer management and treatment outcomes.
Disclosures and Conflicts of Interest: This work was funded in part by the United States National Cancer Institute (grant R01CA218547). All authors are employees of Avenda Health
Extracapsular Extension Risk Assessment Using An Artificial Intelligence Prostate Cancer Mapping Algorithm
Alan Priester1,2, Sakina M. Mota2, Joshua Shubert2, Shyam Natarajan1,2, Wayne G. Brisbane1
1University of California, Los Angeles, USA, 2Avenda Health, Inc, USA
Introduction: The presence of extraprostatic extension (ECE) is critical to risk stratification and management of prostate cancer (PCa), including determination of treatment eligibility and surgical margins. Current techniques for prediction of ECE, which rely upon interpretation of magnetic resonance imaging (MRI) and clinical data such as Gleason Grade group (GG) and prostate specific antigen (PSA), are imperfect. Herein we evaluate the use of an artificial intelligence (AI) cancer mapping algorithm to improve ECE risk assessment.
Methods: Consecutively accrued patients who received preoperative multiparametric MRI, confirmatory biopsy, and subsequent prostatectomy were evaluated (N = 121). A radiologist prospectively interpreted the MRI, defining regions of interest (ROIs) suspicious for PCa and ECE risk via a Likert scale. Following prostatectomy, a pathologist determined if and where ECE occurred using whole-mount slides (Fig B). An FDA-cleared AI cancer mapping algorithm (Unfold AI, K221624) was then investigated for ECE prediction. The algorithm incorporated T2-weighted MRI, serum PSA, and biopsy histopathology to generate 3D cancer estimation maps for each case. ECE risk was estimated as the total cancer probability of voxels intersecting and up to 2 mm beyond the prostate capsule (Fig A). For comparison, conventional metrics were also assessed: GG, serum PSA, MRI Likert score, Partin table value, and ROI capsular contact length. A receiver operator characteristic was generated for each metric, and areas under the curve (AUCs) were compared using DeLong’s test at α = 0.05.
(A) Exemplary AI-generated cancer estimation map, wherein the cancer probability of voxels intersecting and beyond the capsule was used to make an objective assessment of ECE risk. (B) Exemplary ground truth histopathology slide wherein ECE was observed in the prostate anterior, the highest-risk region identified by the AI algorithm. (C) Receiver operator characteristic for patient-level prediction of ECE using AI and conventional metrics.
Results: The distribution of GG on final diagnosis was 13% GG1, 56% GG2, 16% GG3, 9% GG4, and 6% GG5. ECE was present in 46/121 cases; of these, 76% had posterior ECE only, 15% had anterior ECE only, and 9% had both. The receiver operator characteristic for patient-level ECE prediction is shown in Fig C. The AUC of AI (0.88) was significantly higher (p < 0.001) than PSA (0.60), GG (0.68), MRI Likert score (0.71), and Partin tables (0.65). The AUC of AI was likewise higher than ROI contact length (0.83), an improvement that was suggestive but insufficient for statistical significance (p = 0.10).
Conclusions: Unlike conventional ECE predictors, AI can combine multi-modal data to map cancer risk in 3D. This approach shows promise as a means of ECE prediction, surpassing conventional methodology such as Partin tables and subjective MRI interpretation. Clinicians furnished with AI could potentially improve prostate cancer management, particularly when defining focal therapy eligibility and focal treatment margins. This approach shows considerable promise and warrants further study in broader populations.
Disclosures and Conflicts of Interest: This work was funded in part by the United States National Cancer Institute (grant R01CA218547). All authors except Wayne Brisbane are employees of Avenda Health.
Expanded Eligibility Criteria for Prostate Cancer Focal Therapy Does not Significantly Increase the Number of Potential candidates: A Multicenter Investigation From a Large Global Health Research Network (TriNetX)
Brian H. Im1, Aaron R. Hochberg1, Sohan S. Shah1, Anushka Ghosh1, Patrick Gomella2, J. Ryan Mark2, Mihir Shah2, Costas Lallas2, Joe Izes2, Adam R. Metwalli2
1Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, PA, USA, 2Department of Urology, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, PA, USA
Introduction: Focal therapy (FT) is being researched as an alternative to whole-gland prostate cancer treatments. We utilized the TriNetX database to determine the proportion of patients who might be candidates for FT.
Methods: The TriNetX database was queried for all adult male patients with a diagnosis of prostate cancer. We then created two cohorts: Group A - men with only Gleason 7 disease and Group B – men with Gleason 7 or 8 disease. Each cohort was then further limited to men with a PSA less than 10, and MRI of the prostate. Each subject who met these criteria represents patients potentially eligible to receive FT. Procedures available in the TriNetX database are High-Intensity Focused Ultrasound (HIFU) (CPT: 55880), Focal Laser Ablation (CPT: 0655T), and Focal Cryoablation (CPT: 55873). Prior to the specific CPT code for HIFU in 2017, all focal therapies were billed under “Unlisted Procedure, male genital system” (CPT: 55899). This code may represent FT or another urologic procedure; these queries provide the most generous estimate of those undergoing FT in the TriNetX database. Whole gland prostate treatments were queried, including robotic assisted laparoscopic prostatectomy (RALP), retropubic radical prostatectomy (RRP), androgen deprivation therapy (ADT), or radiation therapy.
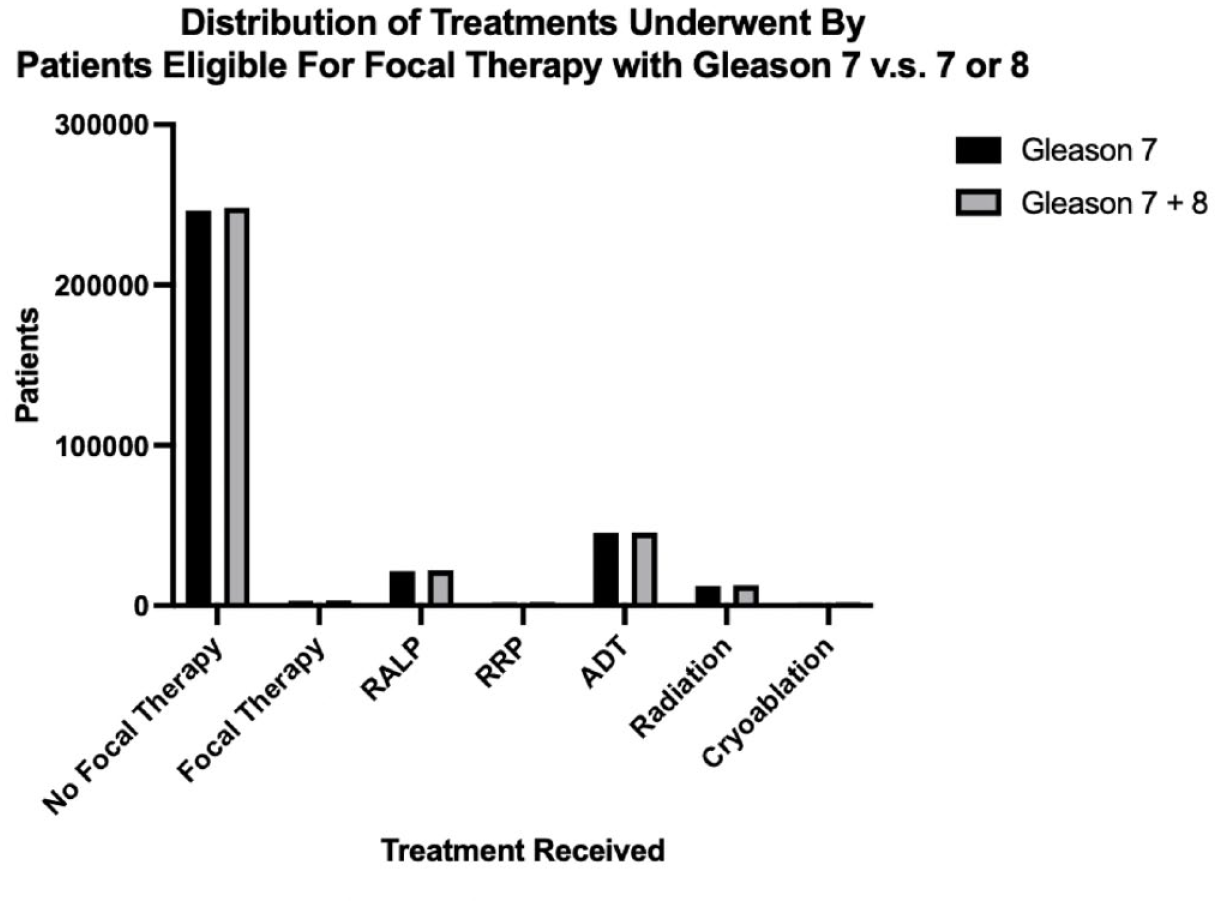
Results: A total of 110,805,357 patients in the database were searched to identify 838,126 with a diagnosis of prostate cancer. Utilizing the more stringent search criteria consistent with guideline recommendations of no greater than Gleason 7 disease, a total of 249,250 patients were identified for Group A. Using the more liberal search criteria including both Gleason 7 and Gleason 8 disease, 251,093 patients were included in Group B as potential candidates for Focal Therapy. Our first cohort using guideline recommendations of no greater than Gleason 7 disease identified 249,250 patients who met the criteria for focal prostate therapy. Of this group, only 2,991 patients (1.2%) had a corresponding CPT code possibly representing some form of FT. Androgen deprivation therapy is the primary the alternative option (18.4%), followed by robotic-assisted prostatectomy (8.7%), radiation therapy (4.9%) and radical retropubic prostatectomy (0.8%). The remainder of the patients (65.16%) possibly received active surveillance, declined treatment, or were missing or omitted due to coding issues. Our second cohort of patients with a Gleason score of either 7 or 8 showed marginal differences in patient counts. 251,093 patients were identified who met this expanded criterion for focal prostate therapy, of which only 2,995 patients (1.2%) had a corresponding CPT code possibly representing some form of FT; the addition of a Gleason score of 8 resulted in only 4 additional patients who may have had some form of FT. Similarly, androgen deprivation therapy remained the primary the alternative option (18.5%), followed by robotic-assisted laparoscopic prostatectomy (8.6%), radiation therapy (3.9%) and radical retropubic prostatectomy (0.73%).
Conclusion: Focal therapy is currently very rarely employed. Accurate determinations of the number of eligible patients are limited by the current CPT codes and the TriNetX database. The addition of Gleason 8 prostate cancers does not dramatically expand the potential pool of candidates for FT in this dataset. Regardless of the eligibility criteria, a large number of men are potentially candidates for FT. Specific coding for FT is needed to better track utilization of this modality.
Post-Cryoablation MRI and Biopsy Performance Characteristics
Piroz Bahar1, Eugene Oh1, Matthew Jordan2, Matthew S. Davenport3, Abhinav Sidana4, Arvin K. George5
1University of Michigan Medical School, USA, 2University of Michigan, USA, 3Michigan Medicine, Department of Radiology, Department of Urology, 4University of Cincinnati Medicine, Division of Urology, USA, 5Johns Hopkins Medicine, Brady Urological Institute, USA
Introduction: Assessing oncological success following focal ablation for prostate cancer (PCa) includes measuring PSA response and imaging. However, the value of protocol biopsy remains under scrutiny. Despite consensus recommendations recommending follow-up multi-parametric MRI (mpMRI) and biopsy, the quality of imaging, interpretation, and biopsy performance is variable. We aim to determine mpMRI performance characteristics post-ablation for in-field (i.e., within the planned ablation zone) failure following focal cryoablation.
Methods: Patients receiving focal cryoablation from 01/01/2017 to 04/21/2023 were enrolled in a multi-institutional, IRB-approved, prospective registry. Per protocol, PSA, mpMRI, and ultrasound-MR fusion prostate biopsy of the ablation bed were obtained at 6 months following prostate ablation. Residual PCa was suspected at mpMRI if there was hypervascularity and impeded diffusion at the margins of the ablation zone. Sensitivity, specificity, positive predictive value, and negative predictive value of post-ablation mpMRI for Gleason Grade Group ⩾2 PCa was calculated. Chi-squared test was used to perform bivariate analysis.
Results: 84 patients undergoing 94 cryoablations were enrolled (mean age: 70.5 years; 92% Caucasian; mean pre-ablation PSA: 9.52 ng/mL [SD±6.97ng/mL], mean pre-ablation PSA density: 0.21 ng/mL/cc [SD±0.17ng/mL/cc]). 1.2% (1/84) of patients had Maximum PI-RADS v2 score 2, 4.7% (4/84) PI-RADS 3, 58.3% (49/84) PI-RADS 4, 34.5% (29/84) PI-RADS 5, and 1.2% (1/84) unscored. Pre-ablation biopsy showed 4.8% (4/84) grade group 1, 73.8% (62/84) grade group 2, 16.7% (14/84) grade group 3, 3.6% (3/84) grade group ⩾4, and 1.2% (1/84) unscored PCa. Post-primary-ablation mpMRI and biopsy were performed in 69 patients; 10 patients required repeat cryoablations, of which 7 underwent post-ablation mpMRI and biopsy (N=76 post-ablation events). Post-ablation mpMRI showed possible residual cancer in 11.7% (9/76). Post-ablation biopsy of the target lesion showed grade group ⩾1 PCa in 13.7% (10/73) and grade group ⩾2 PCa in 9.6% (7/73) patients. MpMRI sensitivity, specificity, positive predictive value, and negative predictive value for detecting grade group ⩾2 PCa in targeted biopsy post-ablation were 71.4%, 95.5%, 62.5%, and 96.9%, respectively. Chi-squared test of the primary analysis showed a significant association between suspicion of residual disease on MRI and biopsy pathology [p<.001]. Secondary analysis excluding post-repeat cryoablation data (N=66) was 71.4%, 94.9%, 62.5%, and 96.6%, respectively.
Conclusion: Post-ablation mpMRI has a high negative predictive value, specificity, and sensitivity for detecting residual grade group ⩾2 PCa and when negative, could be used to defer near-term prostate biopsies to determine oncologic control post cryoablation. Future research investigating causes of false positive and false negative post-ablation mpMRI will help identify those who warrant per-protocol biopsy.
Imaging the Ice Balls Using Low Field in Office MRI System for Focal Prostate Cryotherapy
Haydar Celik1, Muller Gomes1, Aleksandar Nacev1, Srirama Venkataraman1, James Bennett2, Prithipal Sethi1,3
1Promaxo, Inc., Oakland, CA, USA, 2Midtown Urology, Atlanta, GA, USA, 3Golden State Urology, Sacramento, CA, USA
Introduction: Percutaneous transperineal prostate cryoablation is a modality used in the treatment of prostate cancer (1) and can be used for complete or focal partial gland ablation (2). In this study, Promaxo MRI, a low-field MRI system (Promaxo Inc, Oakland, CA), was used to image an ice ball to show the feasibility of this system for cryoablation procedures. Furthermore, the low field MRI system is single-sided, eliminating any possibility for obstruction in accessing the prostate during surgical operation.
Methods: The feasibility study was done on in vitro bovine sample using a low-field MRI operating between 55mT and 74mT. A ground bovine meat was made into a ball and frozen overnight in a freezer. The ball is then covered with fresh ground bovine meat to represent the ice ball and surrounding tissue. This in vitro sample was scanned using a scout and then T2 weighted sequences. After an hour, the phantom was scanned again with the same sequences.
The MRI sequence included permanent z gradient as the readout (Superior-Inferior) and phase encoding is done in x (Right-Left) and y (Anterior-Posterior) directions. A 3-dimensional spiral, fast spin echo sequence was used to include a total volume of 4.8cc. Images were reconstructed immediately after acquisition on the MR imager and used for further analysis. A series of fast xSPEN scans were used to monitor the formation the ice ball in the phantom as well.
Results: The frozen part of the in vitro sample was hypointense with the fresh meat providing hyperintense signal similar to high field systems (1.5Tesla, 3Tesla, etc). Once the frozen meat was completely thawed, the contrast between the previously frozen fresh bovine meat completely disappeared as shown in figure 1 below. Figure 2 shows the formation of the ice ball in a gel phantom over time.
Comparison of initial scan with ice ball in the middle (left) and result after the ice ball melts (right).
Example of how ice ball formation can be monitored over time using the Promaxo scanner. A new frame is added to the time series every two minutes, using a fully sampled xSPEN pulse sequence.
Discussion: Seeing the ice ball is an important feature of a percutaneous cryoablation procedure (3). The ice balls created during cryoablation have been shown to be hypointense in MR images that can be effectively monitored during the formation (4). The same characteristics were shown here using the Promaxo MRI system. Furthermore, it has be shown that the formation of the ice ball can be monitored over time using the Promaxo scanner.
Conclusion: This initial feasibility study demonstrates the capability of imaging ice-ball using a low-field, in-office MRI system cleared by FDA for prostate cancer biopsies and treatment. Monitoring the formation of the ice ball in real time may also be feasible if MRI real time imaging techniques are used in conjunction with the fast imaging sequences used to collect the data in figure 2. In the future, a commercially available cryoablation system will be used to create the ice ball to show the practicality of the operation in a more clinical setting with active temperature monitoring.
Note:
Therapeutic Advances in Urology cannot be held responsible for errors or inconsistencies contained within the abstract supplement. Only formatting alterations have been made and abstract content remains consistent with what was entered at time of submission by the author/s.