
Abstract
Introduction:
Urothelial carcinoma can arise from the urinary bladder or from the upper urinary tract. In some instances, urinary bladder cancer (UBC) and upper tract urothelial carcinoma (UTUC) can be concurrently diagnosed, necessitating a combined radical cystectomy (RC) with radical nephroureterectomy (RNU). A systematic review was done on the combined procedure exploring outcomes and indications, in addition to a comparative analysis between the combined procedure and cystectomy alone.
Methods:
For the systematic review, three databases (Embase, PubMed, and Cochrane) were queried, selecting only studies that included intraoperative and perioperative data. For the comparative analysis, using the NSQIP database, CPT codes for RC and RNU were used to identify two cohorts, one with RC and RNU and one with RC alone. A descriptive analysis was performed on all preoperative variables, and propensity score matching (PSM) was performed. Postoperative events were then compared between the two matched cohorts.
Results:
For the systematic review, 28 relevant articles were included amounting to 947 patients who underwent the combined procedure. The most common indication was synchronous multifocal disease, the most common approach was open surgery, and the most common diversion technique was using an ileal conduit. Almost 28% of patients required blood transfusion and remained in the hospital for an average of 13 days. The most common postoperative complication was prolonged paralytic ileus. For the comparative analysis, 11,759 patients were included of which 97.5% underwent RC only and 2.5% underwent the combined procedure. After PSM, the cohort that had undergone the combined procedure showed an increased risk of renal injury, increased readmission rates, and increased reoperation rates. Whereas the cohort that had undergone RC only showed an increased risk of deep venous thrombosis (DVT), sepsis, or septic shock.
Conclusion:
A combined RC and RNU is a treatment option for concurrent UCB and UTUC that should be cautiously utilized as it is associated with high morbidity and mortality. Patient selection, discussion of the risks and benefits of the procedure, and explanation of the available treatment options remain the most important pillars in managing patients with this complex disease.
Introduction
Urothelial carcinoma can arise throughout the urinary tract and can be broadly divided into upper tract urothelial carcinoma (UTUC) and urinary bladder cancer (UBC). More than 90% of urothelial carcinomas arise from the bladder, whereas UTUC constitutes only 5–10% of all urothelial carcinomas. 1 UBC accounted for around 573,000 new cases of cancer worldwide in 2020, making it the 10th most commonly diagnosed malignancy. 2 It also resulted in 200,000 deaths globally. 3 Radical cystectomy remains the gold standard treatment for muscle-invasive bladder carcinoma (MIBC) 4 and recurrent high-risk non-MIBC. 5 However, radical nephroureterectomy with bladder cuff excision is the treatment of choice for high-risk non-metastatic UTUC. 6
UBC and UTUC have histopathological similarities and share common risk factors, 7 so the possibility of synchronous tumors should be considered. In patients with primary diagnosed UTUC, the presence of a concomitant bladder tumor is around 17% and can be as high as 33% depending on the primary tumor location. 8 In comparison, the incidence of UTUC is 2.6% for patients with primary diagnosed superficial bladder tumors. 9 This highlights the multifocal nature of urothelial carcinoma and that any primary urothelial tumor is an important risk factor for developing another tumor along the rest of the urinary tract. 10
The management of concurrent UTUC and MIBC is challenging, but in certain instances, a combined one-step nephroureterectomy and radical cystectomy is needed11–13 since it allows for decreasing the morbidity of a staged procedure and avoiding the anesthetic risk of multiple surgeries. In other instances, patients with end-stage renal disease (ESRD) and urothelial carcinoma could be considered for a combined procedure involving both upper tracts known as complete urinary tract extirpation (CUTE).11,14 This treatment strategy precludes the need for urinary diversion in such patients and obviates the risk for metachronous recurrence in the urinary tract.
The literature regarding concurrent unilateral or bilateral nephroureterectomy and radical cystectomy is scarce and mostly involves small case series and case reports. The aim of this study is to perform a systematic review of the literature on concurrent radical cystectomy and nephrectomy procedures, and describe the indications, clinical outcomes, and procedure safety. Moreover, using the American College of Surgeons – National Surgical Quality Improvement Program (ACS-NSQIP) database, we sought to compare the combined procedure to radical cystectomy alone, which is classically known to be more morbid than radical nephrectomy.
Methodology
Systematic review
Nephroureterectomy is indicated concurrently with radical cystectomy in some clinical situations. Data regarding the perioperative outcomes of this combined procedure are scarce and needed in order to provide patients with optimal surgical care when taking the decision to perform a concurrent cystectomy and nephrectomy.
The systematic literature search was initially performed in December 2020 using Embase, PubMed, and Cochrane databases. The search was done using MeSH terms and keywords. ‘Cystectomy’, ‘urinary bladder’, ‘urinary bladder neoplasms’, and ‘urinary diversion’ combined with ‘nephrectomy’ were the main MeSH terms adopted. The search was complemented with the use of different combinations of keywords synonyms of the two procedures with asterisks for potential variants, including but not limited to: heminephrectomy, nephroureterectomy, bladder excision/removal, and kidney excision/removal. No limits were applied.
Two authors (N.F.A.H. and M.Z.) separately reviewed all results to select relevant studies and case series of concurrent nephroureterectomy with radical cystectomy. Few discrepancies were resolved by open discussion.
Our review included studies reporting perioperative outcomes and complications only. All non-comparative studies reporting intraoperative and perioperative data (operative time, blood loss, transfusion rate, lengths of hospital stay, complication rates) and oncologic data (cancer-free survival, cancer-specific survival, overall survival) of the combined procedure were collected.
Studies mainly describing surgical technique, staged procedures, or single case reports were not included in our review. After discussing the studies at hand and due to the very limited number of articles meeting our criteria, we decided to include data from congress abstracts.
Data from all selected papers were extracted, summarized, and plotted in Excel sheets. Weighted averages were calculated for all numerical variables (age, operative time, estimated blood loss, etc.). Categorical variables were stratified, and rates/percentages were reported based on the overall number of patients included.
There was heterogeneity among the studies in reporting oncological outcomes. None of them included survival analysis except one. 15 Therefore, it was not possible to summarize and draw conclusions from these variables.
Comparative analysis
Patient population
The study population consisted of patients who underwent RC with or without concurrent RN or RNU and were listed in the ACS-NSQIP between 2005 and 2017. The ACS-NSQIP is a multinational database that provides data on patients undertaking major surgical procedures. The database includes more than 150 variables, encompassing demographic factors, preoperative medical history, laboratory values, intraoperative factors, and 30-day postoperative morbidity and mortality outcomes. Data collection is performed by certified surgical clinical reviewers and is directly listed onto the ACS-NSQIP registry. Quality is assured using an intra-rater reliability (IRR) audit of participating centers. Procedures are categorized by Common Procedural Terminology (CPT) codes. Radical cystectomy cases had the following CPT codes: 51570, 51575, 51580, 51585, 51590, 51595, and 51596. Radical nephrectomy cases had the following CPT codes: 50220, 50225, 50230, 50234, 50236, 50545, 50546, 50547, 50548, and 50549. The concurrent surgery cohort was identified and combined with the RC-only cohort.
Clinical variables
The analyzed variables included patient demographics, medical history and patient health status, preoperative laboratory findings, and surgical factors. Demographic factors were age, gender, body mass index (BMI), ethnicity, race, smoking status, and alcohol use. Medical history included diabetes, insulin use, hypertension, congestive heart failure (CHF), peripheral vascular disease (PVD), stroke or transient ischemic attack (TIA), hepatic disease including presence of esophageal varices or abdominal ascites, chronic obstructive pulmonary disease (COPD), acute renal failure, kidney dialysis, chronic steroid use, disseminated cancer, unintentional weight loss, bleeding disorders, and systemic inflammation or sepsis. Patient health status was evaluated using the American Society of Anesthesiologists (ASA) classification. Preoperative laboratory findings included serum hematocrit, platelet count, white blood cell count, creatinine, albumin, and international normalized ratio (INR). Surgical factors included surgical approach (open versus minimally invasive), urinary diversion type, and operation time. Outcomes studied included wound complications, infectious complications, renal injury, cardiovascular incidents, mortality, prolonged ventilation, need for reintubation, readmission, and unplanned reoperation.
Statistical analysis
A descriptive analysis was performed on all preoperative variables, associations with concurrent nephrectomy status were determined using the chi-square (χ2) test and independent t-test for categorical variables and continuous variables, respectively. A total of 12 variables with significant difference were considered for propensity score matching (PSM). Matching was performed with a match tolerance on 0.001. After matching, the association of postoperative events incidence with concurrent RC/RN status was assessed using the chi-square test. All statistical analysis was conducted using the IBM SPSS Statistics v26 (IBM corp., Armonk NY, USA), and a two-sided alpha level of 0.05 was used to indicate statistical significance.
Results
Systematic review
The initial search strategies on Cochrane, Embase, and PubMed generated 6572 articles. Duplicates (n = 927) were removed and 5645 articles were left for screening. The screening by title and abstract excluded 5561 studies that were irrelevant to concomitant nephroureterectomy and radical cystectomy.
A total of 84 resultant articles were sorted into 36 case reports and 48 larger studies and screened again by full text. Case reports as well as articles purely describing surgical techniques, staged procedures, or other irrelevant results were excluded.
In total, the review of literature yielded 28 relevant articles that were mostly case series and a few cohorts that described perioperative outcomes and complications of concurrent radical cystectomy and nephroureterectomy.
In total, 12 articles originated from Europe, out of which 4 were from Germany. Eight articles were from East Asia, with all except one being from Taiwan. Six articles were from the United States, and 1 article stemmed from Turkey and Chile each.
Patient demographics
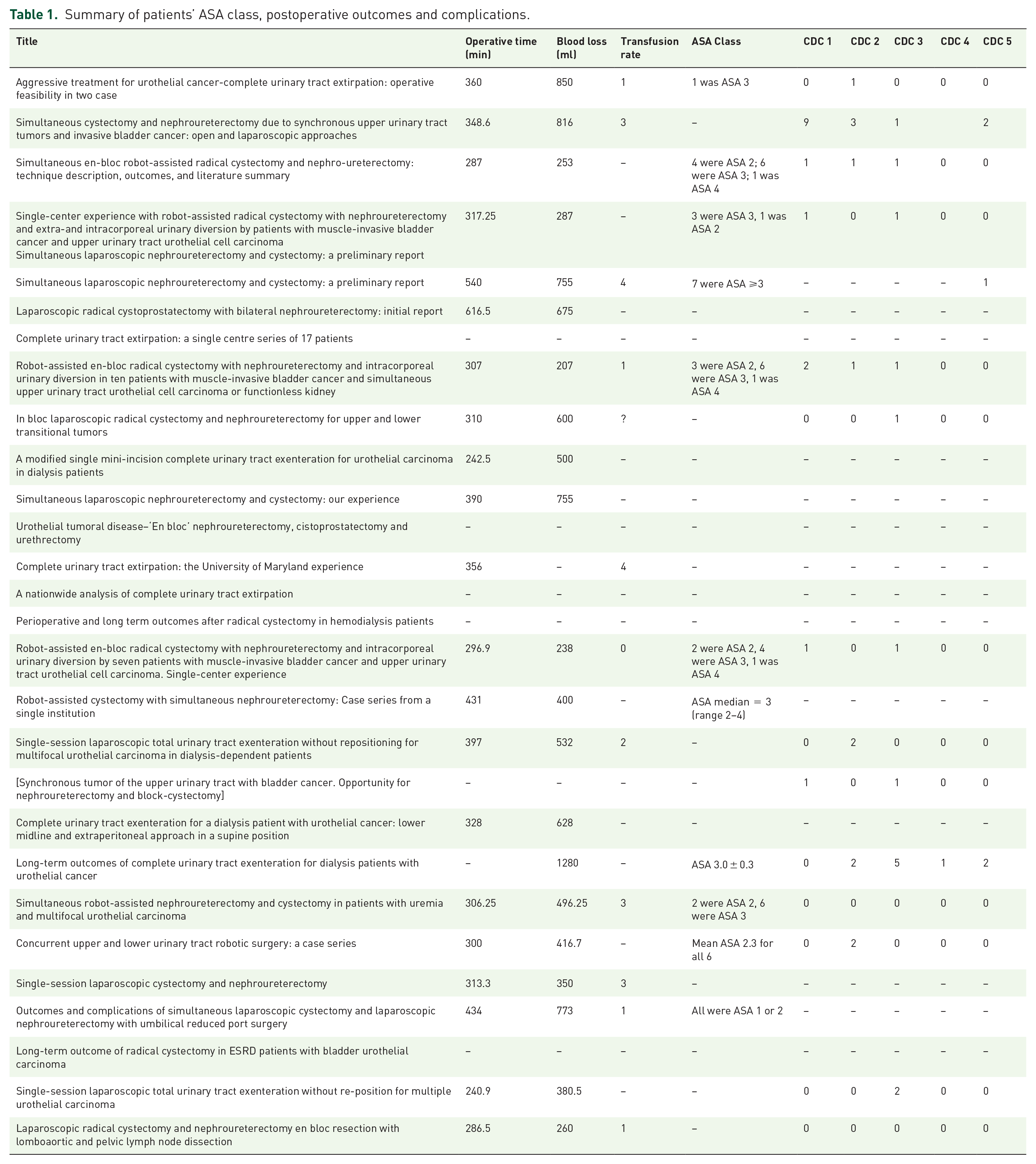
Review of the 28 studies published from 2006 till 2020 included 947 patients that underwent concurrent nephroureterectomy and radical cystectomy. Mean weighted age was 66.54 years (range, 35–89 years), and 67.4% of patients were males. Of studies that reported patient comorbidity profiles using the ASA classification, 73.5% of patients were ASA class ⩾3 (Table 1).
Summary of patients’ ASA class, postoperative outcomes and complications.
Surgical indication, bilateral versus unilateral nephroureterectomy
Almost all indications for radical cystectomy were muscle-invasive transitional cell carcinoma or recurrent high-risk superficial TCC of the bladder (98.4%). The indications for concurrent nephroureterectomy were more varied, with the majority (70.3%) being synchronous multifocal transitional cell carcinoma involving the upper urinary tract, some of which included patients with known ESRD and underwent bilateral concurrent nephroureterectomy known as complete urinary tract extirpation.14,16–19 The next most common indication was a unilateral non-functional kidney20–24 which accounted for 11.3% of the cases. ESRD,25,26 concurrent renal cell carcinoma in two cases,11,26 autosomal dominant polycystic kidney disease, 11 bilateral complex renal cysts, 11 and multiple oncocytomas 23 were also indications in individual instances. Overall, out of 947 patients, 426 (45%) received radical cystectomy with bilateral concurrent nephroureterectomy (Table 2).
Summary of reviewed studies, surgical approach and procedure indication.
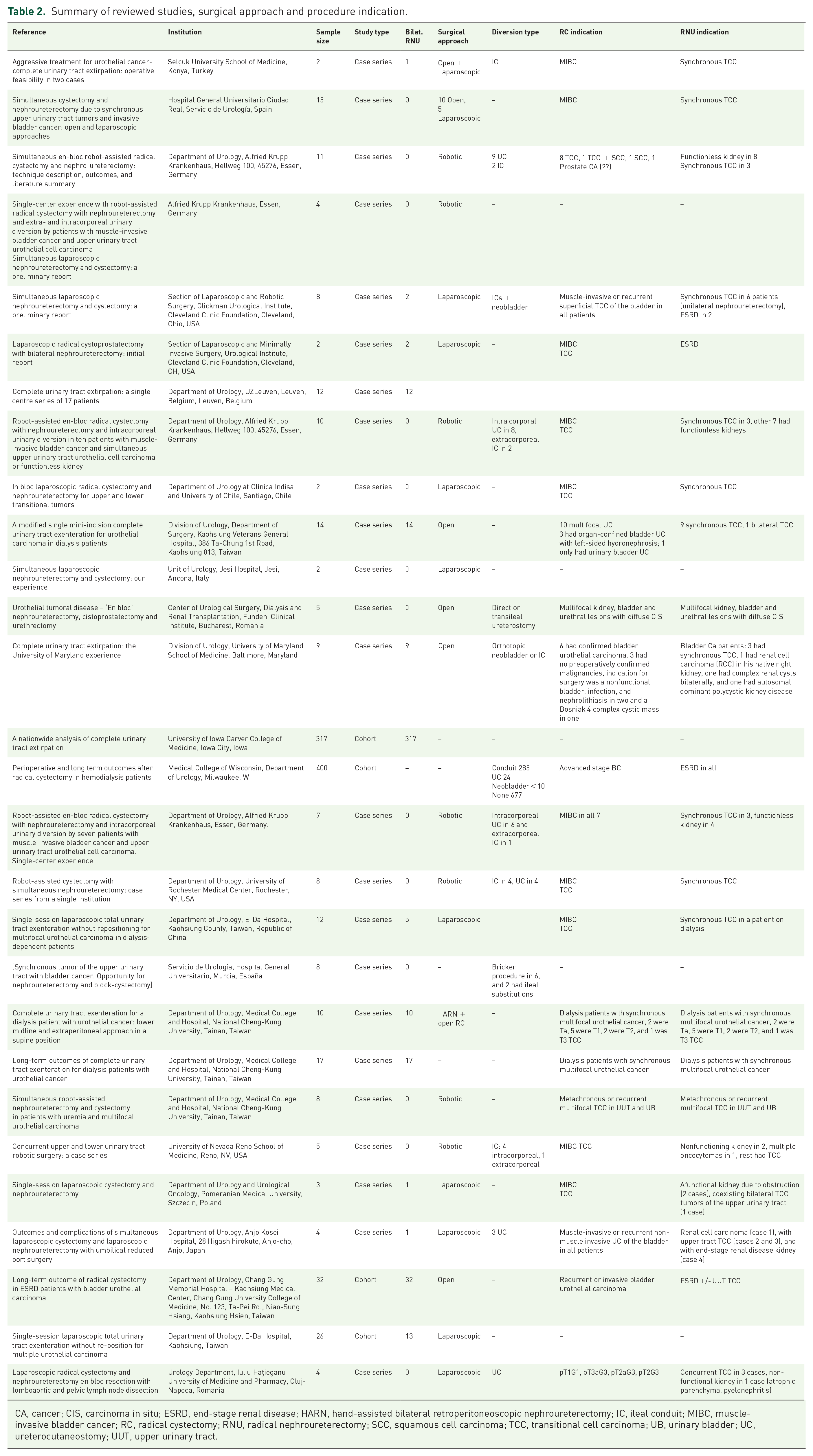
CA, cancer; CIS, carcinoma in situ; ESRD, end-stage renal disease; HARN, hand-assisted bilateral retroperitoneoscopic nephroureterectomy; IC, ileal conduit; MIBC, muscle-invasive bladder cancer; RC, radical cystectomy; RNU, radical nephroureterectomy; SCC, squamous cell carcinoma; TCC, transitional cell carcinoma; UB, urinary bladder; UC, ureterocutaneostomy; UUT, upper urinary tract.
Surgical approach and diversion type
Regarding surgical approaches, open surgery was performed in 35.7% of cases, laparoscopic surgery was adopted in 32.9%, and robotic-assisted surgery in 25.2%. In two cases, a combined approach using open radical cystectomy and laparoscopic nephroureterectomy was done. 12 In 11 cases, bilateral hand-assisted retroperineoscopic nephroureterectomy (HARN) and open extraperitoneal cystectomy were the approaches of choice. 17
For patients requiring urinary diversion, an ileal conduit was the most common diversion method, accounting for nearly 82% of diversions. Other patients had ureterocutaneostomies (15.2%), and continent diversions using a neobladder were relatively rare (2.9%) (Table 2).
Perioperative outcomes and complications
Total operative time was reported by most studies, with the mean being 352.8 min (range, 240.9–616.5 min). Weighted mean for estimated blood loss during the procedure was 578.6 ml (range, 207–1280 ml), and approximately 28% of patients received blood transfusions. Length of hospital stay was indicated by most series with a weighted mean of 13 days (range, 6–36 days) on average.
Regarding postoperative complications, some articles adopted a descriptive classification for listing complications while others used the Clavien-Dindo Classification (CDC). 27 In the former studies, the most commonly described complications were prolonged paralytic ileus,28,29 infectious-related adverse events, 15 and postoperative mortality.13,28 Other mentioned complications were acute kidney failure, 28 ureter-intestinal anastomosis leak, 28 port hernia, 22 and retroperitoneal hemorrhage 30 A total of 47 patients from the included studies had a CDC for complications. From these articles, class I, II, and III adverse events were reported as 32%, 25.5%, and 28.8%, respectively.
Comparative analysis
A total cohort of 11,759 patients was included in the NSQIP database analysis. In total, 11,465 (97.5%) underwent radical cystectomy only, and 294 (2.5%) underwent concurrent radical cystectomy and radical nephrectomy. Before matching, the cohort was significantly different in race, ethnicity, preoperative creatinine, insulin dependence, hypertensive status, history of stroke or TIA, preoperative renal failure, preoperative dialysis, presence of disseminated cancer, use of steroids for chronic conditions, ASA classification, operative time, and urinary diversion type. Table 3 shows the summary of demographic factors, laboratory results, medical history, and operative factors of the entire cohort stratified by concurrent surgery status.
Summary of demographic factors, preoperative laboratory results, medical history, and operative factors for the RC-only and concurrent surgery cohorts, before propensity score matching.

ASA, American Society of Anesthesiologists; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; INR, international normalized ratio; pRBC, packed red blood cell; PVD, peripheral vascular disease; RC, radical cystectomy; SIRS, systemic inflammatory response syndrome; TIA, transient ischemic attack.
The cohort was matched using the 12 significantly different preoperative and operative variables, as highlighted in Table 3. The matched cohort comprised of 510 patients, with 255 (50%) patients undergoing cystectomy only or concurrent RC and RN. After matching, the only significantly different preoperative or operative variables were smoker status (p = 0.039) and alcohol consumption prior to operation (p = 0.001). Table 4 provides the summary of all demographic, laboratory, medical, and operative factors of the matched cohort stratified by concurrent RC and RN status.
Summary of demographic factors, preoperative laboratory results, medical history, and operative factors for the RC-only and concurrent surgery cohorts, after propensity score matching.

ASA, American Society of Anesthesiologists; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; INR, international normalized ratio; pRBC, packed red blood cell; PVD, peripheral vascular disease; RC, radical cystectomy; SIRS, systemic inflammatory response syndrome; TIA, transient ischemic attack.
The matched cohort outcomes showed an increased risk of renal injury (p = 0.007), particularly the need for dialysis postoperatively (p = 0.045), as well as increased readmission rates (p < 0.001) and unplanned reoperation (p = 0.001) for patients undergoing concurrent RC and RN. On the contrary, cystectomy alone showed an increased risk of deep venous thrombosis (p = 0.015) and sepsis or septic shock (p = 0.028). Table 5 provides the full summary of 30-day outcomes for the matched cohort.
Summary of 30-day postoperative outcomes in the propensity score matching cohort.

CI, confidence interval; DVT, deep venous thrombosis; MACE, major adverse cardiovascular events; OR, odds ratio; PE, pulmonary embolism; RC, radical cystectomy; SSI, surgical site infection; UTI, urinary tract infection.
Discussion
Urothelial carcinoma is notorious for being a multifocal disease of the urothelial lining of the whole urinary tract whether in the bladder or the upper urinary tract. This causes urothelial carcinoma to present occasionally as synchronous lesions in the upper urothelial tracts as well as the urinary bladder. In such scenarios, the literature is scarce regarding the optimal management of patients with concurrent localized invasive urothelial carcinoma of both the bladder and the upper tracts. We sought to perform a systematic review of concurrent nephroureterectomy and cystectomy in order to determine the associated complications as well as the oncologic outcomes. Furthermore, we utilized the ACS-NSQIP database to derive the perioperative complication rates in a large national cohort and to compare those rates to patients undergoing cystectomy alone.
Concurrent nephroureterectomy and cystectomy is a surgical procedure with non-negligible complication rates. Our review showed that significant postoperative complications affect about a third of the patients undergoing this surgical procedure. The most commonly stated complications include prolonged paralytic ileus,28,29 infectious-related adverse events, 15 acute kidney failure, 28 ureter-intestinal anastomosis leak, 28 port hernia, 22 and retroperitoneal hemorrhage. 30 In this study, we found that the most commonly encountered complications are surgical site infections (11%), renal failure (9%), and other infectious complications (20.6%). When compared to radical cystectomy alone, we found that renal injuries and unplanned re-operation rates are significantly higher. Kidney injury is intuitively expected due to the removal of a kidney. On the other hand, the increased rates of re-operation are a testament to the increased complexity of performing a concurrent nephroureterectomy and cystectomy when compared to radical cystectomy alone. Interestingly, urinary tract infections were significantly lower in the concurrent group, which could be explained by less uretero-intestinal anastomoses (one or none in concurrent group) when compared to the general population undergoing radical cystectomy (two uretero-intestinal anastomoses). Thus, given the morbidity of the combined procedure, the indication of a concurrent nephroureterectomy should be restricted to cases where benefit is thought to outweigh these demonstrated risks. This is especially relevant for concurrent nephroureterectomies that were performed in the setting of a nonfunctional asymptomatic kidney or other low-risk indications.
The oncologic outcomes of concurrent nephroureterectomy and cystectomy could not be compared due to the lack of proper statistical analysis given the nature of the reviewed papers in our study. Most papers were small case series that reported oncologic outcomes heterogeneously with different follow-up periods. A large-scale study focusing on oncologic outcomes with proper survival analysis is needed to answer this question. However, multifocal disease affecting multiple urinary organs might confer worse oncologic outcomes when compared to focal disease, partly due to the complexity of the curative surgery which could affect recurrence rates, but also possibly related to the inherent biologic and genetic behavior of such tumors. Moreover, systemic therapy alone or in combination with curative surgery remains another role player that may affect oncologic outcomes. This highlights the importance of patient selection and individualized treatment plans as there is no size that best fits all.
Comparing outcomes of different surgical approaches for a combined radical cystectomy and nephroureterectomy, mainly open versus minimally invasive, was not feasible due to the nature of the available literature and diversity of used approaches within the cases series. However, this can be foreseen to a certain limit from comparative studies of minimally invasive versus open radical cystectomy. Robotic-assisted surgery in RC has lower blood transfusion rate but longer operative times when compared with open surgery, with all other outcomes being comparable.31,32
Conclusion
The treatment of concurrent UBC and UTUC is a challenging task requiring a multidisciplinary approach. A combined RC and RNU is a treatment option that should be cautiously utilized as it is associated with high morbidity and mortality. Intraoperative and postoperative complications are worse when compared with RC alone. Oncologic outcomes of this combined operation need to be further investigated and notably compared with RC. This highlights the need for further research as well as exploration of other treatment options such as a staged procedure or other nonsurgical treatments tailored to this complex disease.