
Abstract
Introduction:
With several single-use ureteroscopes now available, our aim was to analyze and compare data obtained globally from high-volume centers using both disposable and reusable flexible ureteroscopes and see if indeed in real-world practice either scope has a distinct advantage.
Methods:
Retrospective analysis was performed on the FLEXOR registry, which was created as a TOWER group (Team of Worldwide Endourological Researchers, research wing of the Endourological Society) endeavor. Patients who underwent retrograde intrarenal surgery (RIRS) for renal stones from January 2018 to August 2021 were enrolled from 20 centers globally. A total of 6663 patients whose data were available for analysis were divided into Group 1 (Reusable scopes, 4808 patients) versus Group 2 (Disposable scopes, 1855 patients).
Results:
The age and gender distribution were similar in both groups. The mean stone size was 11.8 mm and 9.6 mm in Groups 2 and 1, respectively (p < 0.001). Group 2 had more patients with >2 cm stones, lower pole stones and of higher Hounsfield unit. Thulium fiber laser (TFL) was used more in Group 2 (p < 0.001). Patients in Group 2 had a slightly higher stone-free rate (SFR) (78.22%) and a lower number of residual fragments (RFs) compared with Group 1 (p < 0.001). The need for further treatments for RF and overall complications was comparable between groups. On multivariate analysis, overall complications were more likely to occur in elderly patients, larger stone size, lower pole stones, and were also more when using disposable scopes with longer operative time. RFs were significantly higher (p < 0.001) for lower pole, larger, harder, multiple stones and in elderly.
Conclusion:
Our real-world practice observations suggest that urologists choose disposable scopes for bigger, lower pole, and harder stones, and it does indeed help in improving the single-stage SFR if used correctly, with the appropriate lasers and lasing techniques in expert hands.
Introduction
Retrograde intrarenal surgery (RIRS) has established itself in mainstream guidelines1–3 as a safe alternative to percutaneous nephrolithotomy (PCNL) in managing renal stones. 4 A 2 cm cut-off is considered suitable for RIRS and instrument and lithotripsy advancements help push the upper limit of stone volume that can be managed with RIRS and as technology changes its periodically reviewed by the guidelines committee as well. 5
Typically, urologists use reusable or disposable scopes for RIRS. The likelihood of scope damage increases with higher stone volume and stone numbers, which happens due to a reduction in tip deflection 6 or working channel damage. 7 Needless to say, the high repair and procurement costs strains resources and is disruptive to practice. Hence, disposable scopes may be the ideal replacement or compliment reusable scopes. Using a disposable scope each time provides advantages of getting a brand new sterile scope with perfect digital vision and excellent bi-directional deflection and ergonomically much lighter than fiberoptic or digital scopes and absence of sterilization procedures with no hospital infections. 8 Furthermore, newer disposable scopes have smaller calibers and sturdier shafts and tips with much better active and passive deflection that allows access to all parts of the renal collecting system safely and with no risk of scope damage due to maneuverability. 9 Finally, disposable scopes aid in providing training to residents without the worry of expensive repair in case of an accidental scope damage. 10 Many small single-center studies have reported that disposable scopes fare better than reusable scope with regard to stone-free rate (SFR) and infectious complications. 11 Moreover, the quality and effectiveness of sterilization of the reusable RIRS scopes is constantly being questioned and several studies have addressed this. 12
Since the successful launch of Lithovue disposable scope in 2016, several scopes have flooded the market with each claiming better features and aimed at overcoming the shortcomings of reusables. 11 Our aim is to analyze data obtained globally from high-volume centers using both disposable and reusable scopes and see if indeed in real-world practice either scope has a distinct advantage minimizing the residual fragments (RFs) post lithotripsy, and complications specifically fever and sepsis rates post-operatively, when used with different lasers and adjunct when tackling calculi in specific locations, size, and numbers.
Methods
Study population and design
Retrospective analysis was performed on the FLEXOR registry, which was created as a TOWER group (Team of Worldwide Endourological Researchers, research wing of the Endourological Society) endeavor. A total of 6669 patients who underwent RIRS for renal stones from January 2018 to August 2021 were enrolled from 20 centers globally, and only expert consultants who had performed more than 500 RIRS cases using both disposable and reusable scopes were invited to contribute cases.
A total of 6663 patients whose data were available for analysis were divided into Group 1 (Reusable scopes) versus Group 2 (Disposable scopes). Decision to use a reusable or disposable scope and the brand of the scope was totally at the discretion of the surgeon based on availability and preference.
Only adult patients (⩾18 years old), with normal calyceal anatomy, were enrolled. Patients with ureteric stones, anomalous kidneys, bilateral renal stones, and planned endoscopic combined intrarenal surgery (ECIRS) were excluded from this study. Clinically significant residual fragments (CSRFs) defined as single fragments >2 mm or multiple fragments of any size requiring further treatments were assessed as per local practice with kidney, ureter, and bladder (KUB) X-rays and ultrasound or computed tomography scan.
As this was a retrospective data entry and as practices vary globally based on available resources, no strict criteria on how to choose which scopes or which brands were applicable.
Statistical analyses
Baseline characteristics of the patients, presenting complaint, stone size, multiplicity, location, and perioperative characteristics, were analyzed. Categorical variables are reported as absolute numbers and percentages, while continuous variables are reported as mean and standard deviation (SD). Kolmogorov–Smirnov test was used to check data distribution for normality and data on demographics, Hounsfield unit (HU), greatest transverse diameter, single versus multiple, location, type of lasers, intraoperative, postoperative complications, and surgical time assessed. These characteristics between the two groups were analyzed using Pearson’s chi-square test and t-test. Outcomes of surgery including length of hospital stays, presence of CSRF, and complications from surgery were analyzed using Pearson’s chi-square test and t-test as well.
A multivariate logistic regression (MV) analysis was performed to predict the likelihood of overall complications and RF. The covariates being analyzed were age, sex, recurrence stone, stone size, multiple stones, lower pole (LP) stone, and pre-stenting. All statistical analyses were done using the IBM SPSS statistics, version 26 (IBM Corp, Armonk, NY). We considered two-tailed p-value less than 0.05 to be statistically significant.
Results
Patients’ demographics are shown in Table 1. Patients (n = 6663) were divided into two groups. A total of 4808 patients were in Group 1 while 1855 patients underwent RIRS in Group 2. The age and gender distribution were similar in both groups with majority of patients aged 41–65 years old. Disposable scopes were more commonly used among Asian patients (74.61% versus 25.39%).
Patient demographics and stone characteristics.
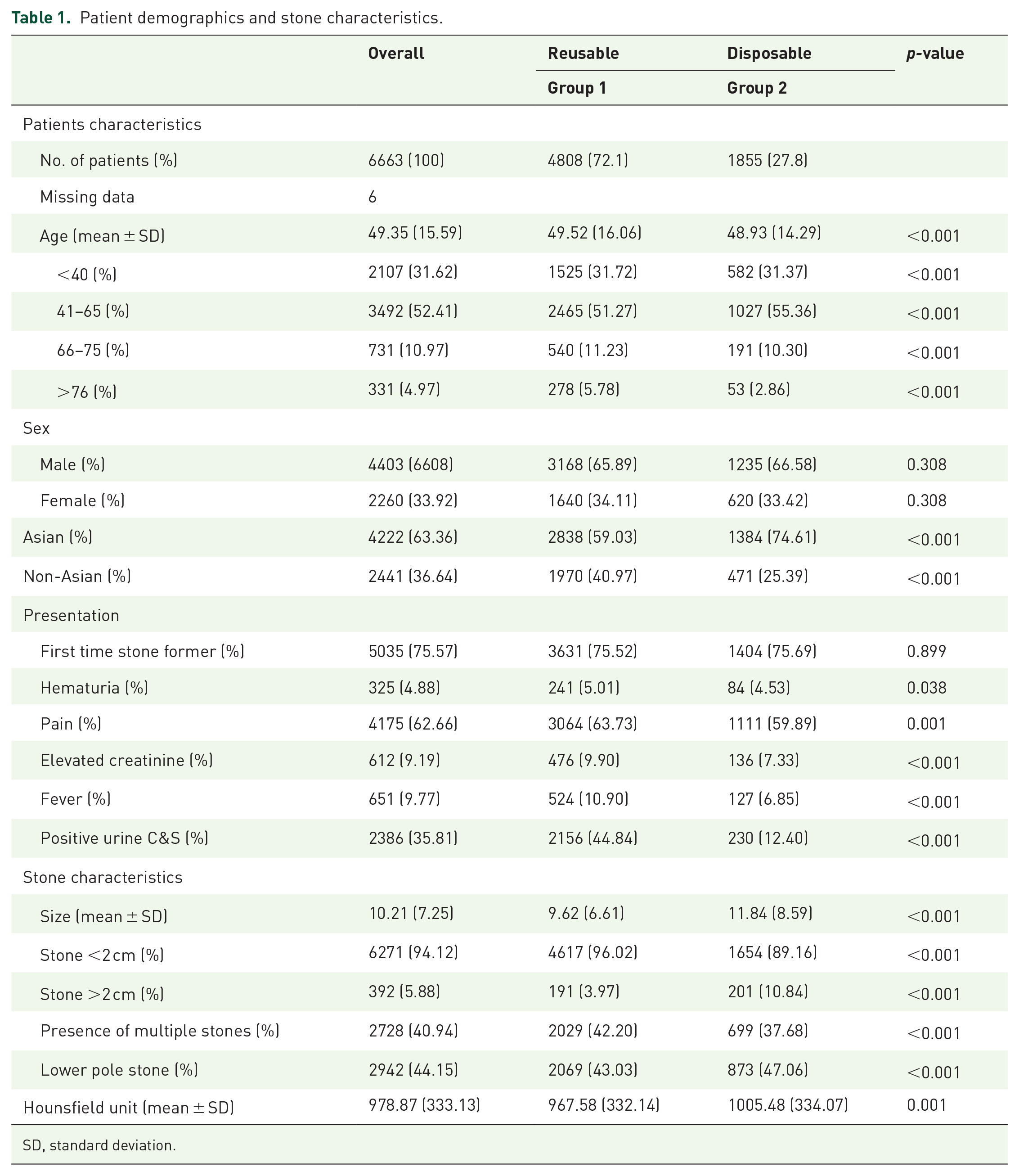
SD, standard deviation.
Statistically significantly (p < 0.001) higher number of symptomatic patients for pain (3064 versus 1111), fever (524 versus 127), elevated creatinine (476 versus 136), positive pre-op culture (2156 versus 230) and with multiple stones (2029 versus 699) were seen in Group 1.
Looking at the stone characteristics (Table 1), the mean stone size of patients in Group 2 (11.84 mm) was bigger than that in Group 1 (9.62 mm) (p < 0.001). A subgroup analysis also showed Group 2 had more patients with stone larger than 2 cm (201, p < 0.001), lower pole stones (47.06% versus 43.03%) and of higher Hounsfield Unit (1005.48 versus 967.58).
With regard to perioperative findings (Table 2), mean operating time was longer in Group 2 (78.37 min versus 57.67 min, p < 0.001). Almost half of the patients in both groups had preoperative stenting, and majority of patients in Group 2 utilized ureteral access sheath (UAS) during surgery (99.62%). Significantly higher number of patients in Group 1 had laser lithotripsy with Holmium lasers, especially using MOSES (8.74% versus 5.12%, p < 0.001). Thulium fiber laser (TFL) was used more in Group 2 (53.69% versus 26.85%, p < 0.001). In the reusable scopes, 79% were fibreoptic and 29% were digital scopes.
Perioperative findings of the groups.

SD, standard deviation; UAS, ureteral access sheath.
Mean hospital stay was longer in Group 1 (3.96 versus 2.52 days) (Table 3). Patients in Group 2 had a slightly higher SFR (78.22%) and a lower number of RFs compared with Group 1 (1210 versus 404, p < 0.001).
Perioperative outcomes of the groups.

CT, computed tomography; ECIRS, endoscopic combined intrarenal surgery; ESWL, extracorporeal shock wave lithotripsy; ICU, intensive care unit; PCNL, percutaneous nephrolithotomy; RF, residual fragment; RIRS, retrograde intrarenal surgery; SD, standard deviation.
There can be considerable interobserver heterogeneity in reporting RF using multiple modalities and as a computed tomography (CT) scan is more sensitive to reporting RF. When this was strictly applied overall, the number of RF reported were only 12.31% from 24.22%, an almost 50% reduction. Furthermore, RF in the reusable/Group 1 was reported significantly lower (11.21% versus 15.15%, p < 0.001) (Table 3). This reiterates that imaging modality has a very big influence on RF assessment post endoscopic intervention. The need for further treatments for RF and overall complications was comparable between both groups.
On multivariate analysis (Table 4), overall complications were more likely to occur in elderly patients, larger stone size, lower pole stones, and were also more when using disposable scopes with longer operative time. RFs were significantly higher (p < 0.001) for LP, larger, harder, multiple stones and in elderly. Disposable scopes were not associated with higher RF.
Multivariate logistic regression analysis of incidence of overall complications and residual stone fragments (SF).

CI, confidence interval; OR, odds ratio.
Discussion
Significant differences in physical and optical properties of single-use or reusable flexible ureterorenoscopes exist, which have a variable influence on surgical efficacy during RIRS. 13 RIRS is an accepted safe intervention, 14 and advancement in size, optics, and lithotripsy adjuncts have put RIRS on center stage in minimally invasive intervention for renal stones up to 2 cm as a less invasive alternative to PCNL. 4 To date, the FLEXOR study by the TOWER group is the largest real-world registry reporting on the outcome of RIRS exclusively for renal stones only using disposable and reusable scopes with different lasers from 20 centers worldwide.
Bozzini et al. reported a very high overall SFR of 90% versus 86.6% in their prospective analysis of 180 patients undergoing RIRS with disposable and reusable scopes and recommended using disposable scopes as they had significantly lesser complications and shorter hospital stay. In our registry, all centers used both reusable and disposable scopes. We reported a better operative outcome in Group 2 patients, with higher SFR and lower incidence of RF (21.78% versus 25.17%) despite the fact that Group 2 had bigger, harder (higher HU), and higher number of stones in lower pole and larger number of stones >2 cm as well. 11 Possibly, we can infer that in such situations and locations, surgeons want to maximize having good vision/deflection and flow characteristics which is exactly what a new disposable scope offer upon each use8,9 and hence could account for the good outcomes and higher utilization of disposable scopes.
This was cited by other studies and in particular it has been observed that as lower pole stones are the most significant risk factor for flexible ureteroscope damage, single-use ureteroscopes could be preferentially used in anatomically difficult cases where a greater degree of deflection is needed and the probability of the instrument damage is higher.4,15
An unquestionable advantage of adding disposable scopes to one armamentarium is that it can help preserve a reusable scope’s longevity. 6 Kramolowsky et al. 16 reported that on average a fiberoptic reusable scope needs repair/maintenance after 21 uses, while upkeep of digital scopes ranges from 10 to 21 uses. Besides that, Ozimek et al. 17 reported that infundibulo-pelvic angle of 60° or less translate to exaggerated deflection which is a risk factor for scope damage. A common recommendation to preserve scope longevity is to displace the lower pole stone to a better location for easier lithotripsy. 6 However, often the stone size and Pelvicalyceal system (PCS) anatomy is not favorable for some. Hence, in situ lasering with a thin laser fiber may be the best way to tackle the stone and here disposable scopes have proven to be equal, if not better, than their more expensive reusable counterparts.18,19 In our study, in situ dusting was the preferred means of lithotripsy in Group 2, with lesser fragmentation and extraction than Group 1.
FLEXOR had patients enrolled where RIRS was done in normal PCS only using both types of scope. However, disposable scopes completely negate the element of wear and tear and maintenance all together. Perhaps that’s why they are the preferred choice by most surgeons when anticipating complex RIRS surgery 20 and also in anomalous kidneys. García Rojo et al. 21 reported that in 249 cases with renal anomalies (60.1%), a disposable scope was used, and the global trend was toward using smaller and disposable scopes.
Literature has mixed reports on the outcome with some studies showing no significance difference 22 and some like Bozzini et al. 11 reporting better outcomes with disposable scopes. Mazzucchi et al. 23 explained that a reduced deflection and an impaired vision of a heavily used scope could contribute to poorer SFR outcome for RIRS. SFR is dependent on multiple factors, including stone volume, expertise, lasers used, and stone location. 24 Our multivariate analysis reflected that disposable scopes may contribute to minimizing RF and help improve the single-stage SFR. The Reducing Operative Complications from Kidney Stones (ROCKS) collaborative reported that in 1817 ureteroscopy procedures, 2.4% of patients were hospitalized secondary to infectious complications. 25 The Clinical Research Office of the Endourology Society (CROES) evaluated 11,885 patients undergoing ureteroscopy (both semirigid and flexible for renal and ureteric stones) and reported that postoperative fever occurred in 1.8% of patients with 1.0% of patients developing a urinary tract infection (UTI) and 0.3% of patients becoming septic. 26 In the MV analysis of our study, disposable scope was associated with higher overall complications. However, when we analyze the implications closely, transient fever needing only antibiotics was the most common complication and occurred in both groups, and sepsis rates were only marginally more in Group 2. Group 1 patients might have had lesser infective complications as a larger number received preoperative antibiotics following a positive preoperative urine culture (Table 1). This was also reported by Corrales et al. in their meta-analysis and several other studies have identified older patient age, patient comorbidities, renal abnormalities, altered kidney function, pregnancy, history of UTI, infectious stone disease, inadequate antibiotic coverage, stone size, lower pole stones and operative times, and intrarenal pressures (IRP), among several other factors as independent contributing factors for septic complications after RIRS.27–32 However, they did not recommend using a disposable scope to actually minimize the risk of infective complications and hence it remains debatable if disposable scope is indeed an independent risk factor for infective complications. In the overall cohort, an UAS was used in 99.62% of patients (Table 2), which might have contributed to minimizing the risk of high IRP as a significant attributing factor for post-op major sepsis. 28
Female gender is also a well-established risk factor for infectious complications following RIRS.29,30 This was, however, not noted in our study, with an equal gender distribution seen in both groups. In the Multivariate analysis (MVA) of our study, apart from type of scopes, the other significant contributing factors to overall complications were stone size, lower pole stones, and operative times only. Reasonably, increased operating time requires the use of a larger amount of irrigation volume when compared with shorter procedures, and a higher stone burden would also necessitate more operative time, and this could provide more nidus for infection. 31 Yet these complications were not life threatening and transient and did not increase the hospitalization time with Group 2 having a significantly shorter hospital stay.
The aforementioned findings indicate that perhaps earmarking the type of scope itself as an independent risk factor for complications needs further evaluation. Disposable scopes have been favored over reusables to minimize time, costs of sterilization, and proposed as a better alternative to minimize infective complications if reusables are not sterilized well.9,32 Our study does not support this finding as similar profiles of infective complications were noted in both groups. Hence, we would suggest advocating or advertising the use of a disposable scope to minimize infective complications, and if sterilization protocols are safely followed, there is no reason that reusables should be considered inferior.
Limitation and strengths
The FLEXOR registry is likely the largest real-world multinational multicenter study, but being a retrospective study, we were limited by our ability to determine the clinical criteria on how a surgeon decides on type, brand, and size of scope used. We lack the information on how many patients had infective stones aka stones in an infected system 33 as well as preoperative stent dwelling time and antibiotic protocols to provide a detailed insight on cause and management of sepsis. This further limits any subset analysis in the patients who had sepsis.
Besides, from being a retrospective study, the main limitation of our study is the absence of cost analysis between the two cohorts. Being a global multi-center study across multiple health systems, a cost-analysis is not possible as procurement, price of scopes, and insurance disbursement vary across different geographical locations and various health centers. Yet this was a study which had patients managed in a real-world setting and helps shine light on global practice patterns and preferences, as well as the bearing that has on surgical outcomes. We believe these data help urologists and industry partners to consider how best they can use this information to improve scope technology for maximum operative outcomes in a single-stage RIRS especially when dealing with bigger, harder stones in different parts of the kidney. This also indirectly helps in providing data for better preoperative costing based on stone and patient clinical parameters and to provide proof of concept to hospital management systems on why single-use consumables should be integrated into daily RIRS practice.
Having a good vision, excellent instrumentation with good flexibility, irrigation with and without instrument in the working channel, and a good deflection to reach the desired calyx for proper stone access is integral for minimizing the risk of PCS injury, reducing the operative time, and yet ensuring adequate stone disintegration with laser, all of which improves outcomes and minimizes preventable complications. Perhaps as the utility of RIRS as a modality will continue to increase world over,34–37 a new disposable scope each time may just be the correct answer.
Conclusion
Our real-world practice observations suggest that urologists choose disposable scopes for bigger, lower pole, and harder stones, and it does indeed help in improving the single-stage SFR if used correctly with the appropriate lasers and lasing techniques in expert hands. We need more information to make a resolute conclusion that the scope itself is an independent risk factor for complications. With regard to costing, the urologists need to independently decide in their ability to integrate disposable scope in their practice for the aforementioned study findings, based on the nuances of their respective health systems.