
Abstract
Background:
Robotic-assisted simple prostatectomy (RASP) proved to be a sound and effective procedure for bladder outlet obstructive symptoms relief. Routinely, the transvesical (Freyer) or transcapsular (Millin) techniques are performed. A novel approach of near-infrared fluorescence imaging (NIFI)-guided urethra-sparing robot-assisted prostatectomy (Madigan) was recently introduced.
Objectives:
The aim of our study was to evaluate the long-term functional outcomes between the Millin, Freyer, and Madigan RASP.
Design:
This is a single-center, retrospective evaluation of a prospectively maintained Institutional Review Board–approved database.
Methods:
Data from patients who have undergone RASP in our center were prospectively collected. Demographics, prostate size, and preoperative flowmetry parameters were assessed. Questionnaires such as International Index of Erectile Function (IIEF), and International Consultation on Incontinence Questionnaire (ICIQ), International prostatic symptoms score (IPSS) with its quality of life (QoL) score, Male Sexual Health Questionnaire (MSHQ), Overactive bladder questionnaire (OABQ) were administered to every patient preoperatively and during follow-up. We tested composite outcomes (trifecta) defined as a combination of postoperative Q-max >15 ml/s, IPSS score < 8, and absence of complications. We also tested a pentafecta which keeps in account the persistence of antegrade ejaculation (MSHQ > 0) and the erectile function maintenance (∆IEEF < 6).
Results:
Median follow-up was 36 months. Millin, Madigan, and Freyer procedures were performed in 37 (51%), 18 (25%), and 17 (24%) cases, respectively. Trifecta was achieved in 43 (60%) patients. Preoperative ICIQ, postoperative IPSS, postoperative OABQ, and QoL were significantly different between groups (all p < 0.02). Pentafecta was achieved by 14 (20%) patients. The pentafecta group showed a statistically significant advantage in terms of postoperative IPSS and MSHQ (p < 0.01).
Conclusion:
RASP provides an effective and durable relief of obstructive symptoms at long-term follow-up, regardless of the technique, achieving the trifecta in the majority of the patients. The Madigan technique is significantly related to the pentafecta achievement.
Keywords
Introduction
Benign prostatic hyperplasia (BPH) is a common disorder in men aged 50–80 years and is the most common cause of bladder outlet obstruction (BOO) and lower urinary tract symptoms (LUTS).1,2 It is estimated that more than 90% of men will develop at least one episode of LUTS, from which 25% will require surgical intervention for symptoms relief.2,3 Surgical intervention has been considered the standard of care in patients with ineffective medical therapies and cases of complicated LUTS. 4 Historically, open simple prostatectomy (OSP) has remained as a standard therapy for benign prostatic enlargement in men with prostatic adenomas (>80–100 ml). 4 A paradigm shift toward minimally invasive procedures for BOO has surged during the last decades with utilization of bipolar or laser enucleation. Recently, robotic-assisted simple prostatectomy (RASP) has been introduced as an alternative to the different laser enucleation techniques. 5 Due to its feasible and reproducible technique, RASP has gained widespread adoption during the last years. RASP offers improved perioperative clinical outcomes compared with open procedures, with a decreased incidence of hemorrhage, transfusion rate, length of hospitalization, and postoperative complications.5,6 Previous studies have evaluated the composite factors predictive of a favorable outcome, known as trifecta, defined as no perioperative complications, postoperative IPSS < 8, and postoperative Q-max >15 ml/s. Reported factors associated with a favorable trifecta outcome include age, body mass index (BMI), operative time, and estimated blood loss.7,8
Transcapsular and transvesical techniques by Millin and Freyer, respectively, are the most frequent approaches of RASP reported in the literature.9,10 However, these approaches are associated with retrograde ejaculation being unsuitable for young, sexually active men. Recently, a novel approach of near-infrared fluorescence imaging (NIFI)-guided urethra-sparing robot-assisted prostatectomy (Madigan) was described by our center. 11 The Madigan technique showed a higher rate of sexual function, sexual satisfaction, and erectile function, with no differences in perioperative outcomes and complications at 1-year follow-up compared with Millin and Freyer techniques. 12
The aim of this study is to provide our long-term, single-center, functional outcomes between the three RASP approaches and to evaluate a trifecta and pentafecta achievement among the procedures.
Materials and methods
Study design
This study is a retrospective evaluation of a prospectively maintained Institutional Review Board–approved database of RASP performed between June 2012 and May 2020. The research protocol was approved by the ‘Regina Elena’ Institutional Ethics Committee. All procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Exclusion criterions included patients with a prior history of prostatic or bladder cancer, neurological disease, urethral stricture, and a prostate volume <80 cc. Clinical data including age, American Society of Anesthesiology classification status, BMI, International Prostate Symptom Score (IPSS), quality of life (QoL), International Index of Erectile Function (IIEF) score, Male Sexual Health Questionnaire (MSHQ), Overactive bladder questionnaire (OABQ), International Consultation on Incontinence Questionnaire (ICIQ), and prostatic volume (PV) were prospectively collected. PV was measured by transrectal ultrasound, using the ellipsoid formula: height × width × length of the prostate × 0.523. All operations were performed by two experienced surgeons with a Da Vinci Si Surgical System (intuitive Surgical, Sunnyvale, CA, USA). Indications for each surgical approach can be reviewed in the publication by Bove et al. 12
Surgical techniques
Table 1 describes the main steps of each of the surgical techniques. Thromboembolic preventive measures and prophylactic antibiotics were applied in all patients. A Trendelenburg position and a transperitoneal approach were used in all surgeries. A more comprehensive description of each technique is mentioned in another previous study. 10
Minimal invasive simple prostatectomy surgical techniques performed at our center: an overview.
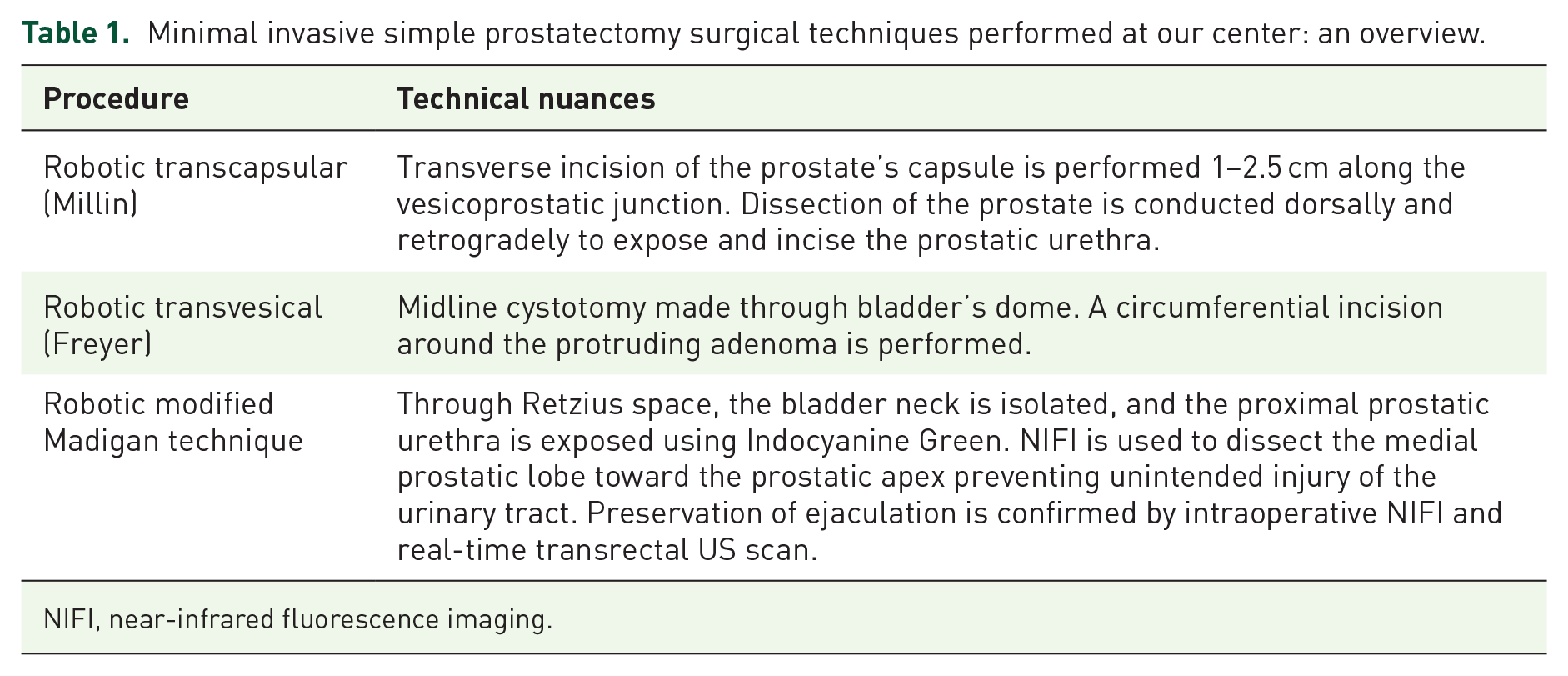
NIFI, near-infrared fluorescence imaging.
Specifically, patients presenting with an ultrasound (US) scan–assessed prostatic median lobe of more than 10 cc, indenting the bladder neck, patients with coexistent bladder diverticula and/or stone underwent RASP according to the Freyer approach. Young and sexually active patients without a prostatic median lobe underwent the RASP according to the urethra-sparing (Madigan) technique. Non-sexually active patients with higher IPSS and lower IIEF score, without evidence of prostatic median lobe, underwent RASP according to the Millin technique.
Intra-operative blood loss was recorded from the suction canisters at the end of the procedure. Perioperative complications were graded according to the Clavien classification system. 13 The IIEF, ICIQ, IPSS, QoL score, MSHQ, and OAB questionnaires were administered to every patient during yearly follow-up, as well as measurement of PVR rate.
We tested composite outcomes (trifecta) defined as a combination of postoperative Q-max >15 ml/sec, IPSS score <8, and the absence of complications. 7 In addition, pentafecta outcomes which keep in account the persistence of antegrade ejaculation (MSHQ > 0) and the erectile function maintenance (∆IEEF < 6).
Statistical analysis
Results were analyzed and compared across the three techniques retrospectively. Continuous and categorical variables were compared between groups using the Mood’s median test and the chi-square tests, respectively. P < 0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS®, IBM, version 24).
Results
Between June 2012 and May 2020, 72 patients underwent RASP at our center. Median follow-up was 36 months. Millin, Madigan, and Freyer procedures were performed in 37 (51%), 18 (25%), and 17 (24%) cases, respectively. The median operative time, defined as console time, was 128.5 min, significantly longer in the Madigan cohort compared to the Millin and Freyer groups (p = 0.05). Blood loss was negligible with every approach (<50 ml).
Trifecta
Trifecta was achieved in 43 (60%) patients (Figure 1). No significant differences were observed between the ‘trifecta achieved’ and the ‘trifecta not achieved’ groups for baseline ASA score, BMI, prostate volume, baseline IPSS, IIEF, and MSHQ scores (all p ⩾ 0.2). Surgical technique was not related to the trifecta achievement. Preoperative ICIQ, postoperative IPSS, postoperative OABQ, and QoL were significantly different between groups (all p < 0.02). Data are shown in Table 2.

Trifecta.
Trifecta application to robotic-assisted simple prostatectomy cohort; median (IQR).
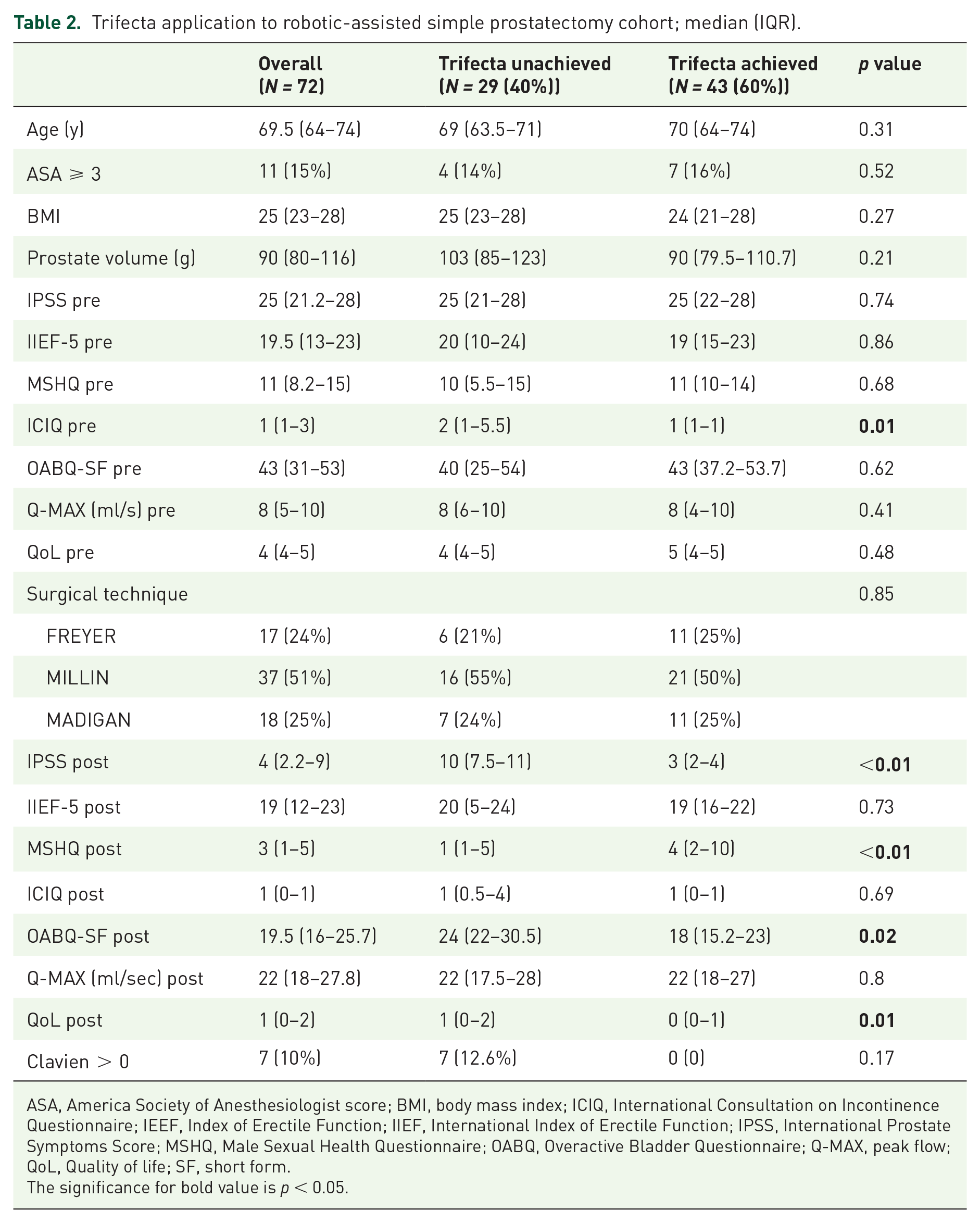
ASA, America Society of Anesthesiologist score; BMI, body mass index; ICIQ, International Consultation on Incontinence Questionnaire; IEEF, Index of Erectile Function; IIEF, International Index of Erectile Function; IPSS, International Prostate Symptoms Score; MSHQ, Male Sexual Health Questionnaire; OABQ, Overactive Bladder Questionnaire; Q-MAX, peak flow; QoL, Quality of life; SF, short form.
The significance for bold value is p < 0.05.
Pentafecta
Pentafecta was achieved by 14 (20%) patients. Surgical approach was significantly related to pentafecta achievement ( p < 0.01; Figure 2). The pentafecta group showed a statistically significant advantage in terms of postoperative IPSS and MSHQ (both p < 0.01; Table 3).

Pentafecta.
Pentafecta application to robotic-assisted simple prostatectomy cohort; median (IQR).
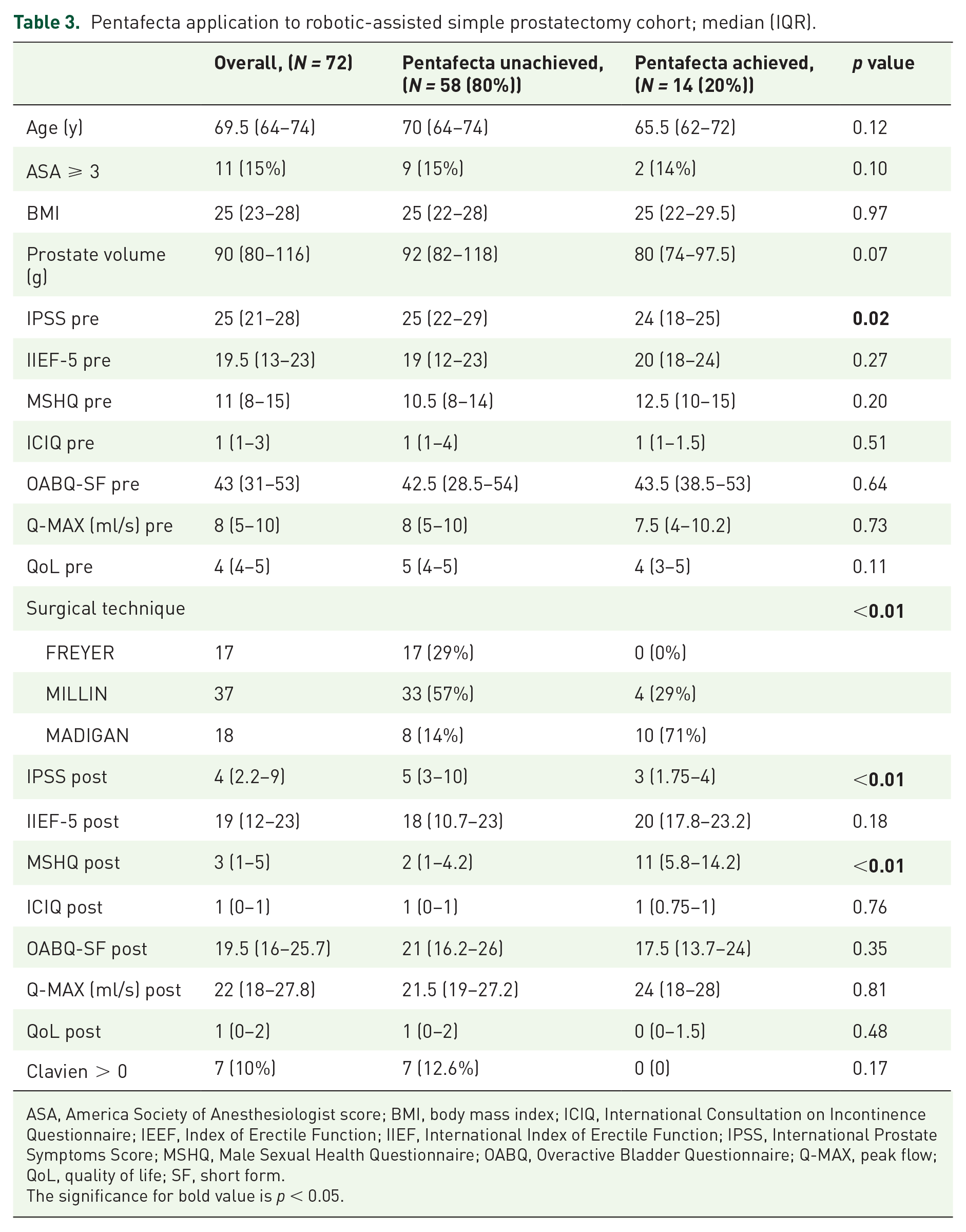
ASA, America Society of Anesthesiologist score; BMI, body mass index; ICIQ, International Consultation on Incontinence Questionnaire; IEEF, Index of Erectile Function; IIEF, International Index of Erectile Function; IPSS, International Prostate Symptoms Score; MSHQ, Male Sexual Health Questionnaire; OABQ, Overactive Bladder Questionnaire; Q-MAX, peak flow; QoL, quality of life; SF, short form.
The significance for bold value is p < 0.05.
Discussion
We analyzed 72 patients treated at our institution comparing the novel Madigan technique with Freyer and Millin approaches for benign prostatic obstruction (BPO). In this article, we report the first study to evaluate the trifecta, pentafecta, and long-term postoperative outcomes across the three RASP techniques. The achievement of trifecta and pentafecta showed a statistically significant postoperative advantage for IPSS and QoL. OSP is the oldest and most invasive surgical approach for BPO. Due to its long-term functional results with reduction of LUTS symptoms, increased mean Q-max, and reduction of post-void residual test, OSP remains as a treatment option for substantially enlarged prostatic adenomas or when concomitant bladder surgery is required. 14 For decades, simple prostatectomy has been performed through an open approach, being the transvesical (Freyer’s) and retropubic (Millin’s) the most used techniques.9,10 Limitations of these techniques include the requirement for major surgery, higher rates of perioperative complications, and most importantly postoperative ejaculatory dysfunction (EjD).15 –17 With the introduction of endourological techniques and novel technology, the performance of OSP is significantly lower. Various endourological modalities are now available for BPO, including laparoscopic resection, RASP, laser vaporesection and enucleation, among others. 13 A recent meta-analysis of minimally invasive prostatectomy showed a similar improvement to OSP, with a decrease in blood loss and shorter hospital stay. 18 Sotelo et al. introduced RASP for the first time in 2008. Thenceforth, it has gained worldwide acceptance due to its improved perioperative clinical outcomes compared with the open procedures, with a decreased incidence of hemorrhage, transfusion rate, length of hospitalization, and postoperative complications.5,6 Despite the range of surgical approaches available, EjD due to retrograde ejaculation represents a major postoperative issue which significantly affects QoL in young sexually active patients. In 1990, the urethra-sparing (Madigan) approach was introduced by Dixon et al. 19 as a surgical alternative for OSP. This technique showed the maintenance of anterograde ejaculation and sexual quality due to the preservation of the prostatic urethra and bladder neck.19,20 The open technique was successfully reproduced by a laparoscopic approach. In 2011, Quan et al. reported their results of 16 case-series in which an extraperitoneal laparoscopic approach (modified Madigan) was performed. Although, the postoperative IPSS and increased mean Q-max were not significantly different between the comparing groups, the time to catheter removal and estimated blood loss was significantly lower in the laparoscopic group. In addition, erectile function was preserved in previously potent patients. 21 Wang et al. described an extraperitoneal urethra-sparing RASP technique. In their case-series, despite a noticeable improvement in the voiding function, 26.9% required urethral repair secondary to inadvertent injury and preservation of antegrade ejaculation was maintained only in 50% of men. 22 In 2018, our center introduced a novel robotic urethra-sparing technique in which visualization of the prostatic urethra was enhanced by utilizing NIFI, and, consequently, the complexity of the Madigan procedure steps was simplified. 11 The instillation of Indocyanine Green (ICG) into the urethra provides the enhancement of the prostatic urethra promoting an adequate urethral contouring and dissection.11,12 ICG reflux through the ejaculatory ducts during transurethral instillation permits the identification and maintenance of the ejaculatory ducts allowing the conservation of the ejaculatory function. This technique showed a preservation of anterograde ejaculation in 71.5% of men with acceptable symptomatology relief, a minimal hospital stay, and minimal blood loss. No increase in perioperative complications were reported compared with Freyer and Millin techniques.11,12 Autorino et al. 7 recently proposed the use of a composite outcome of factors associated with a favorable trifecta surgical result. They defined the trifecta as a combination of postoperative Q-max >15 ml/s, IPSS score <8, and absence of perioperative complications. Since then, it has been externally validated by other authors.8,23 In Autorino’s paper, the achievement of the trifecta was associated with operative time and estimated blood loss. However, these results differ from those reported in the study by Pavan et al., 8 in which only age and BMI were associated with the trifecta. We found that a postoperative trifecta achievement was not associated with baseline patients’ demographics, IPSS, IIEF, MSHQ, OABQ, ICIQ scores, nor surgical technique performed. However, we observed that the trifecta achievement was associated with a significant improvement of IPSS, OABQ-SF, and QoL postoperative scores. Even though a trifecta achievement has been considered as a favorable composite outcome for RASP, sexual function and QoL have not been considered. Sexual dysfunction and low sexual QoL, commonly observed postoperatively in patients after non-urethra preservation RASP, have been associated with a decreased life satisfaction, mood, and relationship quality. 24 To overcome this limitation of the trifecta, we introduced a pentafecta composite outcome which integrates sexual function and satisfaction with the inclusion of an MSHQ > 0 and a maintenance of IEEF < 6. The achievement of the pentafecta was associated with the performed surgical technique. The Madigan technique was the approach with major pentafecta achievement compared with Freyer and Millin techniques. Furthermore, a significant higher MSHQ and IIEF scores were observed in the Madigan cohort at 1-year follow-up. 12 Erectile function was maintained, and an improved sexual function and satisfaction was observed in men with pentafecta achievement. The main strengths of our study are represented by homogeneity of the performed surgical techniques by two experienced surgeons, and the long-term follow-up of the Madigan technique. This is the first study introducing Pentafecta as a composite outcome. Including both obstructing symptoms relief success rate, and sexual function preservation rate, pentafecta allows for a more comprehensive understanding of the overall patients’ well-being and QoL improvements. This tool can hopefully represent a further step toward a more proficient tailoring of surgical approach. The main limitation of our study is its retrospective design, limited number of evaluated patients, and the indication of Madigan technique in mainly younger and sexually active patients. The trifecta and pentafecta were arbitrarily chosen and further validation in distinct studies is required. Randomized controlled trial are needed in order to avoid selection biases. Besides, RASP is still limited by robotic platform availability and cost-effectiveness issues. That said, further randomized controlled trials and cost-analysis studies are needed to widely introduce this technique in clinical practice.
Conclusion
Our findings show that RASP provides an effective and durable alleviation of obstructive symptoms at long-term follow-up regardless of the chosen approach. Notwithstanding, the Madigan technique was associated with a higher pentafecta achievement rate. This technique should be encouraged in young and sexually active patients as it effectively preserves the antegrade ejaculation and enhances meaningful benefits in terms of self-assessed quality of sexual function.