
Abstract
Aim:
To assess the prevalence of anterior vaginal wall dehiscence in women who underwent anterior vaginal wall colpotomy for pelvic organ prolapse or stress urinary incontinence and to evaluate the influence of suture materials and techniques on wound dehiscence.
Materials and Methods:
This multicenter, prospective study enrolled naïve women for urogynecological surgery affected by anterior vaginal wall defect or stress urinary incontinence. Performed surgical procedures were anterior vaginal wall repair (AVWR) with native tissue (N-AVWR) or polypropylene mesh (M-AVWR), trans-obturator polypropylene in-out middle urethral sling (MUS). Used suture materials were Vicryl 2-0, Vicryl Rapide 2-0, and Monocryl 3-0. Suture techniques were running interlocking or interrupted. Follow-up was performed daily during hospitalization and in outpatient clinic after 10–14, 30 days, and after 3 months.
Results:
A total of 1139 patients were enrolled. AVWR were 790: 89.1% N-AVWR, and 10.9% M-AVWR. Polypropylene MUS were 349. Women with prosthetic implantation were 38.2%, while 61.8% had native tissue repair. Overall Vicryl was used in 53.9%, Vicryl Rapide in 37.4%, and Monocryl in 8.7%. Overall running interlocking sutures were 66.5%, while interrupted were 33.5%. Overall wound dehiscence prevalence was 0.9% (10/1139). Wound dehiscence rate of 0.6% (5/790) was documented in AVWR: 0.3% (2/704) in N-AVWR, and 3.5% (3/86) in M-AVWR. Among women underwent MUS, 1.4% (5/349) showed wound dehiscence. In patients who underwent prosthetic surgery, the overall dehiscence prevalence was 1.8% (8/435). A statistically significant higher rate of wound dehiscence was found in women with implanted prosthetic materials.
Discussion:
We reported for the first time the prevalence of wound dehiscence in females who underwent colpotomy for AVWR or MUS. Wound dehiscence occurrence was low, but non-negligible. We found that this complication was poorly associated to the suture methods and materials, while prosthetic material represented a risk factor for wound healing.
Introduction
Anterior vaginal wall repair (AVWR) and the positioning of middle urethral sling (MUS) are the most performed urogynecological procedures worldwide.1,2 These procedures have a low complication rate. However, when prosthetic material is used, exposure is the most reported complication with a rate of up to 14% in MUS, and up to 17% in cystocele repair.3–5
Surgical wound dehiscence may affect any surgical procedure, and it is defined as the separation of opposed or sutured margins.6–9 This complication usually occurs between 7 and 14 days after surgery.8,9 Prevalence of anterior colpotomy dehiscence has never been investigated, and data are available only regarding wound dehiscence after transvaginal hysterectomy.10–12 Wound dehiscence is an early complication, usually associated to symptoms. However, in case of asymptomatic short wound dehiscence, the early diagnosis of this complication may be missed. In patients who underwent prosthetic surgery, the underlying misleading diagnosis of wound dehiscence may be the first step leading to mesh/tape exposure, that is, usually a late complication. Due to the lack of data on wound dehiscence after anterior colpotomy, the correlation between this wound closure and dehiscence is unknown, as also the relationship between wound dehiscence and prosthetic material exposure.
The aim of the study was to assess the prevalence of anterior vaginal wall dehiscence in women who underwent anterior vaginal wall colpotomy for pelvic organ prolapse or stress urinary incontinence. A second purpose was to evaluate the influence of suture materials and suture techniques on wound dehiscence, and the relationship between prosthetic surgery and wound dehiscence.
Materials and methods
This was a multicenter, prospective study involving nine different urological and gynecological departments of Tertiary Hospitals and 13 surgeons experienced in urogynecology. Patients were enrolled between January 2019 and December 2019. Inclusion criteria were naïve women for urogynecological surgery affected by anterior vaginal wall defect or stress urinary incontinence. Exclusion criteria were connective tissues diseases, diabetes, and peripheral vascular disease. Performed surgical procedures were AVWR with native tissue (N-AVWR) or polypropylene mesh (M-AVWR), and trans-obturator polypropylene in-out MUS.
Wound dehiscence was considered as a complete or partial separation of opposed suture margins within 14 days after surgery.6–9 Sagittal, inverted T or U colpotomy, and trimming of excessive vaginal epithelium were avoided in order to reduce the rate of vaginal mesh exposure. 3 Used suture materials were Vicryl 2-0, Vicryl Rapide 2-0, Monocryl 3-0. Suture techniques were running interlocking or interrupted aiming to make a stitch each 5 mm along the entire length of the wound, and passing the point at a lateral distance of 5–7 mm from the incision. Each suture was tight with 5 knots. Surgeons performed colpotomy closure with the suture material and stitching technique usually used.
Data were collected anonymously in a database recording: the suture material; stitching technique; surgical technique data (kind and length of incision, procedure, and operating time); occurrence of wound dehiscence, its length and treatment; dyspareunia; leucorrhea; vaginal discharge; and the duration of vaginal blood spots. Complications were ranked by Clavien–Dindo scale. Follow-up was performed daily during the hospitalization, and in outpatient clinic after 10–14, 30 days, and after 3 months.
Results
An amount of 1139 patients were enrolled. Mean age of women underwent AVWR was 66.8 y.o. (SD ± 10), while for MUS was 62.3 y.o. (SD ± 12). AVWR were 790: 89.1% N-AVWR (704/790), and 10.9% M-AVWR (86/790). Polypropylene MUS were 349. Women with synthetic material implantation, M-AVWR and MUS, were 435 (38.2%), while 704 (61.8%) had native tissue repair.
In all the cases, there was a vertical midline vaginal incision, with a mean length of 1 cm for MUS, and of 4 cm for AVWR. Mean operating time for AVWR was 55 minutes (SD ± 16), while for MUS was 19 minutes (SD ± 11). Mean blood loss for AVWR was 57 ml (SD ± 85), and for MUS 28ml (SD + 34)
Table 1 reports the data on suture materials and suture techniques according to the different anterior vaginal wall surgical procedures.
Sutures and stitching techniques in different anterior vaginal wall surgical procedures.

M-AVWR, mesh-anterior vaginal wall repair; MUS, middle urethral sling; N-AVWR, native tissue anterior vaginal wall repair.
Suture materials
In overall wound closure, Vicryl was used in 53.9%, Vicryl Rapide in 37.4%, and Monocryl in 8.7%. In women underwent N-AVWR Vicryl was used in 53.97%, Vicryl Rapide in 33.6%, and Monocryl in 12.3%. In M-AVWR, Vicryl was the suture material chosen in 58.1% of the cases, Vicryl Rapide in 41.9%. In MUS procedures Vicryl was used in 52.7% of the women, Vicryl Rapide in 43.8%, and Monocryl in 3.4%.
Suture techniques
Overall running interlocking sutures were 758 (66.5%), while interrupted stitches were 381 (33.5%). In women with N-AVWR, running interlocking was done in 674 patients (83.5%), while interrupted stitches were used in 30 (16.5%). In the cases of M-AVWR, 35 had running interlocking (40.7%), while 51 interrupted sutures (59.3%). In women treated with MUS for urinary incontinence, running interlocking suturing technique was performed in 49 patients (14%), while interrupted stitches were utilized in 300 (86%).
Wound dehiscence
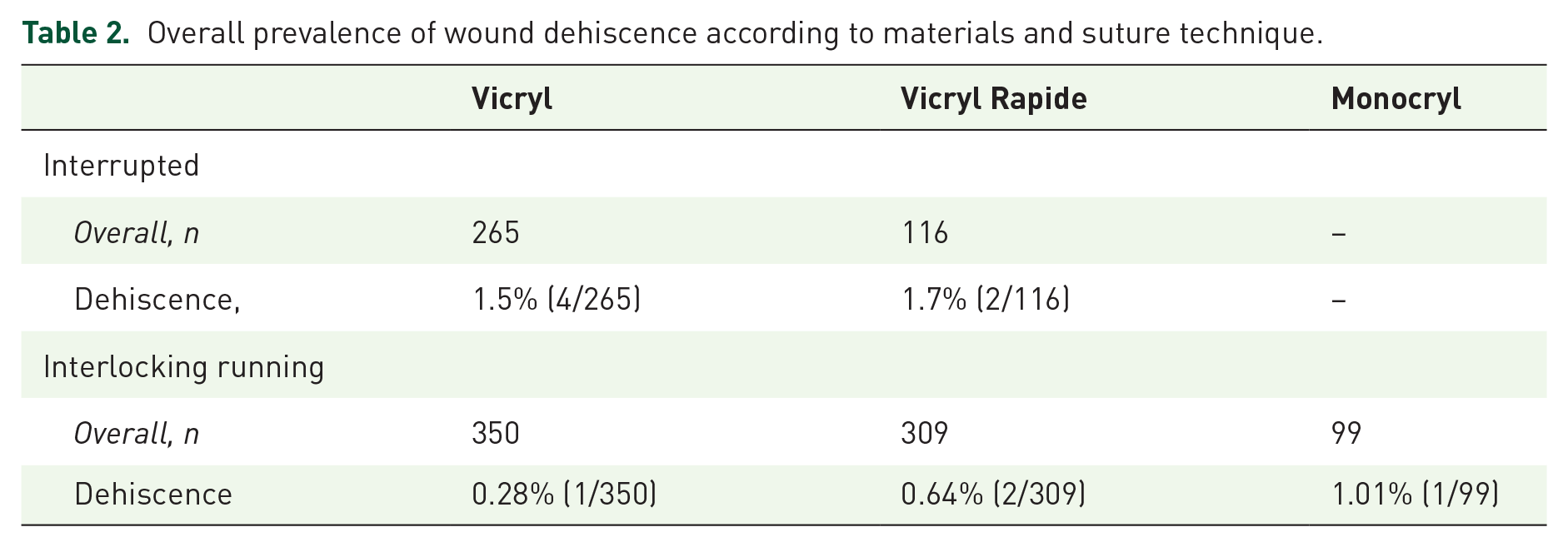
Overall wound dehiscence prevalence was 0.9% (10/1139). Wound dehiscence length ranged from 0.8 to 2.5 cm in AVWR, while in MUS were all lower than 1 cm. Wound dehiscence rate of 0.6% (5/790) was documented in AVWR: 0.3% (2/704) in N-AVWR, and 3.5% (3/86) in M-AVWR. Among women underwent MUS, 1.4% (5/349) showed wound dehiscence. In patients who underwent prosthetic surgery, the overall dehiscence prevalence was 1.8% (8/435). A statistically significant higher rate of wound dehiscence was found in women with implanted prosthetic materials (chi-square test p = 0.0062, with Yates correction p = 0.016). Table 2 reports the overall prevalence of wound dehiscence according to materials and suture techniques; while Table 3 reports the prevalence of wound dehiscence according to the surgical procedures.
Overall prevalence of wound dehiscence according to materials and suture technique.
Prevalence of wound dehiscence of non-prosthetic (N-AVWS), prosthetic surgery (M-AVWS and MUS), M-AVWS, and MUS.
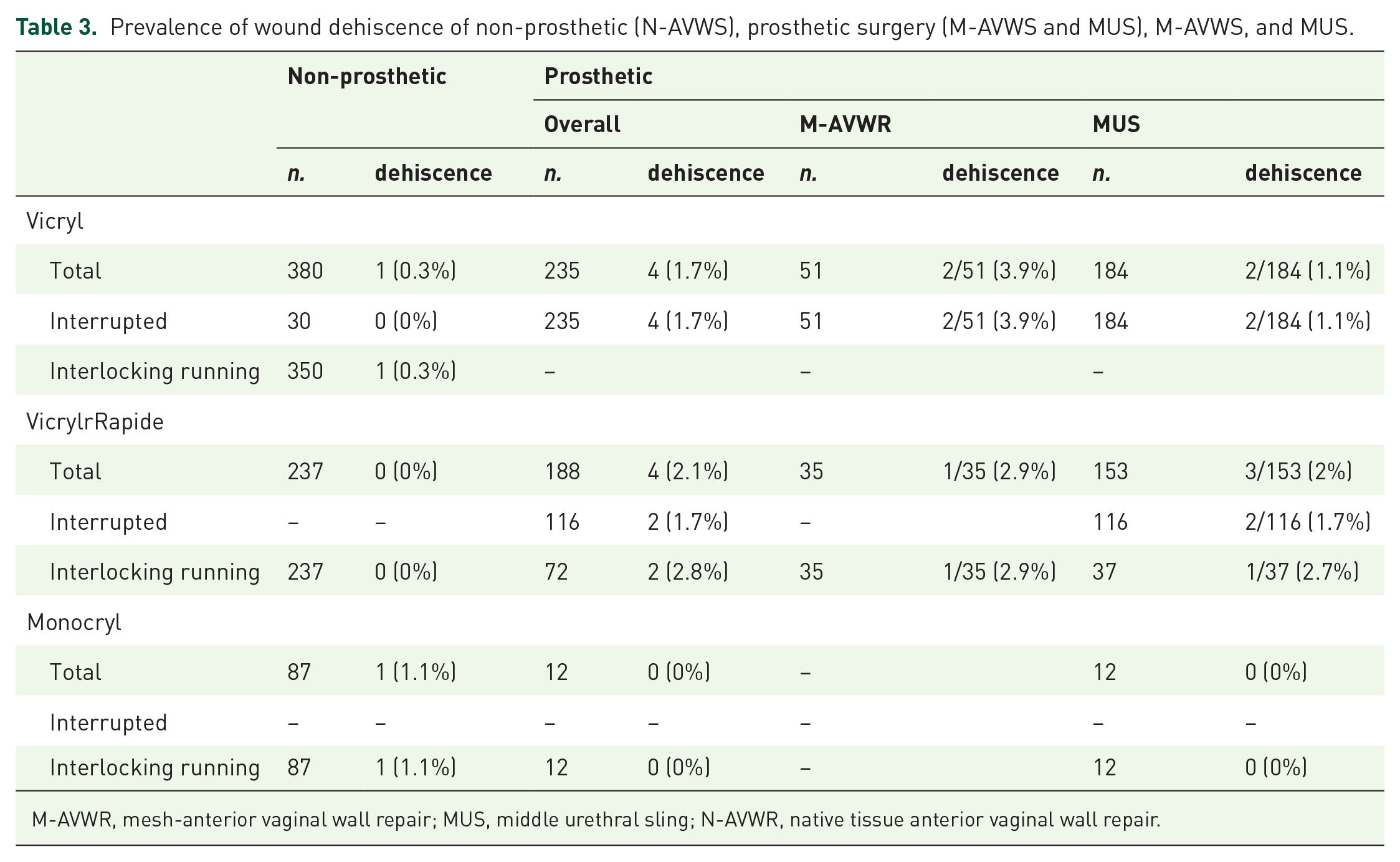
M-AVWR, mesh-anterior vaginal wall repair; MUS, middle urethral sling; N-AVWR, native tissue anterior vaginal wall repair.
Comparing data
We found wound dehiscence in three running interlocking sutures (1 Vicryl, 1 Monocryl, and 1 Vicryl Rapide), and seven interrupted sutures (4 Vicryl, 1 Monocryl, 2 Vicryl Rapide). Overall, using chi-square with Yates test correction, we did not found significant correlation between wound dehiscence and the kind of stitching technique (p = 0.058), nor with the used material (p = 0.66).
Overall, all wound dehiscence with underlying prosthetic material were surgically closed, while the others were conservatively managed. According to Clavien–Dindo scale we had three cases of Grade III complications: two were III a (percutaneous drainage of hematoma) and one was III b (surgical transvaginal drainage of hematoma and blood transfusion). At 3 months, none of the patients had wound healing complication.
Outcomes of surgery at 3 months follow-up did not differ comparing the suture material and/or the suture technique.
Discussion
To date, no data on wound dehiscence in women who underwent anterior vaginal wall colpotomy for pelvic organ prolapse or stress urinary incontinence surgery has been reported. In literature, vaginal wall dehiscence has been evaluated only in case of vaginal cuff dehiscence after hysterectomy with a rate varying from 0% to 7.5%.10–12
Kim et al. assessed the cuff suture method, finding that continuous suture was superior to vaginal approach continuous locking suture. However, continuous suture was done intracorporeal and not by vaginal route. 12
Our research found a low overall prevalence of vaginal wall wound dehiscence (<1%), but not negligible; therefore, the diagnosis and therapy of this complication should not be underestimated. Fatton et al. 13 recognized inverted T colpotomy as a potential cause promoting vaginal wall dehiscence. However, this latter incision was longer than those performed in our study. Indeed, in our series vaginal wall dehiscence occurred despite short vertical colpotomy not exceeding 4 cm, thus less invasive. Therefore, a tiny incision did not preserve from this potential complication.
Our data showed a three-fold increase of wound dehiscence rate in women with implanted prosthetic materials, with a statistically significant difference. Conversely, the sub-analysis comparing wound dehiscence to the materials used and the suture method did not show any significant correlation. It was necessary to provide evidences on the occurrence of wound dehiscence to prove the hypothesis of a relationship between wound dehiscence and materials extrusion. Indeed, it could be postulated that early wound complications may lead to mesh extrusion. Our data showed that implanted patients were at higher risk of wound dehiscence, regardless of the surgical techniques and kind of stiches. Dehiscence occurs in the early post-operative time, usually 5–8 days following surgery, while extrusions with concomitant wound dehiscence are never seen so early. 14 This is a crucial difference between these two complications. Thus, our data evidenced a negative influence of the mesh/tape on the wound dehiscence, and that implantation surgery was a risk factor for wound complication. In literature, prosthetic materials are associated to extrusion of the vaginal mucosa.4,13,15,16,17 However, our findings showed that early wound dehiscence was correlated to synthetic materials; therefore, it is possible that some of the erosions/extrusions have begun as a not identified early asymptomatic wound dehiscence. An explanation of the pathophysiological mechanism is that synthetic materials may affect wound healing, impairing the balance of the vaginal epithelium favoring a dehiscence. 18
Although we found no statistical difference among women underwent AVWR, a higher rate (four times greater) of wound dehiscence was found using Monocryl suture with interlocking technique, compared to Vicryl or Vicryl Rapide. Therefore, in case of AVWR, we suggest the use of Vicryl/ Vicryl Rapide material to close colpotomy. Unfortunately, we could not compare interrupted suture, and this is a limit of our study.
Among patients underwent prosthetic surgery, we did not correlate the results between colpotomy closure by Vicryl/ Vicryl Rapide suture and Monocryl due to the low sample size of this latter group. This was another limitation of our study. However, in women implanted with synthetic material, we found no difference in wound dehiscence rate between Vicryl and Vicryl Rapide suture with interrupted suture method. In patients treated with mesh, wound dehiscence rate was higher when Vicryl was used. The increasing trend of increase of wound dehiscence in MUS was different, showing a higher rate in case of Vicryl rapide. These findings may suggest that Vicryl Rapide was a more efficient material for larger incision, while Vicryl for shorter wound. Unfortunately, a limitation was that we were not able to correlate all the suture techniques in prosthetic patients. However, this was a real practice study design, leading each experienced surgeon to perform their usual colpotomy closure.
Conclusion
We reported for the first time the prevalence of wound dehiscence in females who underwent colpotomy for AVWR surgery or MUS placement for stress urinary incontinence. Wound dehiscence occurrence was low, but non negligible. We found that this complication was poorly associated to the suture methods and materials, while prosthetic material represented a risk factor for wound healing.
Footnotes
Author contributions
Conceptualization: MB, ER, MT, VLM, and MS. Formal analysis: MB, ER, and MG. Investigation: MB, ER, MT, VLM, and MS. Data curation: MB, ER, MT, VLM, MS, VM, MG, EM, OS, AB, SS, GC, and AA. Methodology: MB, ER, MT, VLM, MS, VM, MG, EM, OS, AB, SS, GC, and AA. Supervision: MB, ER, MT, VLM, MS, VM, and AA. Writing—original draft: MB and ER. Writing—review and editing: MB, ER, MT, EM, VLM, and AA.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written informed consent was obtained from all participants. The study was carried out in accordance with the principles of the Helsinki Declaration. The local ethics committee, Comitato Etico Aoui Verona, determined that approval for this investigation was unnecessary, as it only involved anonymised data collecetion and standard clinical practices. This study was registered with our Clinical Audit Department.