
Abstract
Introduction:
Androgenic deprivation therapies have been linked to the development of metabolic syndrome (MS) and cardiovascular diseases, which may lead to a poorer survival in patients with metastatic Castration-Resistant Prostate Cancer (mCRPC). We aimed to analyze whether some cardiovascular or neurological disorders, together with other medical and urological complications, may have an effect on survival outcomes, at baseline and during treatment from patients treated with androgen pathway inhibitors (API).
Material and Methods:
A retrospective study of a consecutive series of patients diagnosed with mCRPC between 2010 and 2018 treated with API in the first line setting in a single center.
Results:
Seventy-three patients met the inclusion criteria. Baseline prognostic factors associated with worse survival were diabetes mellitus (DM) with insulin needs compared to patients without DM [hazard ratio (HR) = 0.19, p = 0.025], hypertension (HTN) (HR = 0.46, p = 0.035), and a history of stroke (HR = 0.16, p < 0.001). However, previous history of hypercholesterolemia, arrythmias, and cognitive disorders did not result in a significant worsening on survival. During treatment, patients who developed de novo HTN had the best progression free survival (PFS) (HR = 0.38, p = 0.048) and overall survival (OS) (HR 0.08, p = 0.012) compared with patients with previous HTN. Other factors related to worse outcomes included the presence of heart failure (HR = 0.31, p = 0.001), the requirement for major opioids for pain relief (HR = 0.33, p = 0.023), and the presence of bilateral ureterohydronephrosis (HR = 0.12, p = 0.008).
Conclusions:
Some comorbidities may be strongly involved in patient outcomes when receiving API for mCRPC. In this sense, collaborative networking between specialists and caregivers treating prostate cancer (PC) patients should be recommended, focusing on MS features, cardiovascular and neurological disorders in order to anticipate medical and surgical complications.
Keywords
Introduction
Prostate cancer (PC) is the most frequent tumor diagnosed in adult males. 1 Approximately 35–45% of patients with treated, localized disease may relapse, while 5–10% are diagnosed with ‘de novo’ metastasis. Fortunately, PC management is increasing in complexity, requiring a multidisciplinary team workflow for an adequate treatment algorithm due to the appearance of new life-prolonging therapeutic options.2–6 In order to optimize this increase in survival, it is also necessary to maintain or improve the quality of life of patients who will live longer.
The mainstay of treatment for patients with metastatic PC is androgen deprivation therapy (ADT). In recent years, several authors have described the relationship between ADT and cardio-metabolic comorbidities. ADT therapy reduces testosterone levels, leading to changes in body composition, lipid profile, and insulin sensitivity.7,8 This has been showed to be related to the development of metabolic syndrome (MS) and cardiovascular diseases (CVD).9,10 MS includes a range of disorders such as hypertension, insulin resistance, weight gain, and dyslipidemia (DL) 11 . These conditions increase the risk of ischemic heart disease (IHD), stroke, and diabetes mellitus (DM) development. All these comorbidities may contribute to an increase in morbidity and mortality from all causes in patients with PC. 12 Two studies specifically assessed the effect of MS in patients treated with androgen pathway inhibitors (API) after progression to docetaxel.13,14 In both studies, those patients with MS presented worse progression free survival (PFS) [4.7 months versus 9 months, hazard ratio (HR) 1.7, 95% confidence interval (CI) 1.2–2.4, p = 0.03 13 and 3.7 months versus 8.7, HR 2.77, 95% CI 2.12–3.61, p < 0.0001 15 ]. However, contradictory results were identified in overall survival (OS) [14.7 months versus 22.3, HR 1.42, 95% CI 0.91–2.22, p = 0.073 13 and 6.9 months versus 19 months, HR 3.43, 95% CI 2.56–4.58, p < 0.0001 14 ].
The duration of ADT could be a key factor in the development of MS.16–19 In fact, more than half of patients who receive ADT for at least 6 months develop MS.20,21 In particular, hyperinsulinemia seems to be the main driver for the development of MS and is responsible for the alteration of the different metabolic pathways such as lipogenesis, steroidogenesis, and protein synthesis. At the same time, this has been suggested to have an important role in carcinogenesis, due to a proliferative and antiapoptotic activity demonstrated in different cell types. 22
Hypogonadism due to treatment with ADT is also associated with hyperinsulinemia and insulin resistance. 23 In this sense, the presence of MS at baseline in patients with mCRPC has been related to a poorer survival, as well as glycemic disorders to a worse response to API. 24
However, positive results have been observed in patients treated with metformin, statins, or with healthy lifestyle habits in different settings of mCRPC.25,26 This mechanism of action is probably leaded by the insulin-like growth factor 1 (IGF1) inhibition thought to be overexpressed in PC as an escape mechanism to hormonal therapy through phosphoinositide 3-kinase (PI3K)/AKT pathway activation. 27
The development of urological complications may contribute to worse survival outcomes. Kobatashi et al. 28 described a greater incidence of urological complications in patients with localized disease treated with ADT, compared with those who received local treatment with radical prostatectomy (RP), [Odd’s ratio (OR) 30.6] or radiotherapy (⩽70 Gy) (OR 5.344). In accordance, other authors found that prior local therapy in advanced disease correlated with lower risk for urological complications compared with those treated only with ADT (32.6% versus 54.6%, p = 0.001). This suggests that the primary prostate tumor burden is relevant in urological symptom control, 29 and even more, its treatment have a potential survival benefit. 30
At present, patients with mCRPC have a longer life expectancy due to the effect of available effective therapies; their treatments can induce metabolic changes with a survival effect. 31 In this sense, an optimal assessment of medical and surgical comorbidities is relevant, as they may have an effect on treatment response and prognosis. To further evaluate the involvement of both medical and surgical comorbidities, in relation to survival outcomes of patients with mCRPC treated with first line abiraterone acetate (AA) or enzalutamide, we have performed the following analysis concerning patients treated in this setting at our PC unit. We have assessed the potential relationship between MS disorders, cardiovascular and neurological alterations at baseline, and throughout the treatment, as well as urological complications with survival outcomes. We have also estimated the potential role of supportive therapy in this setting.
Material and methods
Study design and patients
We retrospectively evaluated a consecutive series of patients with mCRPC treated with gonadotrophin hormone-releasing hormone (GnRH) agonists in combination with AA (1000 mg daily associated with prednisone 5 mg twice daily) or enzalutamide (160 mg daily) in the first line setting outside clinical trials. Patients with a diagnosis of mCRPC between 2010 and December 2018 were included. A data cut-off date of 31 July 2020 was used. The study protocol, called Prostata Centro was approved by the local ethic committee, Comité ético de Investigación clínica Hospital Universitario Ramón y Cajal, on 18 July 2017. Informed consent was waived, due to the retrospective design of the study.
We registered baseline data from the medical records (prior to treatment initiation) that included some metabolic disorders (MD) such as hypertension (defined as blood pressure level >140/90 mmHg), DM, and dyslipidemia [defined as high levels of low density lipoprotein (LDL) cholesterol ⩾ 130 mg/dl], IHD, arrhythmia, stroke, and cognitive disorders (including cognitive impairment and depressive syndrome) as well as their evolution during treatment and until the end of follow up. We also defined cardiovascular events (CVE) as any of the following situations: new hypertension onset, an episode of IHD, new arrhythmia onset, stroke, or any episode of heart failure (HF). In addition, we have evaluated the presence of HF [defined as New York Heart Association Functional Classification (NYHA) ⩾ 3 and/or need for hospitalization], pain management requirements, and the appearance of urological complications, such as obstructive uropathy and hematuria. For urinary problems, we have included the measurement of prostate volume at baseline by a computed tomography at the time of treatment initiation and in a period between three to six months after. Measures were calculated by a single radiologist using the ellipse formula (transversal diameter × anteroposterior × longitudinal × 0.52). The Wilcoxon signed-rank test was used to asses volume variation after treatment, pre-treatment mean volume including patients on AA and enzalutamide.
Statistical analysis
Descriptive statistics were reported as frequencies and percentages for categorical variables and as a mean +/− standard deviation (SD) for continuous variables. Age was categorized into three groups (<65, 65–74, ⩾75) and Gleason score into two groups (⩽7, ⩾8), considering them as categorical variables.
The Shapiro–Wilk test was used to check the normality of quantitative continuous variables (all variables were not normally distributed). A comparison of patients’ characteristics between patients with AA or with enzalutamide was performed using a non-parametric median test (Mann–Whitney test) for continuous variables and the Σ2 test or Fisher-exact test for categorical variables, as appropriate.
Survival curves were estimated by the Kaplan–Meier method. The log-rank test was performed to compare survival curves between different subgroups of the aforementioned variables. A Cox regression model for the univariate analysis was used to investigate potential predictors of PFS and OS and to evaluate their HR and their 95% CI.
PFS was defined as the time from the start of treatment until disease progression or death from any cause. Disease progression was defined according to Prostate Cancer Working Group 2 criteria 32 and Response Evaluation Criteria in Solid Tumors (RECIST). 33 OS was defined as the time from the start of the treatment until death from any cause. Data from patients without events were censored at the last assessment date.
All statistical analyses were carried out using STATA 14. For all the analysis, a 2-sided p-value < 0.05 was considered as statistically significant.
Results
A total of 73 patients were included for the analysis. Basal characteristics are summarized in Table 1. The median age was 70 years (range: 42–84). Patients were treated with AA (N = 44, 60.27%) or enzalutamide (N = 29, 39.73%). In the AA group, there was a higher incidence of patients with previous history of hypertension [AA N = 32 (75.73%) versus enzalutamide N = 14 (48.28%); p = 0.034] and stroke [AA N = 6 (13.64%) versus enzalutamide 0 (0%); p = 0.038]. There were 25 patients (34.25%) with previous CVE.
Baseline patients’ characteristics included in the study.
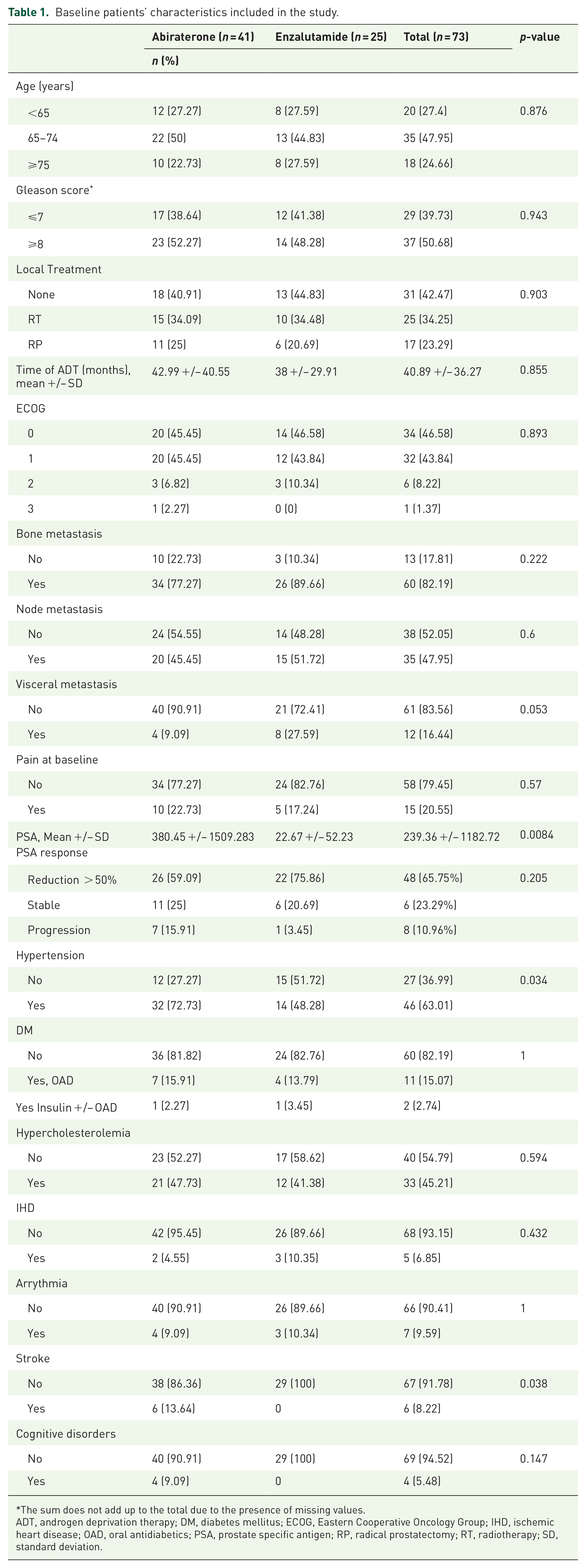
The sum does not add up to the total due to the presence of missing values.
ADT, androgen deprivation therapy; DM, diabetes mellitus; ECOG, Eastern Cooperative Oncology Group; IHD, ischemic heart disease; OAD, oral antidiabetics; PSA, prostate specific antigen; RP, radical prostatectomy; RT, radiotherapy; SD, standard deviation.
The Median follow-up was 24.53 months (range: 1.5–77.59). At the time of analysis, 15 patients (20.55%) were free of disease progression and 43 (58.9%) had died. The most frequent cause of treatment discontinuation was disease progression (N = 42, 57.53%) followed by death and other causes (N = 7, 9.59%, each). The most frequent type of progression was radiological and biochemical (N = 21, 28.77%).
Globally, the median PFS and OS were 15.2 and 32 months, respectively. There were no differences in PFS (HR = 0.67, 95% CI: 0.39–1.17, p = 0.161) neither OS (HR = 0.55, 95% CI: 0.29–1.06, p = 0.075) between both APIs.
Firstly, we analyzed the relationship with survival outcomes of the baseline characteristics before initiating AA or enzalutamide. Considering glycemic control, PFS was superior in those patients without DM (n = 60) in comparison with those with DM (n = 13) (HR = 0.49, 95% CI: 0.26–0.94, p = 0.033). However, when we divided patients according to DM treatment, those given oral antidiabetics (OAD) (n = 11) versus those given insulin (INS) (n = 2), the difference in PFS was only significant for INS (HR = 0.2, 95% CI: 0.04–0.86, p = 0.031), but not for patients given OAD (HR = 0.54, 95% CI: 0.26–1.1, p = 0.09) (Figure 1).

Survival outcomes due to diabetic status before starting treatment with API. HRs were calculated using the status ‘no DM’ as a comparator.
Furthermore, when OS was analyzed, we observed no significant differences between patients without DM versus patients with DM (HR = 0.52, 95% CI 0.26–1.08, p = 0.082). However, once again, when we considered the type of DM treatment, there was a statistically significant improvement in OS in patients without DM in comparison with INS (HR = 0.19, 95% CI 0.04–0.81, p = 0.025), while this difference was not identified in patients undergoing OAD (HR = 0.62, 95% CI 0.28–1.35, p = 0.224) (Figure 1). Patients suffering from previous DM showed adequate controlled baseline hemoglobin A1C (HbA1C) levels, with a mean value of 6.3% (ref. 4.0–6.0%) (range 5.7–7.7%).
A previous history of stroke was only analyzed in the AA group because no patient with this comorbidity was treated with enzalutamide. The results showed that the presence of a previous stroke episode (n = 6) was a predictor of worse PFS (HR = 0.19, 95% CI: 0.07–0.47, p < 0.001) and OS (HR = 0.16, 95% CI: 0.06–0.4, p < 0.001) [Figure 2(a)]. In addition, patients with history of HF (n = 11) had a worse OS (HR = 0.31, 95% CI: 0.15–0.62, p = 0.001) [Figure 2(b)]. We have also found a better OS in patients without a previous history of hypertension (n = 27) (HR = 0.46, 95% CI 0.23–0.95, p = 0.035), and an advantage in PFS in those patients without previous history of IHD (n = 68) (HR = 0.36, 95% CI 0.14–0.94, p = 0.036). There were no differences in PFS or OS considering the other variables (Supplemental material A). Secondly, we analyzed the relationship between new medical complications appearing during AA or enzalutamide treatment and the survival outcomes.

(a) OS due to stroke history. (b) OS due to heart failure history.
Concerning HTN, those patients with an increase in their blood pressure levels (n = 15) (both, patients with de novo HTN and those with a poorer control of their previous HTN) had a significantly better OS compared with those patients in whom blood pressure did not worsen (n = 58) (HR 4.78, 95% CI 1.69–13.55, p = 0.003). However, there were no differences in PFS (HR 1.64, 95% CI 0.86–3.13, p = 0.133). (Figure 3).

Survival outcomes according to HTN evolution. Worse HTN: de novo HTN and poorer control of previous HTN; Stable HTN: rest of the patients.
Interestingly, this difference was also statistically significant when comparing those patients with de novo HTN (n = 8) with those patients who did not require changes in their previous antihypertensive treatment (n = 36) (HR 0.08, 95%CI 0.01–0.57, p = 0.012) and with those patients that did not develop HTN (n = 19) (HR 0.11, 95% CI 0.01–0.91, p = 0.041). (Supplemental material B and C)
The development of hypercholesterolemia or cognitive disorders were not related to worse survival. Patients treated with AA or enzalutamide had a similar risk for the development of DM [p = 0.953 (1 new case in each group)], hypertension [p = 0.23 (3 new cases in the AA group and 5 in the enzalutamide group)], hypercholesterolemia [p = 0.253 (no cases in each group)], and IHD [p = 0.215 (only one case in the enzalutamide group)].
Finally, we considered the assessment of other complications during AA and enzalutamide treatment known to be related with a poor prognosis in mCRPC, such as tumor-related pain and urological complications that are frequently developed in patients with mCRPC. Concerning pain management, only 15 (20.55%) patients reported pain at treatment initiation. In addition, there were 25 patients (34.24%) who required analgesic adjustments due to cancer-related pain and 13 patients (17.81%) achieved an improvement in pain relief. Patients without analgesic adjustments (n = 35) had a better OS than those that required an increase of analgesics to major opioids (n = 7) (HR 0.33, 95% CI: 0.13–0.86, p = 0.023) and, surprisingly, with those with an improvement in their pain management (n = 13) (HR 0.33, 95% CI: 0.14–0.75, p = 0.008). [Table 2 and Figure 4(a)]. Overall, those findings could be probably related with a more aggressive disease.
Description of the incidence of obstructive uropathy in patients with mCRPC included in the study and the different palliative urological treatment approaches.

BOO, bladder outlet obstruction; BUHN, bilateral ureterohidronephrosis; OUP, obstructive uropathy; TUR, transurethral resection; UC, urinary catheter; UUHN, unilateral ureterohidronephrosis.

(a) OS according to pain control. HR are calculated by using the status of ‘No adjustments’ as comparator. (b) OS according to the presence of obstructive uropathy. HR are calculated by using the status of ‘Bilateral UHN’ as comparator.
The prostate volume variation after treatment, pre-treatment mean volume including patients on AA and enzalutamide was 29.18 cc (SD 25.97) and post-treatment mean volume 25.43 cc (SD 32.64), being volume variation statistically significant (p = 0.002). The mean prostate volume was 35.8 cc (SD 32.42) in the enzalutamide group before starting treatment and 30.20 cc (SD 47.30) after treatment (p = 0.03). The mean volume in AA patients prior to treatment was 24.60 cc (SD 19.75) and 22.14 (16.74 SD) after three to six months on treatment (p = 0.051).
Local urological complications were also reported (Table 2). Of the 9 patients (12.33%) who presented hematuria, 5 required continuous bladder irrigation. The presence of hematuria did not effect OS. Thirteen patients (17.81%) had some kind of obstructive uropathy, and their management is also reflected in Table 2. A bilateral ureterohidronephrosis (BUHN) (n = 2) worsened OS, compared with all other complications: no obstruction (n = 60) (HR = 0.12, 95% CI 0.03–0.57, p = 0.008), unilateral ureterohidronephrosis (UUHN) (n = 4) (HR = 0.09, 95% CI 0.01–0.62, p = 0.015) and bladder outlet obstruction (BOO) (n = 7) (HR = 0.04, 95% CI 0.01–0.32, p = 0.002) [Figure 4(b)]. Those findings could be related with the high proportion of patients that did not receive local treatment for their prostate cancer (42.47%) in our series.
Discussion
Since Huggins demonstrated the responsiveness of prostate cancer cells to ADT, this therapeutic strategy has had an undeniable key role in the treatment of patients with metastatic PC. However, ADT causes a decrease in testosterone levels, leading changes in body composition that include an increase in insulin levels leading an insulin resistance syndrome. 23 Insulin resistance is one of the entities involved in the MD along with HTN, hypercholesterolemia, and weight gain. This situation may explain why more than half of the patients with PC treated with ADT for at least 6 months are reported to suffer from MD.20,21 This high prevalence has led several researchers to focus on this entity, finding that patients with PC and MS have poorer survival.15,34–36
Particularly in our study, we have made an exploratory analysis of several endocrine, cardiovascular, clinical, and urologic comorbidities to assess whether they could have an effect on our patients’ survival in the first line mCRPC setting. In this sense, and according to our findings, not only is MD a predictor of worse survival, but evaluation of DM must be taken into account for this purpose. Whether patients with DM treated with OAD who progress to INS have a poorer survival outcome is still unknown. Other previous comorbidities were also related to a worse survival, such as HTN and stroke.
Concerning CVE (defined as de novo HTN, de novo arrhythmia, an episode of IHD, an episode of HF, and stroke), we recorded a higher incidence (34.25%) than that reported in other studies, which may be due to the population included coming from routine clinical practice. 13 However, no relevant differences in survival were identified between most groups. Interestingly, patients with an elevation in their blood pressure levels (either from having de novo HTN or worsening of a previous HTN) have better prognosis in terms of OS than the rest of the patients. These findings result of special interest and suggest a potential predictive value of the worsening of HTN in patients treated with API in this setting. However, an exploratory study has been made in this dataset that must be confirmed in a larger population.
The main limitations of our study are the small sample size and the retrospective design. Despite this, we would like to emphasize that we have selected a homogeneous population, being, to the best of our knowledge, the first study to evaluate a cohort of patients with mCRPC treated with AA or enzalutamide exclusively in the first line setting. In larger studies evaluating the role of MD in mCRPC, all patients had received some type of previous therapy, among which docetaxel was administered in 80.5–100% of patients.13,14
Although we cannot make direct comparisons, the use of previous therapies, especially docetaxel, may increase the incidence of MD in patients with mCRPC. In fact, although Conteduca et al. 14 did not find a different incidence of MD among the different number of previous therapies in mCRPC, they identified that MD was associated with greater frequency in those patients treated with docetaxel (95.5% versus 77.9%, p = 0.0003). They suggested that it could be related to a longer exposure time to a greater number of risk factors (i.e., age, corticoids, advanced disease).
However, we have not found a higher incidence of DM, HTN, or hypercholesterolemia in patients treated with AA over enzalutamide in our study. These findings could be explained by the low number of events in both treatment groups. Longer follow up is needed to confirm these findings.
Regarding statin use, we did not identify any survival effect on its use in this setting in accordance with other authors findings. 37 However, other studies have observed a trend toward a longer duration of treatment with AA, 37 a delay in the progression to CRPC in the metastatic setting, 38 and a longer OS.26,39 These differences could be explained by the heterogeneity between the different patient populations included in the analysis.
In addition, we have also observed that patients who have had a worsening in their pain control and end up needing the use of major opioids, have a poorer survival than those who do not need any adjustment. This fact could be related to a disease progression due to the lack of response to oncological treatment, rather than to be related with those therapies themselves.
Finally, to the best of our knowledge, our study is also the first to evaluate whether the presence of some urological complications (hematuria and obstructive uropathy) could have a deleterious effect in mCRPC patients treated with API. The appearance of hematuria does not adversely affect OS; however, the development of BUHN provides worse survival. The presence of BOO seems to have no effect on OS.
Despite this, these outcomes may be related with a more aggressive disease as well as other prognostic factors as suggested by Armstrong AJ and col. that may help to individualize treatment approaches in this cohort of patients. 31
In addition, our study has evaluated whether some clinical and metabolic conditions could have an effect on survival outcomes, and, according to our findings, this fact seems to be highly probable, especially with HTN and DM. In this sense, it may be critical to include in the management of patients from our daily clinical practice treated with API in the first line setting of mCRPC, the promotion of a change in healthy life habits and, specifically, perform a strict control of glycemic levels, cholesterol, and cardiological assessment, in addition to routine cancer pain and urinary symptoms monitoring. Considering the increasingly high exposure of patients to oncological active treatments, including metastatic hormone sensitive PC or nonmetastatic CRPC settings, the ability to offer a comprehensive and global assessment to the patient, as well as, introducing adequate preventive measures may, in the end, have a benefit in terms of survival and quality of life for patients with PC.
However, we need prospective studies to assess the real effect of these comorbidities and the effectiveness of these proposals, including changes in lifestyle, such as physical exercise and healthy diet.
Conclusion
Although the interactions between different clinical and metabolic characteristics can be complex, we have observed that some comorbidities may be involved in patients’ outcomes when receiving AA or enzalutamide for mCRPC. Unfortunately, these patients were excluded from the randomized trials that motivated the approval of the drugs for general use for patients with mCRPC. In this sense, real life studies are relevant to provide more information about the different prognostic effect of several medical and urological complications. In this analysis, patients with previous DM and insulin needs, HTN, and stroke had a worse survival. During treatment, the presence of heart failure, a requirement of major opioids, and BUHN, was related to poorer prognosis. Overall, the information obtained in this analysis may suggest that a collaborative network between specialists and caregivers treating PC patients might be helpful in order to anticipate the medical and surgical complications that may worse patients’ survival.
Supplemental Material
sj-docx-1-tau-10.1177_17562872211043341 – Supplemental material for The effect of medical and urologic disorders on the survival of patients with metastatic castration resistant prostate cancer treated with abiraterone or enzalutamide
Supplemental material, sj-docx-1-tau-10.1177_17562872211043341 for The effect of medical and urologic disorders on the survival of patients with metastatic castration resistant prostate cancer treated with abiraterone or enzalutamide by Juan José Serrano Domingo, Teresa Alonso Gordoa, Javier Lorca Álvaro, Javier Molina-Cerrillo, Arantzazu Barquín García, Olga Martínez Sáez, Javier Burgos Revilla, Alfredo Carrato and Sara Álvarez Rodríguez in Therapeutic Advances in Urology
Footnotes
Acknowledgements
The authors wish to thank the patients who participated in the study mentioned and their families.
Author contributions
Conceptualization/Design: Juan José Serrano, Javier Molina-Cerrillo, Teresa Alonso Gordoa; Methodology: Javier Lorca, Arantzazu Barquin; Validation: Teresa Alonso Gordoa, Javier Molina-Cerrillo, Afredo Carrato, Javier Burgos; Formal analysis and investigation: Juan José Serrano, Teresa Alonso Gordoa, Alfredo Carrato, Sara Álvarez; Resources: Arantzazu Barquin, Olga Martínez; Data Curation: Teresa Alonso Gordoa; Writing: Juan José Serrano, Sara Álvarez, Javier Lorca, Teresa Alonso Gordoa; Supervision; Alfredo Carrato; Javier Burgos, Teresa Alonso Gordoa, Javier Molina-Cerrillo.
Conflict of interest statement
Juanjo Serrano Domingo declares Travel expenses from Janssen.
Teresa Alonso Gordoa declares Advisory Boards: Bayer, Janssen, Sanofi, Astellas; Speaker: Janssen, Astellas; Travel expenses: Sanofi
Javier Lorca Álvaro declares Travel expenses from Astellas.
Arantza Barquín García declares no conflicts of interest
Javier Molina Cerrillo declares Advisory Boards: Sanofi; Speaker: Janssen.
Olga Martínez Sáez declares no conflicts of interest.
Javier Burgos Revilla declares Advisory Boards and Honoraria from Astellas, Janssen and Sanofi and Travel Grants from Astellas and Janssen.
Alfredo Carrato declares Advisory Boards: Bayer.
Sara Álvarez Rodriguez has received honoraria from Janssen, Astellas and Bayer.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.