
Abstract
Background:
The purpose of this study was to investigate the relationship between marital status and the prognosis of patients with upper tract urothelial carcinoma (UTUC) treated with nephroureterectomy (NU).
Methods:
Patients with UTUC who received NU treatment were identified from the Surveillance, Epidemiology, and End Results (SEER) database between 2004 and 2015. Kaplan–Meier curves and Cox regression were used to analyze the effect of marital status on cancer-specific survival (CSS), and 1:1 propensity score matching (PSM) was performed for married and unmarried patients to explore further the effect of marital status on patients with UTUC.
Results:
Among 1565 eligible patients, 960 (61.3%) were married and 605 (38.7%) were unmarried, of which 146 (9.3%) were divorced/separated, 306 (19.6%) were widowed, and 153 (9.8%) were single. Multivariate Cox regression analysis showed that marital status was not an independent risk factor for patients with UTUC treated with NU. After stratification by grade and SEER stage, multivariate analysis showed that there was no significant difference in 5-year CSS between divorced/separated, widowed, and single patients compared with married patients in different grades and SEER stages. In addition, after PSM analysis, marital status was still not an independent risk factor for patients with UTUC treated with NU.
Conclusion:
For patients with UTUC treated with NU, marital status has no prognostic effect on CSS.
Keywords
Background
Upper tract urothelial carcinoma (UTUC) refers to urothelial malignant tumors that occur in the renal pelvis, calyceal system, and the entire segment of the ureter, including renal pelvis cancer and ureteral carcinoma, which accounts for about 5–10% of urothelial cancer.1,2 Compared with bladder cancer, at the time of onset, more patients with a combination of bladder cancer at the time of onset have a worse prognosis. 3 UTUC has the characteristics of multicentric tumor growth and urinary dissemination tendency, and the tumor recurrence rate of residual renal pelvis or ureteral tissue after simple lesions and partial urethral resection was relatively high. 4 The current gold standard for high-risk UTUC is radical nephroureterectomy (NU) plus bladder sleeve resection, but there are still 20–30% of patients with extra-urinary tract recurrence after operation. 5
Marital status has always been closely related to cancer mortality. Many studies have confirmed that marital status may affect the prognosis of a variety of tumors, including bladder cancer, 6 prostate cancer, 7 penile cancer, 8 as well as colorectal carcinoma, 9 and married patients were considered to have a better survival prognosis. Previous studies have found that marital status was an independent risk factor for UTUC, 10 but no study has reported the effect of marital status on the survival of patients with UTUC treated with NU. Therefore, the purpose of this study was to explore whether marital status has an impact on the survival of patients with UTUC treated with NU through the data extracted from the Surveillance, Epidemiology, and End Results (SEER) database.
Methods
Patient selection
The data presented in our study were retrieved from the SEER database, which is funded by the US National Cancer Institute. The SEER database covers approximately 28% of the US population and includes demographic information and cancer characteristics, such as age at diagnosis, year of diagnosis, race, marital status, insurance status, income status, primary tumor location, tumor grade and stage, histological type, tumor-node-metastasis stage, treatment modality, and survival time. 11 The National Cancer Institute’s SEER × Stat software [version 8.3.5; SEER 18 Regs Custom Data (with additional treatment fields), November 2018 Sub (1975–2016 varying) database] was used in this study. Using the ‘primary site-labeled’ variable codes C65.9 − Renal pelvis and C66.9 − Ureter, we identified 15,119 patients between 1 January 2010 and 31 December 2015.
Exclusion criteria in our study were as follows: (a) marital status unknown or domestic partner (n = 723); (b) patients under 18 years of age (n = 2); (c) unknown survival time (n = 30); (d) not one primary tumor only (n = 7185); (e) surgery code not 50, 70, 80 (n = 5510); (f) histology type not transitional cell carcinoma (n = 104). Finally, we left 1565 eligible patients diagnosed with UTUC.
Study variables
Variable definition information about age at diagnosis, year of diagnosis, sex, race, marital status, histological type, tumor grade, SEER stage, radiotherapy, chemotherapy, median household income, and survival time can be found in the SEER database. The starting point for the follow up was the date of diagnosis of UTUC, and the endpoint was cancer-specific death or the last follow up in December 2015. When analyzing cancer-specific survival (CSS), mortality cases associated with other causes were excluded.
Statistical analysis
Age and household income (Figure S1) were categorically divided based on the optimal cut-off value generated by X-tile software (Version 3.6.1). Chi-square analysis was performed to evaluate clinical characteristics of patients with UTUC treated with NU. Kaplan–Meier curves were used to estimate the CSS of patients with UTUC treated with NU, and the differences between the curves were analyzed by log-rank test. Univariate and multivariate Cox regression models were performed to estimate the hazard ratios and 95% confidence intervals to analyze independent prognostic factors of patients with UTUC treated with NU.
Patients were divided into a married group and an unmarried group according to marital status. The 1:1 propensity score matching (PSM) reduced the selection bias of two groups of baseline variables, including year of diagnosis, age at diagnosis, sex, race, primary site, grade, SEER stage, radiotherapy, chemotherapy, and household income (Figure S2). After PSM, the impact of marital status on the entire cohort and different grades and SEER stages were re-evaluated. The Statistical Package for the Social Sciences software (version 24.0; SPSS, Chicago, IL, USA) and R software (version 3.5.1, http://www.r-project.org/) were used for all statistical analyses. p value < 0.05 (two-sided) was considered statistically significant.
Results
Demographic and clinicopathologic characteristics
According to the screening criteria in Figure 1, a total of 1565 eligible patients with UTUC treated with NU were included in our study cohort from 2004 to 2015, of which 960 (61.3%) were married, 146 (9.3%) were divorced/separated, 306 (19.6%) were widowed, and 153 (9.8%) were single. Table 1 shows the demographic and clinical characteristics of patients with UTUC treated with NU. In the whole cohort, 1250 (79.9%) were patients with renal pelvis cancer and 315 (20.1%) with ureter cancer. The majority of patients were men (56.2%), ⩽76 years (64.9%), grade IV (48.9%), regional (63.1%), and no radiotherapy (92.8%) or chemotherapy (72.8%). In addition, chi-square tests showed differences in sex, age, race, and chemotherapy between married and unmarried groups or between married, divorced/separated, widowed, and single groups. The proportion of women (77.1% versus 33.5%, 43.8%, 41.8%), >76 years (65.7% versus 29.6%, 24.7%, 19.0%), did not receive chemotherapy (84.6% versus 69.1%, 75.3%, 69.9%) in the widowed group was higher than in other groups.
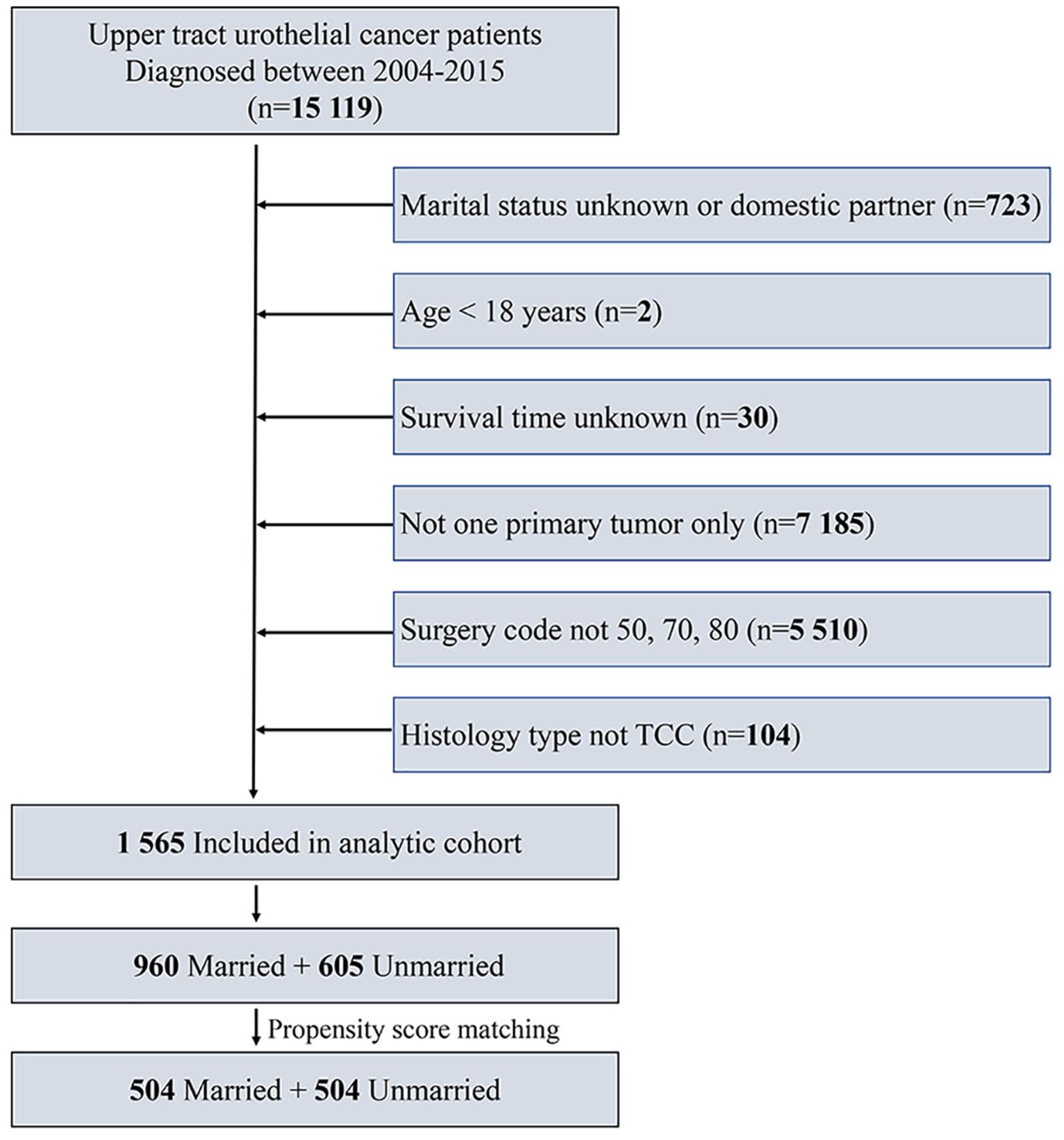
Schematic flow diagram of inclusion and exclusion criteria for the study cohort.
Baseline demographic and clinical characteristics of upper tract urothelial carcinoma patients in our study.

Percentages may not total 100 because of rounding.
Chi-square detected the difference between the married group and unmarried group.
Chi-square detected the difference between the married group, divorced/separated group, widowed group, and single group.
Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated.
SEER, Surveillance, Epidemiology, and End Results.
Identification of prognostic factors of CSS before PSM
Univariate and multivariate Cox regression were used to analyze the factors associated with CSS of patients with UTUC treated with NU (Table 2). Univariate and multivariate Cox regression analyses showed that age, primary site, grade, SEER stage, radiotherapy, and chemotherapy were related factors (all p < 0.05) of CSS in patients with UTUC treated with NU, while marital status was not an independent risk factor for CSS (Figure 2).
Univariate and multivariate analysis of CSS rates before propensity score matching.
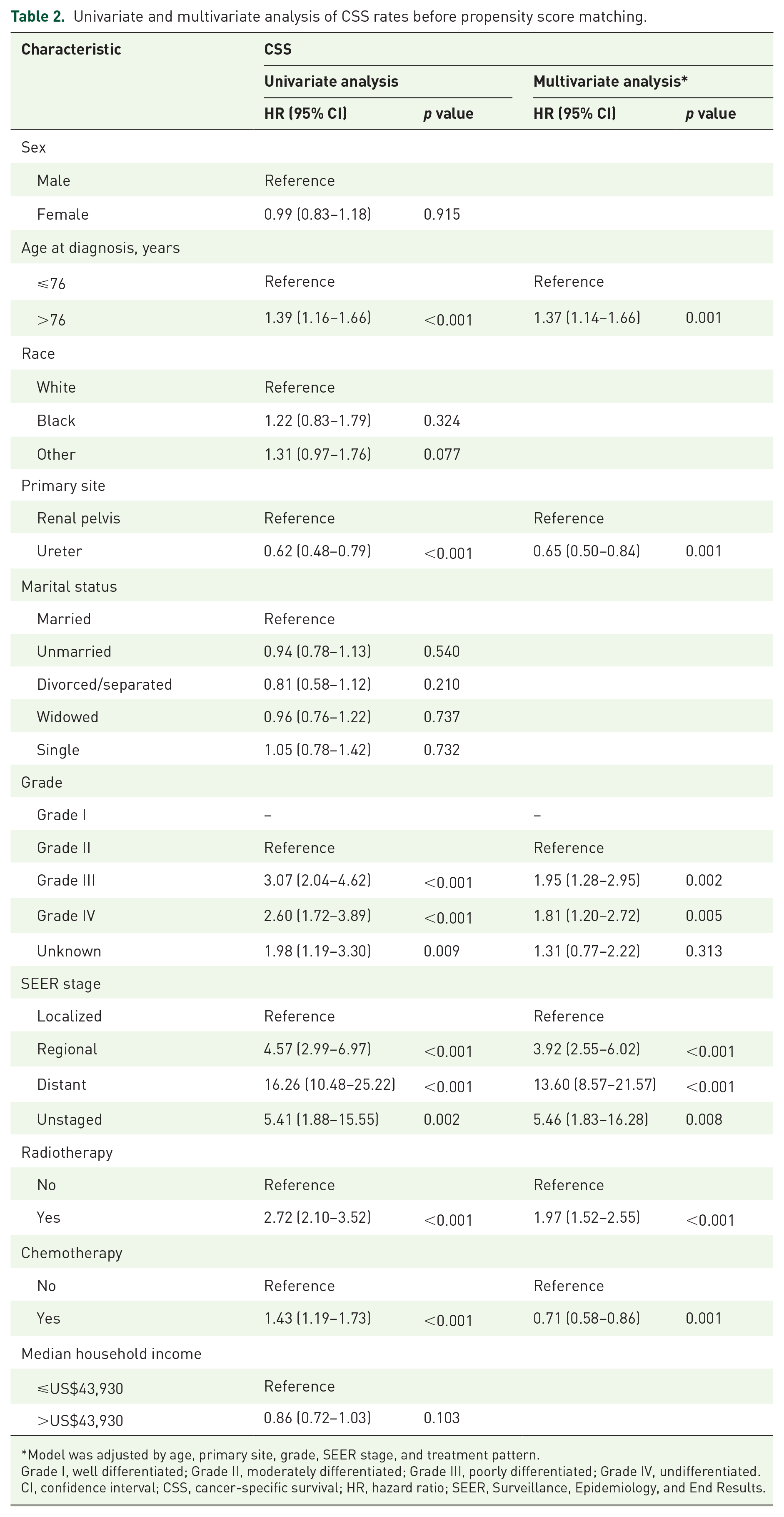
Model was adjusted by age, primary site, grade, SEER stage, and treatment pattern.
Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated.
CI, confidence interval; CSS, cancer-specific survival; HR, hazard ratio; SEER, Surveillance, Epidemiology, and End Results.

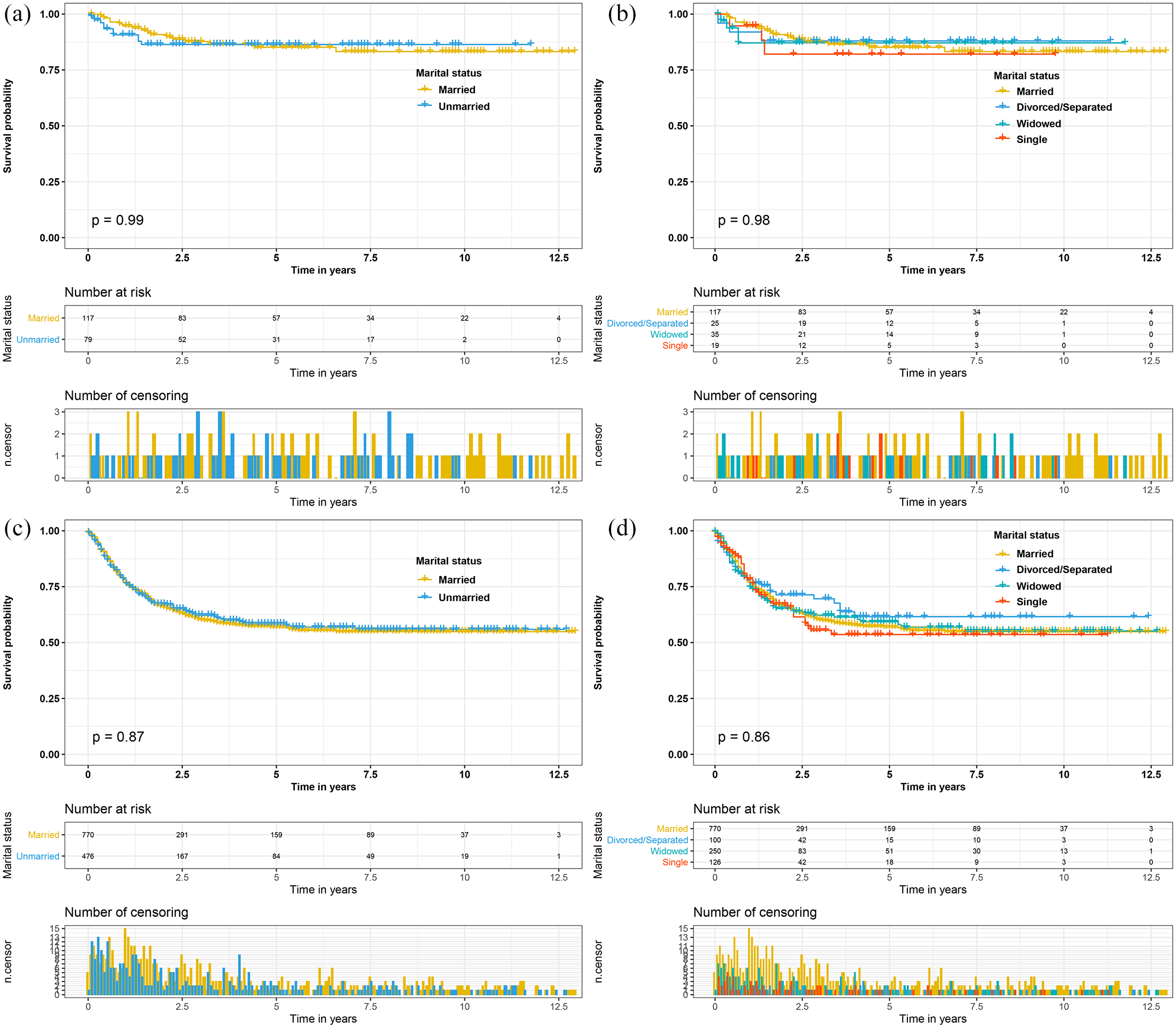
(a)and (b) Cancer-specific survival curves according to marital status in patients with upper tract urothelial carcinoma treated with nephroureterectomy before propensity score matching.
Subsequently, after stratification by grade and SEER stages, univariate analysis showed that marital status was not related to CSS of the different grades and SEER stages (Figures 3 and S3). Multivariate analysis showed that there was no significant difference in 5-year CSS between married and unmarried or divorced/separated, widowed, and single patients; marital status was not an independent risk factor for CSS in patients in the different grades and SEER stages (Table 3).
Cancer-specific survival curves of patients with upper tract urothelial carcinoma treated with nephroureterectomy according to marital status in different grades before propensity score matching. (a) and (b) Cancer-specific survival times in grade I/II patients. (c) and (d) Cancer-specific survival times in grade III/IV patients.
Multivariate analysis of CSS rates based on primary site before propensity score matching.

Model was adjusted by age, primary site, grade, SEER stage, and treatment pattern.
CI, confidence interval; CSS, cancer-specific survival; HR, hazard ratio; SEER, SEER, Surveillance, Epidemiology, and End Results.
Identification of prognostic factors of CSS after PSM
After year of diagnosis, age at diagnosis, sex, race, primary site, grade, SEER stage, radiotherapy, chemotherapy, and household income at 1:1 PSM, we screened 504 married patients and 504 unmarried patients. We performed univariate and multivariate Cox regression analyses on all patients, and found that age, primary site, grade, SEER stage, radiotherapy, chemotherapy, and household income were independent risk factors (Table 4), while marital status was not an independent risk factor for CSS in all patients (Figure 4). After stratification by grade and SEER stage, multivariate analysis showed that there was no significant difference in 5-year CSS between married and unmarried or divorced/separated, widowed, and single patients (Table 5); marital status was not an independent risk factor for the different grades and SEER stages in patient CSS (Figures 5 and S4).
Univariate and multivariate analyses of CSS rates after the 1:1 propensity score matching sample.

Model was adjusted by age, primary site, grade, SEER stage, treatment pattern, and household income.
Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated.
CI, confidence interval; CSS, cancer-specific survival; HR, hazard ratio; SEER, Surveillance, Epidemiology, and End Results.

(a) and (b) Cancer-specific survival curves according to marital status in patients with upper tract urothelial carcinoma treated with nephroureterectomy after propensity score matching.
Multivariate analysis of CSS rates based on primary site in the 1:1 propensity score matching sample.

Model was adjusted by age, primary site, grade, SEER stage, treatment pattern, and household income.
Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated.
CI, confidence interval; CSS, cancer-specific survival; HR, hazard ratio; SEER, Surveillance, Epidemiology, and End Results.

Cancer-specific survival curves of patients with upper tract urothelial carcinoma treated with nephroureterectomy according to marital status in different grades after propensity score matching. (a) and (b) Cancer-specific survival times in grade I/II patients. (c) and (d) Cancer-specific survival times in grade III/IV patients.
Discussion
In this 12-year retrospective study, we conducted a multivariate Cox regression analysis of a large number of patients with UTUC who received NU treatment through the SEER database, and found that marital status was not an independent risk factor for CSS. After stratifying by grade and SEER stage, multivariate analysis showed that there was no significant difference in 5-year CSS between married and unmarried or divorced/separated, widowed, and single patients. In addition, marital status was still not an independent risk factor for patients with UTUC treated with NU after PSM.
Marital status was widely regarded as an independent prognostic factor for many tumors.12–15 However, the impact of marital status on the outcome of surgical patients was still a controversial topic. Wu et al. 16 investigated 13,408 patients with hepatocellular carcinoma (HCC) who underwent surgical resection and found that marital status was an independent risk factor, and widowed patients had the highest risk of death. Roubion et al. 17 investigated the relationship between marital status and prognosis of 422 patients undergoing total knee arthroplasty, and found that the overall prognosis of married patients after total knee arthroplasty was better. Wang et al. 18 collected data from 10,852 patients with UTUC from the SEER database between 1988 and 2015 and found that marital status was a predictor of overall survival and CSS in patients with UTUC, and widowed patients had the worst overall survival and CSS. These studies showed that married patients have higher survival rates than unmarried patients.
In contrast, a few studies have shown that marital status does not affect the survival outcomes of surgical patients. Gatchel et al. 19 found no significant correlation between marital status and surgical outcome in a study of 1679 patients with consecutive chronically disabled work-related spinal disorders. Sorensen et al. 20 conducted a prospective study of 57 patients who underwent surgery for slipped lumbar disc and did not find that marital status could be used as an indicator of postoperative prognosis. Reyngold et al. 21 found that there was no association between marital status and overall survival or disease-free survival in patients with pancreatic cancer who received adjuvant postoperative chemotherapy followed by external radiotherapy and chemotherapy. In addition, Yan et al. 22 found that marital status had no prognostic effect on survival based on the analysis of 1581 patients with less differentiated HCC who underwent surgery between 2004 and 2015. Similar to the above studies, we found that marital status had no significant effect on the prognosis of patients with UTUC treated with NU.
In addition, we also made an interesting discovery: nearly half (48.9%) of the patients included in this study were at grade IV stage. Unlike the study by Wang et al., 18 we found that marital status is not a prognostic factor for patients with UTUC treated with NU, which may be due to the fact that most patients had a higher stage, poor prognosis, and short survival course.
Despite these conflicting views about the effects of marital status on surgical outcomes, variables in each study should be considered. As most of these studies included heterogeneous cohort study, it is not possible to evaluate properly the usefulness of marital status for the prognosis. Therefore, further prospective studies are needed to investigate the effect of marital status on the prognosis of patients with UTUC treated with NU.
There are limitations to be recognized in this study. First, this study was a retrospective study with obvious limitations. Second, there are no data on parenthood in the SEER database, and having supportive children might be a stronger predictor for longevity. Moreover, the specific content of surgery and other adjuvant therapy (e.g. radiotherapy, chemotherapy, immunotherapy, etc.) was not included, which are also prognostic factors for patients with UTUC.
Conclusion
Our study found that marital status had no prognostic effect on CSS for patients with UTUC treated with NU. After stratification and PSM of the primary site, marital status was still not an independent prognosis factor.
Supplemental Material
sj-tif-1-tau-10.1177_1756287220981510 – Supplemental material for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study
Supplemental material, sj-tif-1-tau-10.1177_1756287220981510 for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study by Weipu Mao, Jianping Wu, Keyi Wang, Bin Xu and Ming Chen in Therapeutic Advances in Urology
Supplemental Material
sj-tif-2-tau-10.1177_1756287220981510 – Supplemental material for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study
Supplemental material, sj-tif-2-tau-10.1177_1756287220981510 for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study by Weipu Mao, Jianping Wu, Keyi Wang, Bin Xu and Ming Chen in Therapeutic Advances in Urology
Supplemental Material
sj-tif-3-tau-10.1177_1756287220981510 – Supplemental material for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study
Supplemental material, sj-tif-3-tau-10.1177_1756287220981510 for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study by Weipu Mao, Jianping Wu, Keyi Wang, Bin Xu and Ming Chen in Therapeutic Advances in Urology
Supplemental Material
sj-tif-4-tau-10.1177_1756287220981510 – Supplemental material for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study
Supplemental material, sj-tif-4-tau-10.1177_1756287220981510 for Marital status does not affect the cancer-specific survival of patients with upper tract urothelial carcinoma treated with nephroureterectomy: a propensity score matching study by Weipu Mao, Jianping Wu, Keyi Wang, Bin Xu and Ming Chen in Therapeutic Advances in Urology
Footnotes
Acknowledgements
We acknowledge the efforts of the SEER Program tumor registries in the creation of the SEER database.
Authors’ contributions
WM, BX, and MC studied the concept and design. WM and JW collected the data. WM and KW analyzed and interpreted the data, and drafted the manuscript. BX, JW, and MC critically revised the manuscript for important intellectual content. WM and MC performed the statistical analysis.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 81572517), the Natural Science Foundation of Jiangsu Province (BK20161434), Jiangsu Provincial Medical Innovation Team (CXTDA2017025), national key research and development projects (SQ2017YFSF090096), and Jiangsu Provincial Medical Talent (ZDRCA2016080).
Ethical approval
Cancer is a reportable disease in every state of the USA. The data in the SEER database do not require informed patient consent. The present study complied with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study used previously collected de-identified data, which was deemed exempt from review by the Ethics Committee of the Affiliated Zhongda Hospital of Southeast University and does not require informed patient consent.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.