
Abstract
Introduction:
Lower urinary tract symptoms (LUTS) caused by prostatic enlargement are a common impairing condition in men aged 50 years and older. In the management of LUTS related to benign prostatic hyperplasia (BPH), medication, particularly by α-adrenoceptor antagonists, 5α-reductase inhibitors, and phytopharmaceuticals, is considered the first-line therapy. Despite their popularity, a number of adverse effects on the cardiovascular or cognitive systems have been reported for some of the synthetic drugs. One of the promising herbal preparations for the treatment of patients suffering from LUTS related to BPH is WS PRO 160 I 120 mg, a combination of sabal fruit extract and urtica root extract.
Methods:
This review of the literature summarizes clinical evidence for WS PRO 160 I 120 mg derived from four randomized placebo- or reference-controlled double-blind clinical trials including men aged 50 years and older. In all trials, symptomatic improvement was evaluated by the International Prostate Symptom Score (I-PSS) total score.
Results:
Treatment effects of WS PRO 160 I 120 mg were shown to be superior over placebo and comparable with the 5α-reductase inhibitor finasteride or the α1-adrenoceptor antagonist tamsulosin with more favorable tolerability and safety profiles as compared with the reference drugs.
Conclusions:
The results suggest WS PRO 160 I 120 mg to be considered as a valid alternative in the treatment of patients with early BPH, especially with view to sexual function and a good quality of life, especially in long-term use.
Introduction
Lower urinary tract symptoms (LUTS) are very common in ageing men1–3 and associated with a reduced quality of life. 4 The estimated prevalence of LUTS related to benign prostatic hyperplasia (BPH) in men beyond the age of 50 is around 30% in all industrialized countries. 5 Prostatic enlargement can cause symptoms such as hesitancy, straining, weak stream, and intermittency (often referred to as obstructive symptoms) as well as frequency, nocturia, and urgency (often referred to as irritative symptoms). The latter symptoms, in particular, have been found to be most distressing for the patient. 6 The first and most frequently used treatment for BPH is medical therapy while surgical treatments are a second-line option in case medical therapy is not effective or associated with complications. 7 Drug treatment options in the management of BPH mainly comprise α-adrenoceptor antagonists, 5α-reductase inhibitors, and phytopharmaceuticals. Current recommendations of the American Uro-logic Association (AUA) suggest α-adrenoceptor antagonists as an efficacious therapy option in BPH medical therapy, 8 which is due to their superiority as compared with placebo. 9 Among the herbal drugs, extracts from the fruits of the American dwarf palm/saw palmetto plant (Sabal serrulata, syn. Serenoa repens) and the roots of stinging nettle (Urtica dioica) are particularly popular. 10
However, as phytotherapeutic agents are a heterogeneous group, the Guidelines Panel of the current guidelines of the European Association of Urology (EAU) 11 has not made any specific recommendations on phytotherapy for the treatment of LUTS. Therefore, there is a need to accumulate data and knowledge of individual phytopharmaceutical agents.
A promising herbal preparation is WS PRO 160 I 120 mg (WS® PRO 160 I 120 mg is the active ingredient of the product Prostagutt® forte, Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany), which has been investigated both in double-blind12–15 and in open 16 clinical trials in patients suffering from LUTS related to BPH. WS PRO 160 I 120 mg is a capsule, which contains 160 mg extract from saw palmetto fruits (10–14.3:1), with ethanol 90% (w/w) as the extraction solvent, and 120 mg dry extract from stinging nettle roots (7.6–12.5:1), with ethanol 60% (w/w) as the extraction solvent.
A combination of sabal fruit extract and urtica root extract promises to be effective in the treatment of LUTS due to BPH, as the drugs can be expected to show a synergistic effect 10 owing to their mechanisms of action. Saw palmetto extract was shown to inhibit 5α-reductase without exhibiting any androgen-binding activity,17,18 to potently and noncompetitively inhibit human α1-adrenoceptors in vitro, 19 and to selectively inhibit muscarinic receptors in the lower urinary tract.20,21 Stinging nettle root extract was shown to cause an inhibition of the membrane Na+,K+-ATPase activity of the prostate, which may limit prostate-cell metabolism and growth. 22 In addition, antiproliferative, antiphlogistic, and antiedematous effects were reported for both drugs.23,24
The aim of this narrative review was to summarize clinical evidence for WS PRO 160 I 120 mg (PRO 160/120) derived from randomized controlled double-blind clinical trials.
Methods
For this narrative review, randomized, double-blind, controlled clinical trials investigating the efficacy of PRO 160/120 in LUTS related to BPH were eligible. Control groups in eligible trials were allowed to be randomized to either placebo or a reference drug. A literature search was performed in the scientific data base PubMed in order to identify eligible trials. Search terms applied were ‘PRO 160/120’ and ‘double-blind’. In addition, the manufacturer was asked to provide relevant trials published.
Results
A total of four randomized, double-blind, controlled clinical trials investigating the efficacy and tolerability of PRO 160/120 were identified and included in our review.12–15 Characteristics of the four trials presented in the following are summarized in Table 1.
Overview on double-blind, randomized, controlled clinical trials with PRO 160/120 in LUTS related to BPH.

AUA, American Urologic Association; BPH, benign prostatic hyperplasia; CEDQ, Cologne Erectile Dysfunction Questionnaire; I-PSS, International Prostate Symptom Score; LUTS, lower urinary tract symptoms; QoL, quality of life.
Efficacy in randomized controlled trials
In all four randomized, double-blind, controlled clinical trials investigating the efficacy and tolerability of PRO 160/120, the relevant Ethics Committee or Institutional Review Board provided approval and patients aged 50 years or older were included. The most important outcome measure according to current guidelines used in these trials was the International Prostate Symptom Score (I-PSS) total score30,31 or its predecessor called the American Urologic Association Symptom Index (AUASI; also referred to as AUA Score A) for BPH. 32 At present, the I-PSS is the most commonly used tool to evaluate LUTS suggestive of benign prostatic obstruction. The I-PSS, which has a high level of psychometric validity and reliability, 33 uses the same seven questions as the AUASI but is additionally accompanied by a disease-specific quality of life question (‘bother question’). Both the I-PSS and the AUASI use a scale of 0 to 35, with mild symptoms scored 1 to 8, medium 9 to 18, and severe 19 to 35, and can be considered as identical (for reasons of simplification, both scores are referred to as I-PSS in the following).
Further outcome measures assessed in all four controlled clinical trials with PRO 160/120 were peak urine flow, mean urine flow, mean urine volume, flow increase time, micturition time, ultrasound residual volume, prostatic volume, and quality of life. In addition, adverse events and laboratory safety parameters were documented.
In order to eliminate placebo-responders, each trial had a single-blind placebo run-in phase. Patients whose peak urine flow rate changed by more than 3 ml/s during this phase were excluded.
Placebo-controlled studies
In the first randomized, double-blind, placebo-controlled study conducted with PRO 160/120, patients suffering from symptomatic hyperplasia stage I–II according to Alken, 34 with a peak urine flow <20 ml/s at a mean urine volume >150 ml were recruited in a specialized urological practice. 12 A total of 40 patients (PRO 160/120: 20; placebo: 20; age range 52–84 years) entered the double-blind treatment phase and were given one capsule PRO 160/120 or placebo twice daily for a treatment period of 24 weeks. The double-blind treatment phase was followed by a single-blind treatment phase during which all patients received one capsule PRO 160/120 twice daily for 24 weeks.
In the double-blind treatment phase, the mean I-PSS decreased from baseline values of 18.6 (CI 95% [15.0; 22.2]) points for the PRO 160/120 group and 19.0 (CI 95% [15.1; 22.9]) points for the placebo group to 11.1 (CI 95% [8.4; 13.7]) points and 17.6 (CI 95% [14.5; 20.7]) points at week 24, respectively (p = 0.002; two-sided U test). In a post-hoc evaluation of these results, which focused on I-PSS items assessing the so-called irritative symptoms, it could be shown that there was a statistically significant improvement in frequency and urgency under PRO 160/120 treatment throughout this treatment phase. 25 The time course of the I-PSS during the 48 weeks of treatment is shown in Figure 1(a).

Time course of the International Prostate Symptom Score (I-PSS total score) (a) and peak urine flow (b) during 48 week of treatment with PRO 160/120 versus placebo [n = 40, full analysis set (FAS); means and 95% confidence intervals; last observation carried forward]. Curves show treatment group assignment (PRO 160/120 versus placebo) during the double-blind phase. During the single-blind phase, all patients received PRO 160/120.
During the subsequent single-blind treatment phase, the I-PSS also decreased in those patients having been switched from placebo to PRO 160/120 treatment. However, at week 48, there still was an advantage in favor of those patients having received active medication throughout both phases of the trial (p = 0.009; two-sided U test).
The mean peak urine flow had also improved significantly by 3.3 (CI 95% [2.6; 4.0]) ml/s in the PRO 160/120 group compared with 0.6 (CI 95% [−0.4; 1.5]) ml/s in the placebo group after 24 weeks of therapy (p < 0.001; one-sided U test). While there was an increase in peak urine flow in all PRO 160/120 patients, this parameter was aggravated or unchanged in almost two-thirds of placebo patients. Responder rates (defined as the number of patients having an improvement in peak urine flow of at least 3 ml/s) were 75% for PRO 160/120 and 20% for placebo. During the single-blind treatment phase, peak urine flow also clearly increased in those patients having switched from placebo to active treatment. After 48 weeks, however, there still was an advantage in favor of those patients having received active medication throughout both phases of the trial (PRO 160/120: 4.6, CI 95% [3.7, 5.2], placebo: 2.3, CI 95% [1.1, 3.4]; p < 0.01, one-sided U test). The time course of the peak urine flow during the 48 weeks of treatment is shown in Figure 1(b).
For mean urine flow, mean urine volume, and the additionally assessed problems based on micturitional symptoms there was a statistically significant improvement in the PRO 160/120 group compared with placebo at the end of double-blind treatment. Moreover, at this time point, micturition time, flow increase time as well as ultrasound residual volume had markedly improved in the PRO 160/120 group compared with placebo. Patients’ quality of life, which was assessed by means of the AUA Score C, also showed significantly better results at the end of the double-blind treatment phase for those patients treated with PRO 160/120 compared to patients receiving placebo. Prostatic volume changed only marginally in both groups.
A second randomized, double-blind trial comparing PRO 160/120 with placebo was conducted by Lopatkin and colleagues 14 as a long-term multicenter trial in patients with LUTS (BPH Alken stage I–II, I-PSS total score ⩾14 points, IPSS Quality of Life ⩾4 points, peak urine flow <15 ml/s, and mean urine volume >100 ml).14,26 A total of 257 patients were randomized to a 24-week double-blind treatment (2 × 1 capsule/day PRO 160/120 versus placebo), which was followed by an open 24-week control phase (all patients receiving 2 × 1 capsule/day PRO 160/120) and by an open 48-week follow-up phase (all patients receiving 2 × 1 capsule PRO 160/120), which was evaluated and reported separately. 27
At baseline, the median I-PSS total score of those patients evaluable for efficacy (PRO 160/120: 127; placebo: 126) amounted to 18 points in each treatment group. After double-blind treatment, a statistically significant group difference in the decrease of the I-PSS was observed in favor of PRO 160/120 (PRO 160/120: –6 points; placebo: –4 points; p < 0.01, one-sided U test stratified by center). 14 At the end of the control phase, the I-PSS was reduced by another 2 points in the former placebo patients (now also treated with PRO 160/120) and by another 1 point in those patients having been treated with PRO 160/120 since the beginning of the double-blind treatment. This difference between the two treatment groups was also statistically significant (p = 0.01, one-sided stratified U test). 14 At the end of the control phase, the reduction in the median I-PSS was 7 points in both treatment groups compared with baseline, 26 which indicates that former placebo patients benefited from PRO 160/120 treatment to the same extent as did those patients having been treated with PRO 160/120 already since the beginning of the double-blind treatment phase.
After the control phase, 213 patients (PRO 160/120: 106; placebo: 107) entered the subsequent open-label extension of the trial (weeks 49–96). 27 For the patients without missing I-PSS baseline values (PRO 160/120: 106; placebo: 103), an additional median score reduction of 1 point was observed in each group, resulting in an overall median reduction of 9 points in both groups compared with baseline (Figure 2). This corresponds to an I-PSS total score reduction of 52.9% compared with baseline values. In the subset of patients with initially moderate or severe baseline LUTS, 45.2% and 88.5%, respectively, had improved at the end of the follow-up period, whereas only 6.4% and 11.5%, respectively, had aggravated to or continued to report severe symptoms.
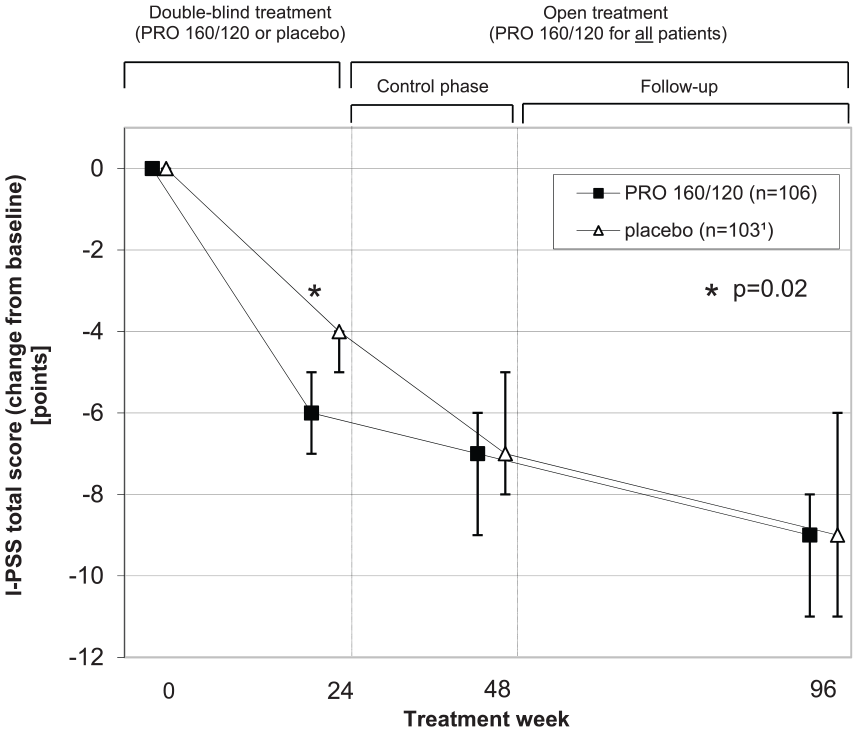
International Prostate Symptom Score (I-PSS total score): Change from baseline [n = 213, full analysis set (FAS) of patients included in the open-label extension of the trial; medians and 95% confidence intervals; one-sided U test p values; last observation carried forward]. Curves show treatment group assignment (PRO 160/120 versus placebo) during the double-blind phase. During the control phase and follow up, all patients received PRO 160/120.
Similar improvements were seen for both the irritative and obstructive symptoms subscores of the I-PSS.14,27 In a post-hoc analysis focusing on irritative symptoms, 35 a more pronounced improvement of nocturia was found for PRO 160/120 treated patients compared with placebo during the double-blind treatment (p = 0.07, one-sided U test, stratified by center). The rate of patients with improved nocturia was statistically significantly higher in the PRO 160/120 group compared with placebo (66.9% versus 54.8%; p = 0.047, two-sided χ2 test) and the improvement of urgency was statistically significant compared with placebo (p = 0.02, one-sided U test, stratified by center).
In a pooled analysis of the placebo-controlled trials concerning the effects on nocturia, nocturnal voids improved by 29% with PRO 160/120 compared with 18% with placebo (p = 0.015, one-sided Wilcoxon test). The responder rate was also significantly superior to placebo (69% versus 52%; p = 0.003, two-sided χ2 test), with the majority of responders improving by one void/night. Improvements were consistently higher with PRO 160/120 over a range of baseline severities. 36
Peak urine flow increased comparably in both groups (from baseline to week 24; PRO 160/120 versus placebo; p = 0.59, one-sided U test stratified by center) with the improvement rates being highest during the first weeks of the double-blind phase. During the control period, similar group differences were seen. For the remaining uroflow measures, changes were also comparable in both groups. Over the whole 96 weeks, data indicated a systematic, moderate improvement in mean urine flow (+18.9% percentage change in mean; p < 0.001, one-sided Wilcoxon signed rank test), a reduction in prostatic volume (−6.7%; p = 0.001) and a decrease in ultrasound residual volume (−43.8%; p = 0.03). All other uroflow measures had slightly improved (micturition time, flow increase time) or remained almost unchanged (mean urine volume).
Reference-controlled studies
A reference-controlled trial comparing the efficacy and tolerability of PRO 160/120 versus the 5α-reductase inhibitor finasteride was carried out by Sökeland and Albrecht. 13 In this randomized, double-blind noninferiority trial, a total of 543 men (aged 50–88 years) with early BPH (Alken stage I–II, peak urine flow <20 ml/s, mean urine volume >150 ml) were recruited from 81 medical practices. After the placebo run-in phase, 516 patients were randomized to a double-blind 48 weeks treatment and given either two PRO 160/120 capsules and one placebo capsule or one finasteride (5 mg) capsule and two placebo capsules daily. The study objective was to demonstrate therapeutic equivalence between PRO 160/120 and finasteride.
At the end of the trial, the symptomatology of patients treated with PRO 160/120 had improved to a similar extent compared with patients treated with finasteride with a decrease in the I-PSS from 11.3 ± 6.5 points (PRO 160/120) and 11.8 ± 6.6 points (finasteride) at baseline to 8.2 ± 5.8 points (PRO 160/120) and 8.0 ± 5.7 points (finasteride) after 24 weeks and 6.5 ± 5.8 points (PRO 160/120) and 6.2 ± 5.2 points (finasteride) after 48 weeks (means ± SD) (Figure 3). The improvement in quality of life according to AUA Score C was also similar compared with finasteride. The increase in peak urine flow with PRO 160/120 (+1.9 ml/s) and finasteride (+2.4 ml/s) was shown to be therapeutically equivalent within an equivalence range of ±1.5 ml/s (p = 0.037; modified t test for shifted hypotheses). Mean urine flow and micturition time also improved with both treatments to a similar extent. There was an advantage in change of ultrasound residual volume in favor of finasteride, but correlation analysis showed that this had no relevant effects on peak urine volume or patients’ perceptible symptomatology. Mean urine volume did not show any relevant differences after treatment with either PRO 160/120 or finasteride.

Time course of the International Prostate Symptom Score (I-PSS total score), peak urine flow, and quality of life according to the American Urological Association (AUA) Score C during 48 weeks of treatment with PRO 160/120 versus finasteride (n = 516, full analysis set (FAS); means ± SD; last observation carried forward).
There was a somewhat greater change in mean prostatic volume for the 5α-reductase inhibitor throughout the trial (finasteride: 44.0–37.2 ml; PRO 160/120: 42.7–42.4 ml), but it was shown in subgroup analyses that both the efficacy of PRO 160/120 and finasteride were unrelated to prostatic volume. 28
Seven years after the end of this trial, Sökeland and Schläfke 29 contacted all trial centers that had participated in this clinical study in order to investigate the long-term effects of the treatment. Investigators were asked to contact the former study participants by mail and to provide them with a standardized questionnaire by which medication, I-PSS and quality of life should be assessed. A total of 184 (35.7%) study participants answered. Of these, 40.8% did not take any BPH medication, 16.3% took PRO 160/120 and 8.7% took finasteride at the time of questioning. According to the I-PSS, subjective symptoms had only worsened by 1.5–3 points under nearly all current therapies. This was especially observed in patients treated with PRO 160/120, tamsulosin, or finasteride at the time of the survey. I-PSS values were still markedly improved (by at least 2 points) compared with the baseline values of the study assessed nearly 8 years before (Figure 4). Patients who took PRO 160/120 at the time of the survey reported a slightly better quality of life than those taking tamsulosin (slightly worse) or other therapies (no change) compared with the end of the trial.

International Prostate Symptom Score (I-PSS total score): time course during 48 weeks of treatment with PRO 160/120 versus finasteride (n = 516) and until post-observation after 7 years (n = 184) (full analysis set (FAS); medians).
Another prospective, randomized, double-blind, multicenter trial was conducted in a double-dummy design in 23 private urological practices and out-patient clinics in order to compare the efficacy and tolerability of PRO 160/120 versus the α1-adrenoceptor antagonist tamsulosin. 15 A total of 140 patients suffering from LUTS caused by BPH (aged ⩾50 years, I-PSS total score ⩾13 points, IPSS Quality of Life ⩾3 points, peak urine flow rate ⩽12 ml/s, mean urine volume ⩾150 ml) were randomized after the placebo run-in phase to a 60-week treatment with 2 × 1 capsule PRO 160/120 (n = 71) or 1 × 1 capsule (0.4 mg) tamsulosin (n = 69) per day.
At the end of treatment, the I-PSS total score had improved from a baseline median of 20 points in each group by a median of 9 points in both groups. A total of 22 (32.4%) patients treated with PRO 160/120 and 19 (27.9%) patients treated with tamsulosin were responders (i.e. IPSS total score ⩽7 at end of treatment; n = 136 patients with any efficacy data after baseline; p = 0.034, test for noninferiority according to Farrington–Manning; noninferiority margin 10%). In a subgroup analysis by baseline I-PSS, PRO 160/120 and tamsulosin were comparably effective in patients with symptoms of moderate severity (initial I-PSS total score ⩽19 points; (Figure 5(a)) as well as in patients with severe symptoms (initial I-PSS total score ⩾20 points; Figure 5(b)). The patients’ quality of life improved by a median of 2 points in the PRO 160/120 group and 1 point in the tamsulosin group (baseline values: 3 points versus 4 points; medians).

International Prostate Symptom Score (I-PSS total score): Change during double-blind treatment, by baseline I-PSS [(a) baseline I-PSS ⩽19; (b) baseline I-PSS ⩾20; full analysis set (FAS); medians and 95% confidence intervals].
According to the Cologne Erectile Dysfunction Questionnaire (CEDQ), neither PRO 160/120 nor tamsulosin had any measurable effect on the patients’ sexual functioning. Regarding uroflowmetry and ultrasound measurement, both treatment groups showed considerable improvements regarding peak urine flow and mean urine flow. PRO 160/120 also decreased micturition time and ultrasound residual volume in a comparable manner to tamsulosin. There was no systematic effect observed for mean urine volume, flow increase time, and prostatic volume in either group.
Tolerability in randomized controlled trials
In all four randomized controlled trials published, the tolerability of PRO 160/120 was reported as very good. The administration of PRO 160/120 was not associated with a higher risk of adverse events than placebo.12,14 The combination of sabal and urtica extract also showed a good tolerability during the long-term administration and a high acceptance among the study participants, evidenced by a very low rate of premature withdrawals. 27 Compared with finasteride, fewer adverse events, especially fewer cases of diminished ejaculation volume, erectile dysfunction, joint pain, and headache, were reported. 13 Moreover, as compared with tamsulosin, adverse events were reported less often with one adverse event in 1514 treatment days for PRO 160/120 and one event in 1164 days for tamsulosin. 15
Discussion
In order to judge the efficacy of sabal preparations, properly randomized, controlled, and blinded trials with outcome measures using validated symptom-scale scores are postulated. 37 These requirements are fulfilled by all trials identified for this review of randomized controlled clinical trials investigating PRO 160/120 in LUTS related to BPH. In all of these trials, the I-PSS served as a main outcome measure. This tool is the most commonly used to evaluate LUTS suggestive to benign prostatic obstruction and has a high level of psychometric validity and reliability. 33 The I-PSS has been translated and validated in several languages and was shown to be sensitive to changes. Barry and colleagues 38 suggested a change of at least 3 points to be meaningful. As measured by this postulated relevant change, the improvements in the total I-PSS shown for PRO 160/120 treatment, which exceeded 3 points in all four randomized controlled trials,12–15 are to be considered of clinical relevance. Treatment with PRO 160/120 was shown to be comparably effective as the 5α-reductase inhibitor finasteride or the α1-adrenoceptor antagonist tamsulosin and clear advantages could be seen regarding the patient’s perception and subjective evaluation of LUTS as compared with placebo. This holds true not only for the total I-PSS but also for single ‘irritative’ symptoms. Nocturia, for example, which appears to be the most frequent urinary symptom, 39 as well as urgency, which was shown to be even more associated with perceived discomfort,6,39 have clearly improved as shown in re-evaluations of the respective placebo-controlled trials.25,35,36 Consequently, treatment with PRO 160/120 also leads to an improvement in patients’ quality of life.
The available data from randomized controlled trials are in line with earlier results derived from an open clinical study in BPH patients (Alken stage I–II), in which a clear improvement of the patients’ subjective condition as well as uroflowmetric parameters was observed 16 and indicate that treatment with PRO 160/120 provides a clinically relevant long-term benefit for the patients. Thus, the conclusion that PRO 160/120 slows down the natural progression of BPH, as drawn by Lopatkin and colleagues, 27 can be confirmed and encouraging evidence that PRO 160/120 is efficacious in this indication can be stated.
By presenting the results above, this review concisely accumulates published data of PRO 160/120 and shows that this herbal drug has already been investigated by means of a wide range of efficacy parameters. As outcome measures for efficacy assessment in this indication are manifold, further outcomes, such as the delay to surgery, may also be worth considering for future trials. Moreover, to present an even wider database, a systematic review and meta-analysis of randomized, double-blind clinical trials with this herbal preparation in LUTS/BPH would be worth thinking about as a next step.
The interest in phytotherapeutic agents is once again rising both in Europe and North America, not least because patients are dissatisfied with the adverse effects of the synthetic alternatives. 40 Therapy with alpha-blockers and 5α-reductase inhibitors, for example, can be associated with sexual adverse effects such as erectile dysfunction and ejaculatory disorders. 41 In general, there is a relatively high risk of vascular-related adverse events reported for most α-adrenoceptor antagonists. 9 Cardiovascular side-effects such as hypotension causing dizziness or syncope can be life-threatening, particularly in aged men who form the main group of LUTS/BPH patients requiring pharmaceutical therapy.42,43,44
Whereas α-adrenoceptor antagonists have been associated with vascular-related events, another group of standard synthetic BPH therapeutics, anticholinergics, are reported to pose an increased risk of promoting brain atrophy and subsequent dementing effects in aged patients. 45 Given the association of standard synthetic BPH therapeutics with possibly life-threatening or cognitively impairing adverse events in the major group of BPH/LUTS patients, the phytopharmaceutical therapeutic option PRO 160/120 should be recommended to this group of mainly elderly patients particularly in the long-term use as it is both safe and also of an effectiveness equal to popular synthetic drugs. Compared with finasteride or the α1-adrenoceptor antagonist tamsulosin, PRO 160/120 appears to be a therapeutically equivalent treatment option in LUTS, which, moreover, revealed a better safety profile than the 5α-reductase inhibitor.
As LUTS are often indicative of BPH, long-term effects of phytopharmacological therapy and the development of symptoms must closely be monitored. In case of perceived increasing impairment, a urodynamic examination to base the decision for surgery on findings of infra-vesical obstruction is indicated. In addition, intermediate administration of a synthetic agent effective in diminishing prostate volume as has been shown for the 5α-reductase inhibitor finasteride 13 may be considered in this case, given the patient’s readiness to cope with the known side-effects. However, taking into account the risk–benefit ratio of PRO 160/120 as compared to that of popular synthetic agents, the herbal preparation should in early stage BPH be the first-line option of treatment 28 as it allows for a safe long-term administration with improvement of BPH-related LUTS and for a better quality of life.
Conclusion
PRO 160/120 can be considered as a valid alternative in the treatment of patients with early BPH, especially considering cardiovascular aspects, sexual function, and a good quality of life. The drug appears to be as effective as finasteride or tamsulosin while showing a more favorable tolerability and safety profile, also in long-term use.
Footnotes
Acknowledgements
Dr. Willmar Schwabe GmbH & Co. KG kindly provided unpublished trial results to support this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany.
Conflict of interest statement
RKH was reimbursed for her scientific services for this review on a contractual basis by Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany. PF is a salaried employee of Dr. Willmar Schwabe GmbH & Co. KG, Karlsruhe, Germany. NL has no conflicts of interest to declare.
Ethical Statement
Being a review of the literature, this work did not require an ethical board approval.