
Abstract
The recently published phase II prospective SWITCH trial evaluated whether patients with metastatic castration-resistant prostate cancer (mCRPC) treated with abiraterone acetate could benefit from a ‘steroid switch’ from prednisone to dexamethasone. A total of 26 patients, both chemonaïve (14 patients) or pretreated with docetaxel (12 patients), with biochemical and/or limited radiological progression, were enrolled in this trial. Primary endpoint was prostate specific antigen (PSA) 30 defined as the proportion of patients with a PSA level decline 30% or more after 6 weeks of treatment with abiraterone acetate + dexamethasone. Secondary endpoints were: a PSA50 rate (defined as the proportion of patients with PSA decline of 50% or more after 12 weeks on abiraterone acetate + dexamethasone), biochemical and radiological progression-free survival (bPFS and rPFS, respectively), benefit from subsequent treatment and identification of biomarkers of response. Primary endpoint was reached in 46.2% of patients (12 patients), and two patients had an objective partial response on computed tomography scan. Median bPFS and rPFS were 5.3 months and 11.8 months. We present a case series of 11 patients who were consecutively treated with a steroid switch at our institution from January 2016 to August 2018 to investigate if this strategy could be used in a ‘real-life’ setting. We observed a PSA30 response in two patients (18%), median bPFS was 4.77 months (95% confidence interval [CI] 2.5–14.6) and median rPFS was 7.2 months (95% CI 3.8–15.5). Seven patients had a radiological stable disease as best response to steroid switch. Three patients were being still treated with abiraterone acetate + dexamethasone at data cut-off time. Our case series confirms that switching from prednisone to dexamethasone during abiraterone acetate treatment produces biochemical and radiological responses in both a predocetaxel and a postdocetaxel setting, providing a clinical benefit in mCRPC patients. However, to date, there is no clear indication as to which patient could benefit most from this kind of strategy.
Introduction
Recently Romero-Laorden and colleagues presented the results from the phase II prospective SWITCH trial, designed to confirm whether patients with metastatic castration-resistant prostate cancer (mCRPC) treated with abiraterone acetate would benefit from a ‘steroid switch’ from prednisone to dexamethasone. 1 Rationale for this trial came from a retrospective analysis of 30 patients with mCRPC treated with abiraterone acetate + dexamethasone after disease progression on abiraterone acetate + prednisone. In this study 30% or more of patients achieved a biochemical response with 30% or more lasting for a median of 20.6 weeks. 2 The SWITCH trial enrolled 26 patients, both chemonaïve (14 patients) or pretreated with docetaxel (12 patients), with biochemical and/or limited radiological progression defined as three or fewer new asymtomatic bone lesions, no new soft tissue lesions and less than a 40% increase in the size of target lesions defined by RECITST 1.1 criteria. Primary endpoint was prostate specific antigen (PSA) 30 defined as the proportion of patients with a PSA level decline of 30% or more after 6 weeks of treatment with abiraterone acetate + dexamethasone. Secondary endpoints were: a PSA50 rate (defined as the proportion of patients with a PSA decline of 50% or more after 12 weeks on abiraterone acetate + dexamethasone), biochemical and radiological progression-free survival (bPFS and rPFS, respectively), benefit from subsequent treatment and identification of biomarkers of response. Primary endpoint was reached in 46.2% of patients (12 patients), PSA50 was observed in 34.6% (8 patients) and 2 patients had an objective partial response on computed tomography (CT) scan. Median bPFS and rPFS were 5.3 months and 11.8 months. Median overall survival (OS) from the start of abiraterone acetate + dexamethasone was 20.9 months. Biological explanation of the antitumour activity of dexamethasone in combination with abiraterone is complex and not yet fully understood. Some evidence suggests a putative role for the androgen receptor (AR) mutated transcription by glucocorticoids or the role played by glucocorticoid receptor (GcR) amplification as a mechanism of treatment escape.3,4 Moreover, dexamethasone appears to be more effective than prednisone in mCRPC, 5 maybe as the result of a greater affinity for the GcR. 6
Case study
Based on these data we present a case series of 11 patients who were consecutively treated with a steroid switch at our institution from January 2016 to August 2018. The patients’ characteristics are shown in Table 1. Median age was 71 years, all patients had an Eastern Cooperative Oncology Group performance status of 0–1 and were asymptomatic. Five patients (45.4%) had bone metastasis, five had lymph node metastasis and one patient had both. Five patients received abiraterone acetate + prednisone after progression to docetaxel, while the other six patients were chemonaïve. Patients were treated with abiraterone acetate + prednisone for 17 cycles (median range 4–37). The switch from prednisone to dexamethasone was offered to patients with PSA progression and/or limited radiological progression (defined as no new lesions and less than 40% increase in the size of target lesions). All the patients were started on abiraterone acetate + dexamethasone after biochemical progression (defined by prostate cancer working group 2) and one patient also had a limited radiological progression. We retrospectively analysed our data to estimate if this strategy is able to provide some clinical benefits in a ‘real-life’ setting. We observed a PSA30 response in two patients (18%) but none experienced a PSA50. Median bPFS was 4.77 months (95% confidence interval [CI] 2.5–14.6) and median rPFS was 7.2 months (95% CI 3.8–15.5). Seven patients had a radiological stable disease as best response to a steroid switch. Median OS from the start of abiraterone acetate + dexamethasone was 14.1 months (95% CI 10.1–23.3). Three patients were still being treated with abiraterone acetate + dexamethasone at the time of data cut-off: two with a biochemical stable disease and one with stable disease on CT scan. Seven (87.5%) of the eight patients who progressed to abiraterone acetate + dexamethasone received further treatments: five patients (71.4%) received a taxane-based chemotherapy, one received enzalutamide and one received radium-223.
Characteristics of the patients at start of abiraterone acetate + dexamethasone treatment.

AA, abiraterone acetate; CRPC, castration-resistant prostate cancer; D, dexamethasone; P, prednisone; PSA, prostate-specific antigen.
Our case series, with the limits of a retrospective analysis and small sample size, confirmed that switching from prednisone to dexamethasone during abiraterone acetate treatment produces biochemical and radiological responses in both a predocetaxel and a postdocetaxel setting, providing a clinical benefit in patients with mCRPC.
The rates of PSA response were significantly lower than those from the SWITCH trial. However, as shown in Figure 1, five patients after 6 weeks and five patients after 12 weeks had a biochemical response thus confirming the antitumour activity of dexamethasone. bPFS was similar to that in the SWITCH trial (4.77 months versus 5.3 months, median), despite our patients having a worse rPFS (7.2 months versus 11.8 months) and OS (14.1 months versus 20.9 months). From our limited data there seems to be a specific subset of patients that responded better and thus benefited more from a steroid switch; we found a moderate positive correlation between long time to castration resistance, median duration of abiraterone acetate + dexamethasone and bPFS (r = 0.66, 95% CI 0.09–0.90; p = 0.029), even though there was no statistically significant correlation between entity of response to abiraterone acetate + prednisone and duration of bPFS on abiraterone acetate + dexamethasone (r = 0.56, 95% CI 0.08–0.92; p = 0.074). It is reasonable to assume that difference in activity and efficacy of a steroid switch is probably linked to different biomolecular characteristics of the tumour cell population among patients. The SWITCH trial evaluated several biomarkers, noteworthy are AR copy number and mutation status in plasma. AR gain and AR somatic puntiform mutation, such as T787A, have been described as mechanisms of primary and secondary resistance to abiraterone, respectively. 7 The SWITCH trial results are consistent with these findings: patients with AR normal had the best biochemical responses (PSA30 100% and PSA50 50%). AR gain led to no PSA response and a significantly shorter bPFS (2.8 months versus 8.3 months), and T878A mutation was associated with lower PSA response and worse bPFS. These molecular findings can probably explain the worse PSA response rates, rPFS and OS in our set of patients.
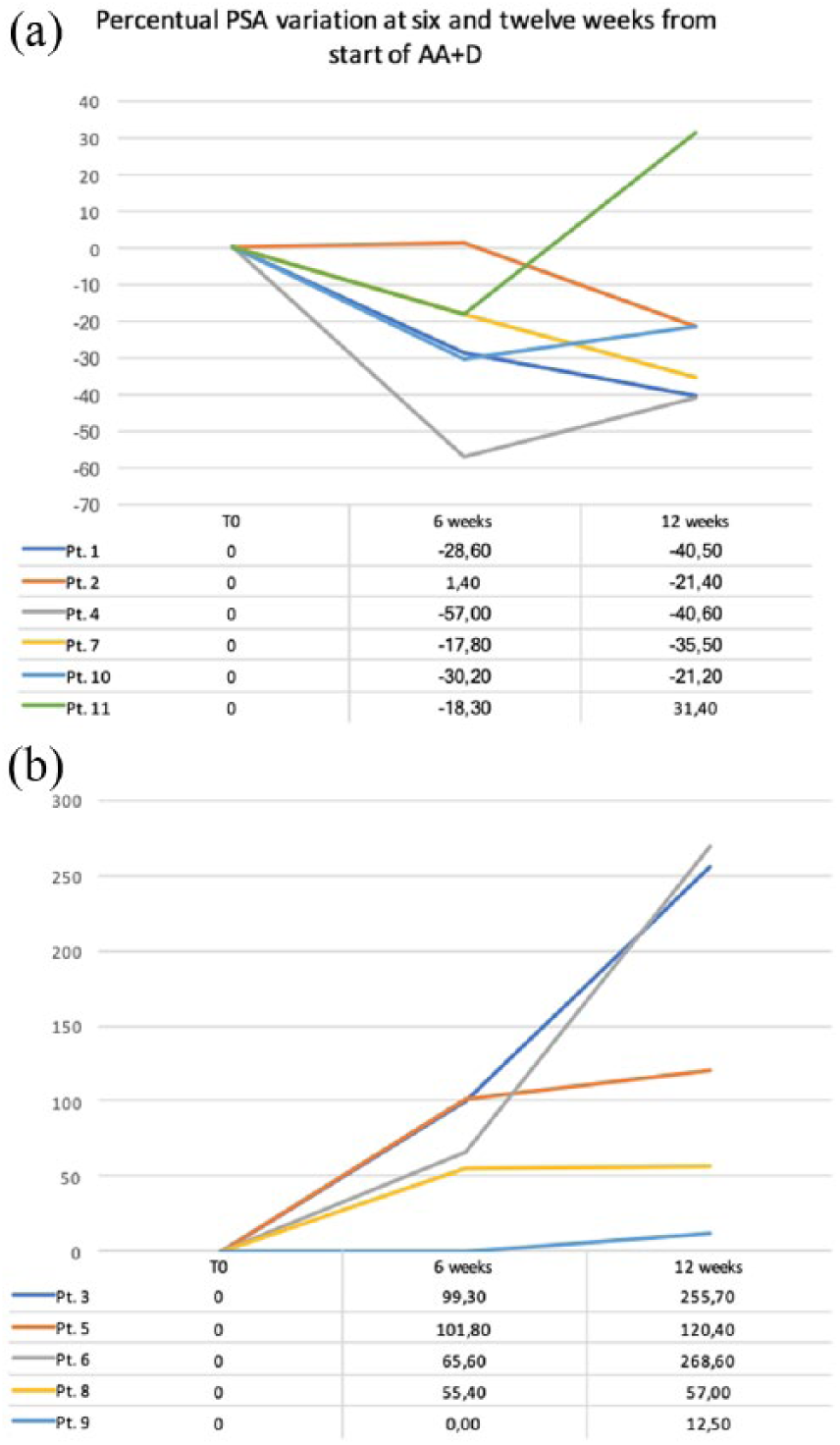
PSA trends in patients with PSA decline (a) and those with PSA progression (b) after the start of abiraterone acetate + dexamethasone. The percentage variation from baseline is given below the trends. A different scale is used to improve readability.
Conclusion
We can conclude that switching prednisone to dexamethasone during abiraterone acetate treatment produces a biochemical response, which is unpredictable both in magnitude and duration, in most cases and that sometimes this biochemical response can produce a long radiological PFS. However, to date, there is no clear indication as to which patient could benefit most from this kind of strategy; in some cases, switching might delay the beginning of more effective options like docetaxel (in patients treated with abiraterone acetate as front line) or enzalutamide/cabazitaxel (in patients treated with abiraterone acetate after docetaxel). A randomized prospective phase III trial evaluating the switch from prednisone to dexamethasone in this clinical setting, alongside molecular evaluation of biomarkers on ctDNA, could determine a specific subgroup of patients more likely to benefit from the switch. Until further data are released we believe that this approach should be limited to asymptomatic patients, with a limited tumour burden, presenting a PSA progression and/or limited radiological progression.
Footnotes
Ethical statement
Our study did not require an ethical board approval because it did not contain human or animal trials. The treatment used, abiraterone, is regularly approved in Italy for the treatment of mCRPC. All patients signed the informed consent before starting the abiraterone treatment. Furthermore, at the time of the steroid switch from prednisone to dexamethasone, all patients were informed about the rationale of this treatment strategy and provided verbal consent. The treatment programme was described in all patient charts with the date when the steroid switch was started.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
EZ is on the advisory board for Janssen Pharmaceutica.