
Abstract
Background:
Low-dose aspirin use has been correlated with an increased risk of bleeding and overall complications in surgical and invasive diagnostic procedures. In this review, our aim was to analyze the current literature on whether robot-assisted radical prostatectomy (RARP) is feasible and safe in patients taking low-dose aspirin perioperatively.
Methods:
A systematic review was performed identifying a total of 767 studies, published between January 2000 and September 2017, with five of these studies meeting the inclusion criteria for the meta-analysis, totalizing 1481 patients underwent RARP. Patients were divided into two groups: taking aspirin (group A) and those not taking aspirin (group B) perioperatively.
Results:
There were no significant differences between groups in the overall [group A 10.7% versus group B 15.7%, risk ratio (RR) 0.83; p = 0.45; I2 = 0%] or major complication rates (group A 1% versus group B 3%, RR 0.98; p = 0.98; I² = 0%), rate of cardiovascular events (group A 1.4% and group B 0.5%, RR 2.06; p = 0.24; I2 = 9%), blood loss (group A 278 ml versus group B 307 ml, SMD −0.12; p = 0.91; I2 = 96%), or hospital length of stay [group A 4 days (3–5) and group B 4 days (3–4), SMD −0.09; p = 0.52; I² = 0%]. There was a slightly higher blood-transfusion rate in group A (2.6%) versus group B (1.6%) (RR, 5.05; p = 0.04; I2 = 0%).
Conclusion:
Continued aspirin use in the perioperative period does not correlate with an increase in surgical morbidity, blood loss, or hospital length of stay. There was a slightly higher blood-transfusion rate in patients taking low-dose aspirin (group A) perioperatively.
Introduction
Low-dose aspirin (81–100 mg) is used as secondary prevention in patients with cardiovascular disease; however, its use has been correlated with an increased risk of bleeding and overall complications in surgical and invasive diagnostic procedures.1–3 Nowadays, percutaneous coronary interventions are becoming more common, and it is recognized that early cessation of aspirin can elevate the risk of cerebrovascular accident, myocardial infarction, and in-stent thrombosis.4–8 Therefore, there must be a risk–benefit analysis of discontinuing aspirin prior to a surgical procedure, examining the benefits of continuing the medication perioperatively versus stopping the medication and risking cardiovascular morbidity.
Present-day literature still has controversies regarding the continuation of aspirin during a variety of urologic procedures, such as transurethral resection of the prostate or bladder tumor, and endoscopic and percutaneous stone procedures.9,10 The robotic platform, specifically in its use for prostate cancer treatment, has significantly reduced surgical morbidity by up to 30%, perioperative bleeding risk, and decreased the blood transfusion rate by approximately 10-fold during robot-assisted radical prostatectomy (RARP). 11 Based on this rationale, some institutions have changed their practice and are having patients continue aspirin use perioperatively in those undergoing RARP who have significant cardiovascular disease and risks.
The purpose of this systematic review and meta-analysis is to analyze the current literature on whether RARP is feasible and safe in patients taking low-dose aspirin perioperatively.
Methods
Selection of studies
A comprehensive review of EMBASE, MEDLINE, Scopus, and the Cochrane Library databases was performed to include studies from 1 January 2000 to 20 September 2017. As demonstrated in Table 1, the PICOS (Population, Intervention, Control, Outcome, Study design) Search Strategy was used to construct the research question.
Database search strategy.

For this systematic review, studies were only included that utilized an intervention group of patients using low-dose aspirin (group A) versus a control group of patients without aspirin or any other anticoagulant therapy (group B) perioperatively. Furthermore, these studies were specific to patients undergoing RARP. The studies should provide adequate and detailed information regarding perioperative complications, allowing for comparison between the two groups.
The search strategy for each database is presented in Table 1. Articles that addressed any procedure other than RARP, including those who did not specify between RARP or laparoscopic radical prostatectomy were excluded. Case-control studies, literature reviews (such as updates, systematic reviews, and meta-analyses), studies that did not have a control group, and those in which the use of aspirin was not evaluated, were also excluded. There were no restrictions for the initial database search with regards to the date or language of publication, in order to determine the magnitude of the existing literature on this topic. In this search, identified papers included case-control studies, large cohorts, and clinical trials. For the systematic review and meta-analysis, study selection was based on the inclusion and exclusion criteria previously stated.
Additionally, the references of the studies which met the inclusion criteria were reviewed, and the reference articles were then analyzed for possible inclusion for the systematic review. When results of the same series were published in more than one study, the paper with the most recent and complete data and the longest follow-up period, was included for the analysis.
Data extraction
Data extraction was conducted independently by two investigators (AC and JC) according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement and any discrepancies between reviewers were resolved by consensus. 12 The following information was extracted from each study and illustrated in Table 2: first author’s name, year of publication, type of study, means age of patients, prostate-specific antigen (PSA; mg/dl), prostate size (ml), and body mass index (BMI, kg/m²), median Gleason score (GS), total number of patients, treatment groups (A or B), overall and major complication rates, blood loss and blood transfusion rates, length of hospital stay, and rate of cardiovascular events.
Baseline patient characteristics.

A, group A: patients using aspirin; B, group B: patients not using aspirin; BL, blood-loss rate; BMI, body mass index; BT, blood-transfusion rate; CE, cardiovascular events; HS, hospital length of stay; MC, major complications; MJ, ; ND, not declared; OC, overall complications; PC, prospective cohort; RC, retrospective cohort; RI, reported interval.
Clinical endpoints
The outcomes assessed included overall complications, major complications, blood loss and blood-transfusion rates, length of hospital stay, and rate of cardiovascular events. The complications were analyzed and stratified as major complications when ⩾3 according to Clavien-Dindo surgical classification. 18
Checklist and risk of bias
Quality of data was assessed by two authors (ORC and JC) using the Newcastle–Ottawa Scale (NOS; 19 Appendix 1).
Statistical analysis
For the meta-analysis, all manuscripts included in the systematic review were considered. All patients were analyzed in the study group to which they were randomized in the original study, that is, the use of aspirin or not (intention-to-treat principle).13–17
The RevMan 5.3 software from the Cochrane Library (The Cochrane Collaboration Information Management System) was used to perform all analyses. For categorical variables, the pooled estimate risk ratio (RR) was calculated using the Cochran–Mantel–Haenszel test. For continuous variables, the reverse variation test was used, and pooled continuous effect measures were expressed as the mean difference (MD). The results were graphically represented using forest plots, with 95% confidence interval (CI 95%). For all analyses, two-sided p values < 0.05 were considered significant.
The homogeneity assumption was measured by I2, which describes the percentage of total variation across studies that is due to heterogeneity rather than chance. I2 was calculated from basic results obtained from a typical meta-analysis as I2 = 100% x (Q − df)/Q, where Q is the Cochran’s heterogeneity statistic. Heterogeneity was considered acceptable when I2 < 50%, and in those cases, it was used as a fixed model. Heterogeneity was considered elevated when I2 ⩾ 50%, and in those cases, the random model was used. It is important when undertaking a meta-analysis to minimize publication bias, which, for this study, was addressed visually using a funnel plot.
Results
Selection of studies
Our initial search yielded 767 studies (270 from EMBASE, 51 from MEDLINE, 428 from Scopus, and 18 from the Cochrane Library). After removing 154 duplicate studies, the title and abstracts of the remaining 613 studies were evaluated. As result of this review, 604 studies were then excluded that did not meet the inclusion criteria. The full texts of the remaining nine articles were carefully read, and four conference abstracts were excluded. Consequently, five articles (n = 1481 patients) met the inclusion criteria and were ultimately selected for use in the meta-analysis (Figure 1).13–17
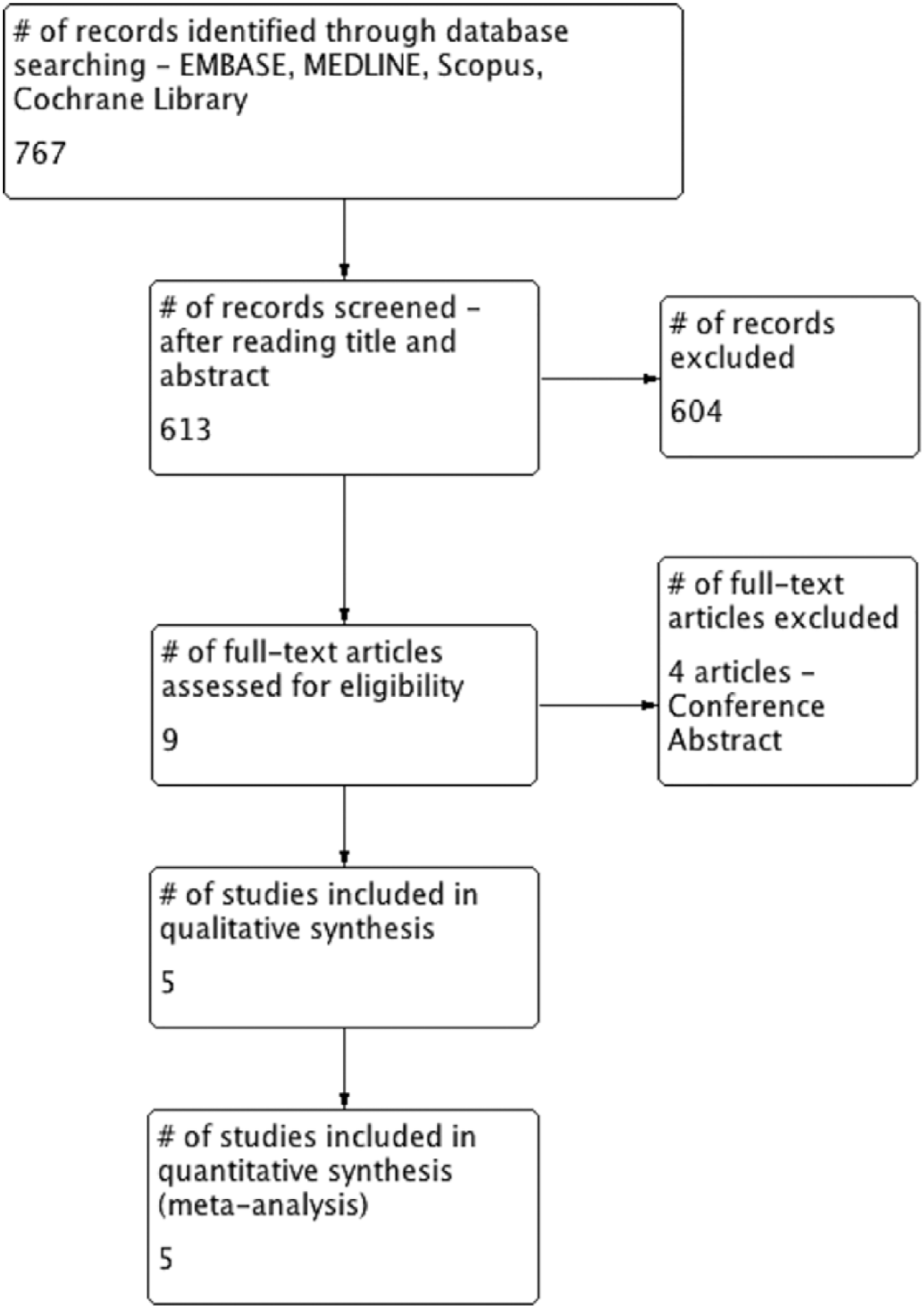
Flow diagram: selected studies.
Of the patients undergoing RARP in these five studies, 168 (11.4%) continued to take aspirin perio peratively (Group A) and 1313 (88.6%) stopped the use of aspirin preoperatively (Group B). The follow up of patients in these five studies ranged between 4 (±0.5) and 222 (±249) days. The baseline characteristics of patients included in each study are shown in Table 2. The selected observational studies included patients age 65 years or older with prostate adenocarcinoma treated by RARP. The patients had similar pathologic stage and PSA, but heterogeneous prostate size and BMI.
Incidence of overall complications and cardiovascular event rate
Four studies with 623 patients (149 in group A and 932 in group B) were included to assess the overall complication rate.13–16 One study was excluded from this analysis, as there was no comparison of complication rates between groups A and B. 17 The overall complication rate was 15%, without a statistically significant difference between the two groups, group A 10.7% versus group B 15.7% [RR 0.83; 95% CI 0.50–1.36; p = 0.45; I2 = 0%; Figure 2(a)].
Three studies with 458 patients (95 in group A and 363 in group B) were included to assess the number of major complications.14–16 Two studies were excluded from this analysis; one study did not specify complications according to severity 13 and the other study did not compare the results between the two groups in question. 17 Major complications were 1% in group A compared with 3% in group B [RR 0.98; 95% CI 0.19–5.08; p = 0.98; I² = 0%; Figure 2(b)]. The most common major complication was urinary leakage postoperatively in three patients (all belonging to group B), category 3A on the Clavien-Dindo surgery classification. 18
Four studies with 623 patients (149 in group A and 932 in group B) were included to assess the rate of cardiovascular events perioperatively.13–16 One study was excluded because it did not present data with respect to cardiovascular events. 17 The studies defined cardiovascular events as myocardial infarction or stroke.14,15 The cardiovascular event rate was similar between both groups; group A 1.4% and group B 0.5% [RR 2.06; 95% CI 0.61–6.97; p = 0.24; I2 = 9%; Figure 2(c)]. There was one death among all patients, in both groups. This patient, as described by Nowfar et al., aspirated after vomiting, resulting in acute respiratory distress, leading to sepsis and multiorgan failure. 14

Incidence of overall and major complications, and cardiovascular event rate.
Blood loss and transfusions
The five included studies were evaluated for blood loss and transfusion rates, to include 1481 patients: group A with 1313 who stopped aspirin and group B with 168 who continued aspirin use.13–17 The estimated perioperative bleeding rate was similar between group A and group B; 278 ml and 307 ml on average, respectively [MD −9.39; 95% CI −60.46 to 41.69; p = 0.72; I2 = 92%; Figure 3(a)]. A subanalysis was performed excluding two studies to control high heterogeneity present in this comparison.15,17 The remaining three studies, including 986 patients, demonstrated the same result in terms of the amount of blood loss between groups, but without heterogeneity [MD −13.33; 95% CI −36.75 to 10.10; p = 0.26; I² = 36%; Figure 3(b), (c)].13,14,16
Additionally, for the evaluation of blood-transfusion rates between the two groups, four studies were included, totaling 858 patients.14–17 One study was excluded from this analysis because it did not describe blood loss and transfusion rates for the two groups. 13 The overall transfusion rate was slightly higher in group A (2.6%) in comparison with group B (1.6%) [RR, 5.05; 95% CI 1.06–24.04; p = 0.04; I2 = 0%; Figure 3(d)].
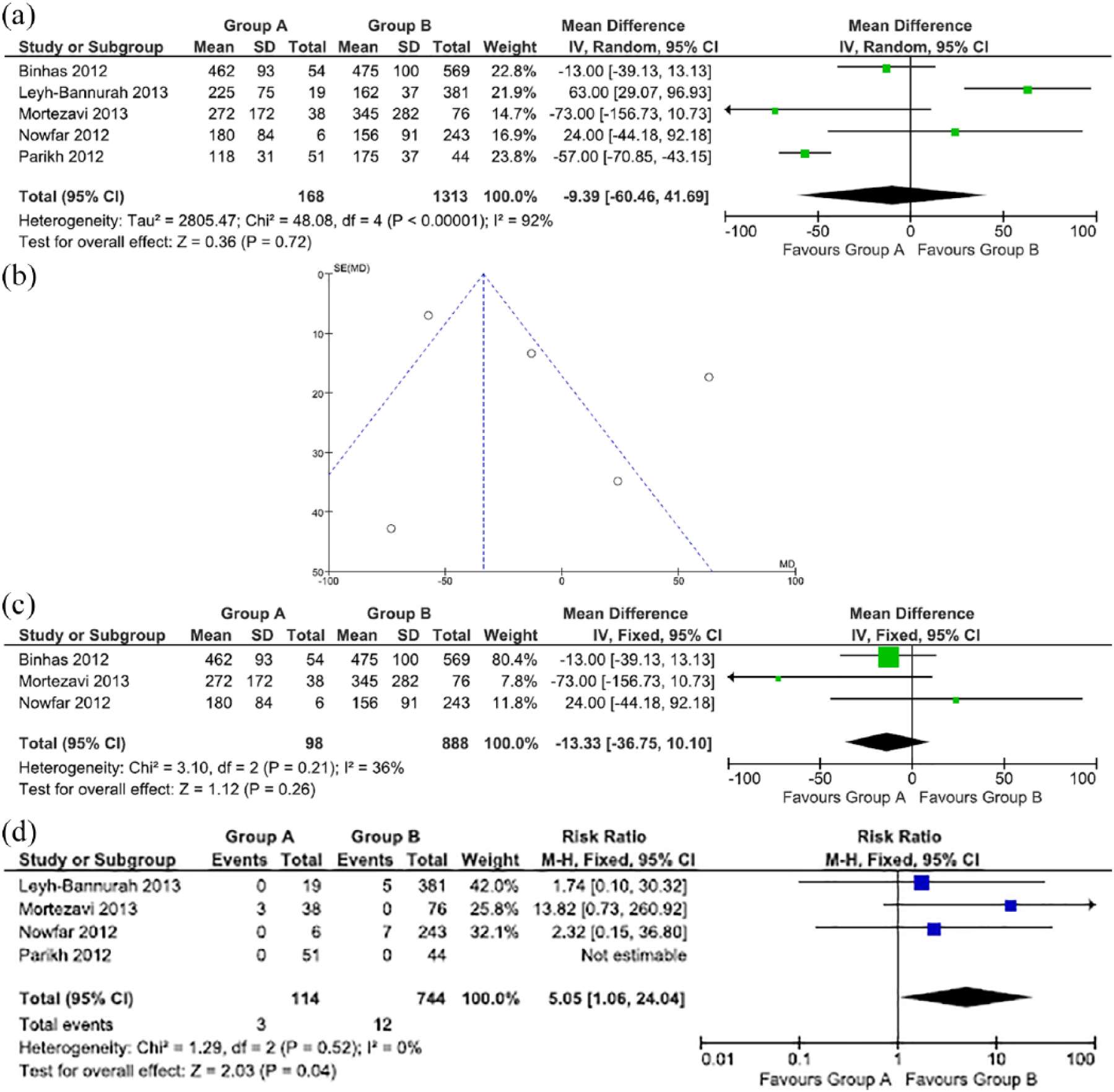
Blood loss and transfusion rates.
Hospital length of stay
Three studies with 458 patients (95 in group A and 363 in group B) were included for the hospital length-of-stay analysis.14–16 The hospital length of stay was similar between groups, group A (95 patients) 4 days (3–5) and group B (363 patients) 4 days (3–4) [MD 0.00; 95% CI −0.04 to 0.04; p = 0.99; I² = 0%; Figure 4]. One study was excluded because it did not report on this outcome. 17 The study by Binhas and colleagues was not included in the analysis because their results were reported in median; this study was therefore not comparable with the other four included studies, which reported their results in mean. 13 Binhas and colleagues also did not present difference in relation to hospital length of stay between group A (54 patients) and B (569 patients), 4 days (3–5) versus 4 days (3–4) days, respectively (p = 0.668).

Hospital length of stay.
Discussion
The data from this meta-analysis suggests that RARP performed on patients taking low-dose aspirin is feasible, safe, and not correlated with an increased risk of perioperative surgical morbidity, blood loss, or longer hospital stay. Only blood-transfusion rate was slightly higher in patients taking low-dose aspirin perioperatively.
Previous studies reported severe bleeding complications in aspirin-treated patients undergoing transurethral resection of the prostate (TURP) and higher bleeding risk with open radical prostatectomy (ORP).1,20 For this reason, the practice of many urologists was to discontinue aspirin use 5–10 days prior to most urologic procedures. Consumption of low-dose aspirin has been reported to be feasible and safe for small-to-medium urologic procedures (such as prostate and bladder photovaporization, and prostate biopsies), and even categorized as low risk for significant hemorrhage during open simple prostatectomy and renal surgeries. However, concerns regarding the feasibility and safety of continued aspirin use before and during major operations, such as open or minimally invasive radical prostatectomies, have sparked recent controversies and debate.9,10
In parallel with this is the fact that the number of patients with cerebrovascular or coronary heart disease is growing worldwide. Consequently, the use of coronary stents and antiplatelet drugs is increasing. It is estimated that two million patients undergo coronary angioplasty and stenting in Western Europe and the United States each year. 21 Several reports have also demonstrated that preoperative cessation of antiplatelet therapy for invasive noncardiac procedures, especially in patients presenting with coronary stents, is increasing the risk of cardiovascular complications.6,7 This 10-day aspirin withdrawal practice is responsible for up to 10.2% of new acute cardiovascular syndromes. 22 During surgical procedures, there is an increased synthesis of procoagulant factors due to associated tissue trauma. This is exacerbated by the sudden cessation of antiplatelet therapy which, in addition to restoring thrombotic function, induces a rebound of hypercoagulability with prothrombotic effects.23–25 These findings lead the American College of Chest Physicians and European Society of Cardiology to recommend aspirin continuation in patients who have been preoperatively treated with antiplatelet agents.26,27
In the context, specifically of the surgical procedure, radical prostatectomy, when comparing ORP versus robotic approaches, RARP has been shown to reduce hemorrhagic complications and morbidity due to its inherent minimally invasive approach.28–31 Consequently, continuing aspirin during RARP seems rational, with no significant increased risk of perioperative complication. Furthermore, current RARP literature has demonstrated that continuing aspirin use perioperatively is feasible and may be superior to ORP in respects to rate of blood transfusions (21.2% in ORP versus 0% in RARP), and major complication rates (7.6% in ORP versus 5.3% in RARP). 17 These findings can be explained by the following: increased intra-abdominal pressure due to pneumoperitoneum, enhanced precision and intuitive surgical movements, and an improved surgical field and visualization achieved with the robotic platform.
Our findings are in concordance with previous reports published in literature, demonstrating that continued use of low-dose aspirin (81–100 mg) is feasible and safe, even for major oncologic surgical procedures by minimally invasive approach. 17 We did not find significant differences regarding overall and major complications, blood loss, or hospital length-of-stay rates. It is only with respect to blood-transfusion rates that patients taking low-dose aspirin perioperatively have a slightly higher rate. It is important, however, to consider the difference between the studies in the hemoglobin threshold for administering a blood transfusion. Patients that continued aspirin intake perioperatively, at baseline, carried higher preoperative major cardiovascular risks and, therefore, higher hemoglobin cut-offs were adopted for this group. This may explain the slightly higher blood-transfusion rate identified for group A when compared with those patients who discontinued aspirin use perioperatively (2.6% versus 1.6%), suggesting a lower tolerance of bleeding in this group of patients. This effect, therefore, could potentially impact the analysis of blood-transfusion rate and represent a selection bias. Additionally, the literature has shown low rates of blood transfusion (1.5–4.0%) after RARP, in agreement with the results of both groups analyzed in this current meta-analysis, minimizing the real effects of this statistical difference between group A and B. 32
Furthermore, this result should be tempered due to the high heterogeneity between the studies. It is important to consider other factors related to bleeding, such as surgical experience, BMI, prostate size and weight, use of general anesthesia, neurovascular bundle preservation, and selective versus standard ligature of the deep venous complex.33–35
This current systematic review and meta-analysis presents some limitations which should be acknowledged. First, none of the included five studies were prospective or randomized. Second, this study included a limited number of trials, although the whole of population analyzed was quite large, some were excluded due to the inclusion criteria set for this review. This could lead to an underestimation of the complication, blood loss, and transfusion rates between group A and group B patients, and as a result, explain the absence of a statistical difference between the groups. Another potential selection bias is represented by the cardiovascular indication for aspirin medication.36,37 Consequently, patients of group A, who continued aspirin use perioperatively, were usually older and had more baseline comorbidities, leading to overall increased complication risks. 38 Finally, some of these patients might have had a low-risk cancer and could have been eligible to active surveillance, once they presented PSA mean < 10 mg/dl and GS median < 8.
This study, to our knowledge, is the first meta-analysis evaluating the impact of continued aspirin therapy during a major urologic robot-assisted surgery. Our methodology fulfilled high-quality requirements for meta-analysis reporting. Most previous studies tended to address perioperative management of antiplatelet and anticoagulants together; however, our report selection distinguished between perioperative management of antiplatelet therapy and anticoagulants separately, which allowed for an enhanced evaluation of perioperative complications.39,40 Further investigations will need to be conducted that are randomized and prospective, which compare antiplatelet therapy continuation and cessation in a patient population specifically with preoperative cardiovascular disease or risk factors, to confirm these results.
Conclusion
The present study is the first meta-analysis of patients continuing aspirin use before and during a major urologic robot-assisted surgery. The continuation of aspirin, in a low, prophylactic dose, does not correlate with an increased risk of perioperative surgical morbidity, blood loss, or hospital length of stay. Performing RARP on patients taking low-dose aspirin appears to be feasible and safe, with no significant increased risk of perioperative morbidity, except for a slightly higher transfusion rate in these patients.
Footnotes
Appendix 1
Newcastle–Ottawa quality assessment scale cohort studies.

| Studies | Binhas et al. 13 | Nowfar et al. 14 | Parikh et al. 15 | Mortezavi et al. 16 | Leyh-Bannurah et al. 17 |
|---|---|---|---|---|---|
|
|
|||||
| 1. Representativeness of the exposed cohort | B | B | B | B | B |
| 2. Selection of the nonexposed cohort | A | A | A | A | A |
| 3. Ascertainment of exposure | A | A | A | A | A |
| 4. Demonstration that outcome of interest was not present at start of study | A | A | A | A | A |
|
|
|||||
| Comparability of cohorts on the basis of the design or analysis | AB | AB | AB | AB | AB |
|
|
|||||
| 1. Ascertainment of exposure | A | A | A | A | A |
| 2. Was follow up long enough for outcomes to occur | A | A | A | A | A |
| 3. Adequacy of follow up of cohorts | A | A | A | A | A |
A study can be awarded a maximum of one star for each numbered item within the selection and outcome categories. A maximum of two stars can be given for comparability.
Acknowledgements
Conception and design: Arie Carneiro and Jonathan Cha.
Data acquisition: Arie Carneiro and Jonathan Cha.
Data analysis and interpretation: Arie Carneiro, Willy Baccaglini, Fatima Husain, Oliver Claros and Marcelo Wroclawski.
Drafting the manuscript: Arie Carneiro, Willy Baccaglini, Igor Nunes-Slva, Natahsha Moran and Paulo Kayano.
Critical revision of the manuscript for scientific and factual content: Arie Carneiro, Jonathan Cha, Willy Baccaglini, Fatima Husain, Rafael Sanchez-Salas, Alex Ingels and Rene Sotelo.
Statistical analysis: Willy Baccaglini and Paulo Kayano.
Supervision: Gustavo Lemos.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.