
Abstract
Background:
Urogenital tuberculosis (UGTB) is one of the great imitators; it is commonly masked by urinary tract infections (UTIs). We aimed to estimate how many UGTB patients were among patients with a long history of UTIs.
Material and Methods:
A total of 244 patients with recurrent UTIs and suspected UGTB were enrolled in an open, noncomparative prospective study. Their urine and expressed prostate secretion or ejaculate were cultured (a total of 1446 samples), and 421 isolates with growth of ⩾104 colony-forming units (CFU)/ml were investigated for drug resistance. Typically, UGTB diagnosis is made by individual case.
Results:
All 244 patients had a long history of recurrent UTIs (on average, 7.9 ± 3.4 years); all received at least five courses of antibacterial therapy without good result. UGTB was diagnosed in 63 (25.8%), and in 41 of these (65.1%), there was comorbidity of UTI and UGTB. Of 1446 samples investigated, 421 (29.1%) were positive, and 1025 were negative. Escherichia coli was found in 57.3% of gram-negative microflora and in 29.0% only among all uropathogens. E. coli was resistant to amoxicillin/clavulanate in 51.5–57.1%, to cefotaxime in 50.0–52.0%, to gentamycin in 33.3–59.5%, to ciprofloxacin in 63.2–66.7%, to levofloxacin in 54.8–45.2%, and to nitrofurantoin in 23.5–20.8% in 2015 and 2016, respectively. If, in 2015, all isolates of E. coli were susceptible to imipenem, in 2016, 7.1% of strains were resistant to this antibiotic. Level of drug-resistance was higher in 2016, excluding only levofloxacin and nitrofurantoin.
Conclusions:
Total prevalence of UGTB among UTI patients with poor results of antibacterial therapy was 25.8%. Comorbidity of UTI and UGTB was diagnosed in 65.1%.
Keywords
Introduction
With a new strategy, the World Health Organization (WHO) aims to eliminate tuberculosis (TB) by 2035, 1 but the epidemic tendency has a negative outlook: in 4 years (from 2012 to 2015), incidence increased from 8.6 million people to 10.4 million people, and mortality, from 1.3 million to 1.8 million.2–4 The TB epidemic is much larger than earlier thought, particularly in the WHO southeast Asia region. This is because in 2015, there were 4.3 million ‘missing cases’. 1
Tuberculosis is a multisystemic disease with myriad presentations and manifestations. The second to third most common form of extrapulmonary tuberculosis is urogenital tuberculosis (UGTB).5–8 Actually, UGTB is not a rare disease but it is often overlooked. The most common reasons for delayed diagnosis are absence of typical clinical features and the tendency of UGTB to be masked by another disease, mainly urogenital tract infections (UTIs). 7 Currently ‘sterile pyuria’ may be found in 25% only, 7 which makes it additionally difficult for a differential diagnosis.
UTIs are amongst the most common infectious diseases affecting millions of people and carry a significant impact on quality of life.9,10 Infections of the genital tract (both sexually transmitted infections and uropathogens) are considered common causes of male fertility disorders, with a prevalence of 6–10%. 11 UTIs and asymptomatic bacteriuria are frequent in elderly patients and in pregnancy. 10 Extra-intestinal pathogenic Escherichia coli represent an emerging pathogen, with pandemics involved in cases of UTIs, bacteremia, and meningitis. 12 Infections of the urine, bladder and kidneys by uropathogenic E. coli (UPEC) may lead to potentially fatal bloodstream infections. 13
UTIs are first in a rank of differential diagnosis with UGTB. Presence of various pathogens in urine makes identification of Mycobacterium tuberculosis (Mtb) very difficult and even sometimes, impossible. UTIs mask UGTB, and a patient with pyuria and bacteriuria receives more and more antibiotics instead of being investigated for UGTB.
The purpose of our study was to estimate a prevalence of UGTB among patients with a long history of UTIs, to estimate a spectrum of microflora in patients with a long history of recurrent UTIs, evaluate drug resistance of uropathogens in patients with ineffective antibacterial therapy for UTIs.
Materials and methods
A total of 244 consecutive patients with recurrent UTIs and suspected UGTB were enrolled in an open, noncomparative prospective study. Their urine and expressed prostate secretion or ejaculate were cultured, and 421 isolates with growth of ⩾104 colony-forming units (CFU)/ml were investigated for drug resistance.
Diagnosis of UGTB is typically made by individual case.
Inclusion criteria for patients were:
male and female patients > 18 years;
history of recurrent UTI > 2 years;
recurrence of UTI three or more times annually;
⩾20 leukocytes in the mid-stream urine;
presence at least one symptom of UTI (flank pain, dysuria, etc.).
Exclusion criteria for patients were:
comorbidity with stone disease;
urinary cancer;
sexually transmitted diseases;
benign prostatic hyperplasia;
constant urinary catheter;
recent surgery on urogenital organs.
Inclusion criteria for uropathogens: growth ⩾ 104 CFU/ml.
We analyzed a spectrum of uropathogens and their susceptibility. Matrix-assisted laser desorption/ionization time of flight mass spectrometry has been used for microbial typing and identification at the subspecies level. Rapid identification was made on Becton Dickinson Biosciences (San Jose, CA, USA). For antimicrobial susceptibility testing, we used the Phoenix 100 (Becton Dickinson Biosciences, CA, USA).
Investigation for Mtb was performed by the following methods: A sample was centrifuged at 3000g. Sediment was cultured on the Lowenstein-Jensen medium modified analogue of medium Finn II (HiMedia Laboratories Pvt. Limited, India) and Lovenstain-Jensen media (Becton Dickinson Biosciences, USA); also, each centrifuged sample was cultured on Middlebrook 7H9 BBLTM MGITTM broth (Becton Dickinson Biosciences, USA). Tubes were incubated in a thermostat at temperature 37°C for 90 days with control weekly. Also, each centrifuged sample was cultured on Middlebrook 7H9 BBLTM MGITTM broth (Becton Dickinson Biosciences, CA, USA) in 0.5 ml. Inoculated test tubes with a dense nutrient medium were incubated in a thermostatically controlled environment at temperature 37°C. Daily viewing of the inoculated tubes was carried out.
Inoculated-with-MGIT tubes were incubated in the BACTEC MGIT 960 system (Becton Dickinson Biosciences, USA) to automatically indicate the presence of growth, which was confirmed by smear microscopy, dyed using the Ziehl–Neelsen method. Positive tubes were removed, while tubes lacking growth continued incubating for up to 42 days for the final result.
Results
All 244 patients were consecutively recruited from the Urogenital Clinic of Novosibirsk Research TB Institute for 2 years (January 2015–December 2016) for differential diagnosis, as they failed repeated courses of antibacterial therapy for UTIs and so were suspected of having UGTB. There were 138 female patients and 106 male patients. All patients were informed they would be enrolled in a study and all signed informed consent. All patients had a long history of UTIs (on average, 7.9 ± 3.4 years, range 2–15 years); all received at least five courses of antibacterial therapy (on average, 12.7 ± 2.9, range 5–18 years), without good result. Among all 244 examined patients, UGTB was diagnosed in 63 (25.8%), and in 41 of these (65.1%), there was comorbidity of UTI and UGTB. None of the patients had asymptomatic bacteriuria. Data are summarized in a Table 1.
Characteristics of patients with repeated ineffective antibacterial therapy for urogenital tract infections.

UTI, urogenital tract infection; UTGB, urogenital tuberculosis.
All patients had more than one symptom.
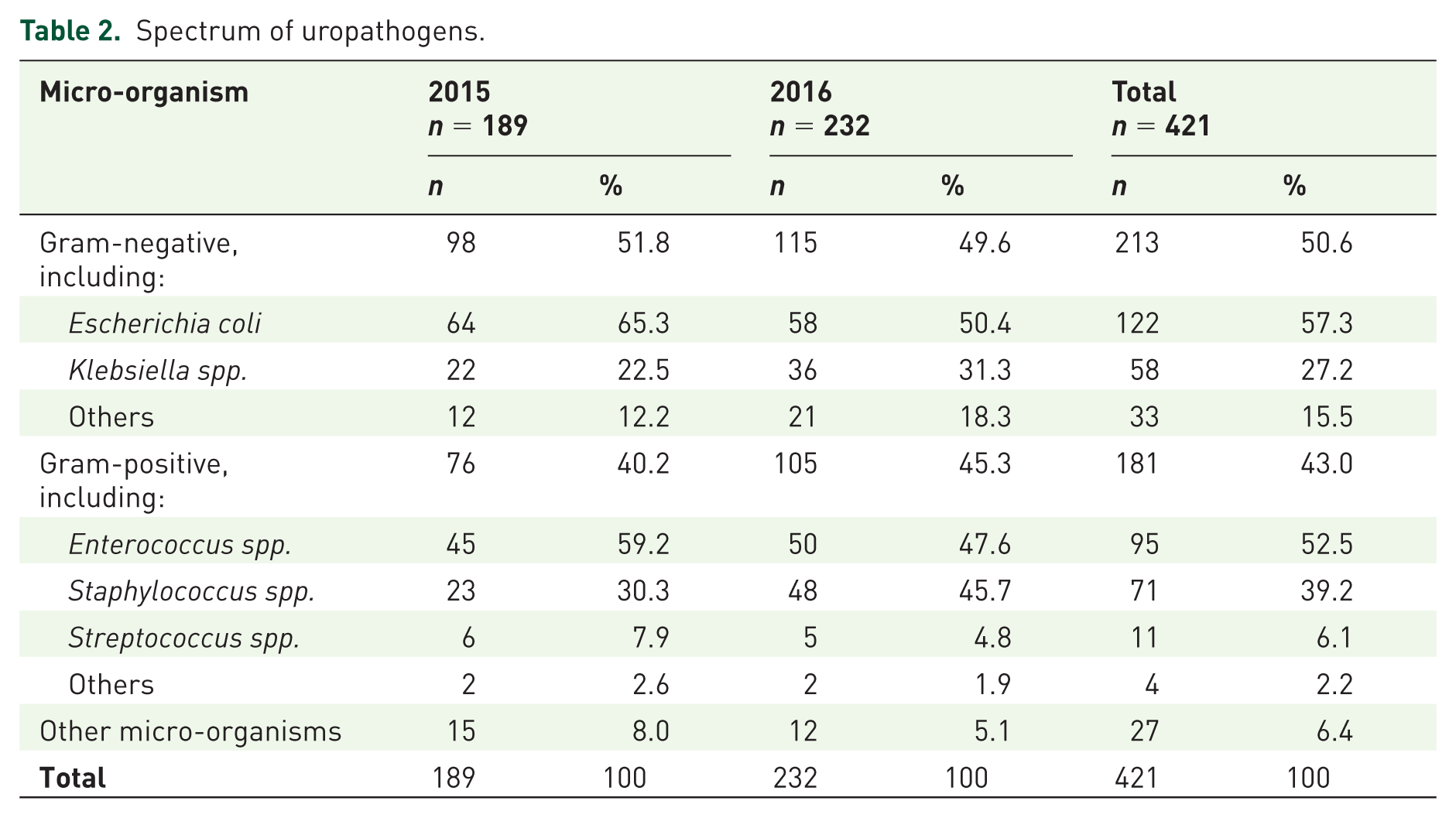
In half of all microflora there were gram-negative micro-organisms; among them, E. coli prevailed, followed by Klebsiella spp. In half of gram-positive microflora there were Enterococcus spp. followed by Staphylococcus spp. Among all uropathogens, E. coli was found in 29.0% only. The spectrum of uropathogens is shown in a Table 2.
Spectrum of uropathogens.
Resistance of uropathogens is shown in a Table 3. Only imipenem had suitable activity: in 2015, all strains of E. coli and Klebsiella were susceptible to this antibiotic, although in the following year, 7.1% of E. coli isolates and 50.0% of Klebsiella isolates were resistant to imipenem. Resistance to fluoroquinolones was observed in 45.2–92.0%; resistance to nitrofurantoin varied from 0% to 100%. All other antibiotics were inactive in about half of cases.
Resistance of uropathogens.
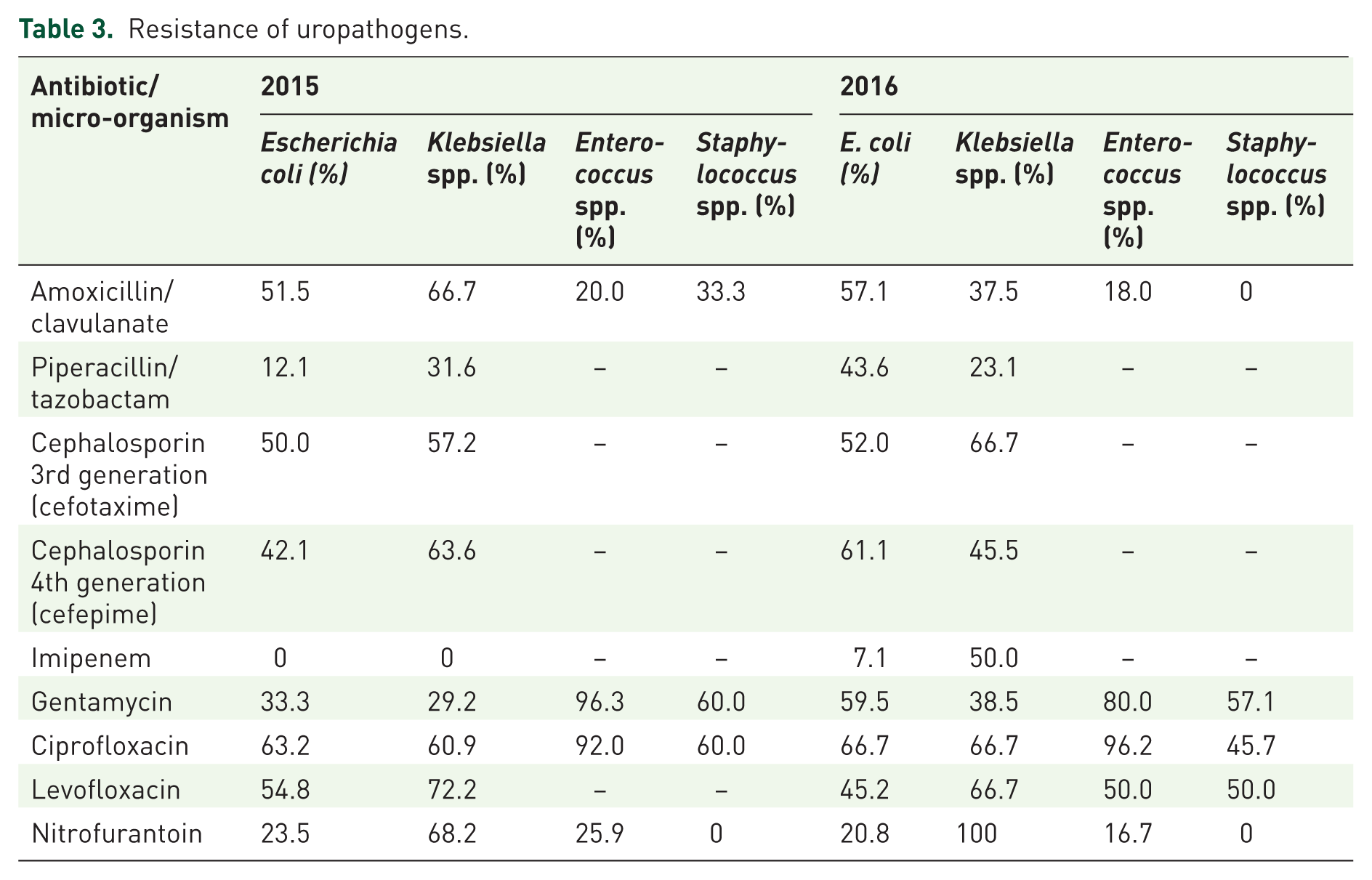
E. coli was resistant to amoxicillin/clavulanate in 51.5–57.1%, to cefotaxime in 50.0–52.0%, to gentamycin in 33.3–59.5%, to ciprofloxacin in 63.2–66.7%, to levofloxacin in 54.8–45.2%, and to nitrofurantoin in 23.5–20.8% in 2015 and 2016 years, respectively. If, in 2015, all isolates of E. coli were susceptible to imipenem, in 2016, 7.1% of strains were resistant to this antibiotic. Level of resistance to all antibiotics was higher in 2016, excluding only levofloxacin and nitrofurantoin.
Diagnosis of UGTB is typically made by individual case. A female patient aged 50 years was admitted to the Urological Clinic of Novosibirsk Research TB Institute with suspected UGTB. She presented with complaints of flank pain, urgency, and frequency. Urinalysis showed pyuria and hemogram was normal. The onset of cystitis was 25 years ago. The first episode was treated with nitrofurantoin and relapse occurred at 6 months. For the next 25 years, the patient received amoxicillin/clavulanate, gentamicin, nitrofurantoin again, cephalosporins and fluoroquinolones of a total of 18 courses, and she was not cured. Growth of multidrug-resistant E. coli 107 CFU/ml was found. Examination in the TB Institute revealed policavernous TB (4th stage) of the left kidney (Figure 1).

Multislice tomography: policavernous tuberculosis (4th stage) of the left kidney.
The patient underwent a nephrectomy: on sagittal incision of the kidney, multiple caverns were revealed (Figure 2).

The kidney after nephrectomy and sagittal incision: multiple caverns.
Diagnosis of UGTB was confirmed by pathohistology. This patient had comorbid UTI and UGTB that led to delayed diagnosis and loss of a kidney.
Discussion
Before anti-TB drugs were created, the prevalence of UGTB was huge. Every fifth urological inpatient had UGTB and more than a third of all pyonephrosis was due to TB. In that era, it was mostly young people who got sick with TB, equally male and female. 14
Recent analysis of the epidemiological situation of UGTB in Siberia and the Far East has found that late diagnosis of UGTB may be the result of suboptimal therapy for UTIs, while UGTB often manifests under their disguise. Authors concluded that currently, it is impossible to estimate the true prevalence of UGTB; we can only report the detection rate. Every fourth UGTB patient under medical supervision had a wrong diagnosis for 5 or more years. 15
UGTB is responsible for a destructive inflammation of the renal parenchyma and urinary tract, often leading to the loss of kidney function. 16 The delayed diagnosis impacts the urinary tract severely. 17 The early diagnosis of UGTB, once considered no longer present in developed countries, is very important in initiating appropriate timely therapy. However, the nonspecific clinical features, often represented by recurrent and persistent lower urinary tract symptoms, can mask disease and delay the diagnosis. Diagnosis is also difficult because of the low accuracy of conventional tests.16–17
UGTB is a serious, insidious disease, generally developing symptoms only at a late stage. 18 A spontaneous autonephrectomy with a nephrocutaneous fistula due to renal TB was described; the patient had recurrent UTI with ineffective antibacterial therapy but UGTB was not suspected. 19 Also, the case of a recurrent UTI was described. Despite antibiotic treatment, there was no symptomatic resolution. Correct diagnosis was established when imaging exams showed left ureteral stenosis with moderate hydronephrosis only; the patient underwent nephrectomy. 20
The analysis of clinical features of urinary TB in southwestern China has shown that the most common presenting symptoms were urinary irritation (61.1%) and lumbago (49.2%). High proportions of microscopic hematuria (63.2%) and microscopic proteinuria (45.6%) were also observed. These nonspecific symptoms were not a reason to suspect UGTB. 21 Even when suggestive findings such as hematuria, sterile pyuria and recurrent urinary infections are present, we rarely remember this diagnostic possibility. 18
UPEC seems to be a pathogen of major significance to global human health. 22 In Hungary, the five most commonly occurring bacteria were E. coli, Enterococcus faecalis, Klebsiella pneumoniae, Pseudomonas aeruginosa and Proteus mirabilis. 23 However, in another clinic in Germany, the role of E. coli declined: the incidence of this pathogen as well as Proteus significantly decreased in the period from 2005–2006 to 2011–2012, while enterococci and staphylococci significantly increased. 24 We have found E. coli less often, too.
So, there are very different data on the spectrum of uropathogens and their susceptibility; incidence of UTIs, pathogen resistance rates that vary according to geographical setting, living standard, accessibility of antibiotics, adherence of doctors to guidelines, and epidemiological situation, etc. 25
All patients suspected of having UGTB were treated for a long time without success. Low index of suspicion led to changing antibiotics in patients with UTI who failed therapy again and again. Finally, the main reason for this treatment failure was a transformation of their microflora, significant rising of drug resistance and late diagnosis of UGTB. Unsuccessful courses of antibacterial therapy for UTI is not an indication for changing antibiotics and increase of dose, but for an investigation for UGTB, especially in a region with high prevalence of TB. Of course, failure in the treatment of UTI may be explained by local resistance of uropathogens, by development of biofilm, by some complicated factors, and it may be due to UGTB. Use of fluoroquinolones, amikacin and imipenem, leads to hiding UGTB and obstructs both bacteriological and histological confirmation of UGTB, but doesn’t cure disease. So, a patient with UGTB, misdiagnosed as UTI, and treated with strong antibiotics, became a chronic patient with frequent relapses. Sooner or later (unfortunately, more often, later), UGTB will be revealed, but by this time, high resistance of microflora, as well as complications of UGTB, will develop.
Conclusion
Total prevalence of UGTB among UTI patients with poor results of antibacterial therapy was 25.8%. UTIs are one of the most common masks of UGTB, and comorbid UTI and UGTB was diagnosed in 65.1%. Ineffectiveness of standard antibacterial therapy for UTI is an indication for an investigation for UGTB, at least in regions with high prevalence of the disease.
Footnotes
Authors’ contribution
EK designed the study; AC performed the investigations; EK analyzed the data and wrote the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.