
Abstract
Background
The objective in this paper was to validate the prognostic performance of the American Joint Committee on Cancer (AJCC) 7th and 8th systems among prostate cancer patients treated with radical prostatectomy.
Methods
The surveillance, epidemiology and end results (SEER) database (2006–2014) was accessed through the SEER*Stat program and AJCC 7th and 8th editions were calculated utilizing T, N and M stages, histological grade group, as well as baseline prostatic-specific antigen (PSA). Cancer-specific and overall survival analyses according to 7th and 8th editions were conducted. Moreover, multivariate analysis was conducted through a Cox proportional hazard model.
Results
A total of 72,999 patients with prostate cancer were identified in the period from 2006 to 2014. Overall survival was assessed according to AJCC 7th and 8th staging systems. The test for trend for overall survival was significant (p < 0.0001) for both staging systems. Concordance index for AJCC 7th system was: 0.791 [standard error of the mean (SE): 0.017; 95% CI: 0.758–0.825]; while concordance index for AJCC 8th system was: 0.840 (SE: 0.015; 95% CI: 0.811–0.869). In a multivariate analysis among patients with M0 disease, lower grade group, N0 stage and pT2 stage were associated with better cancer-specific survival (p < 0.01); while PSA level did not predict cancer-specific survival.
Conclusion
There is a clear improvement in the discriminatory ability for AJCC 8th versus AJCC 7th staging system in the postprostatectomy setting. This may be related to better integration of biological factors into the staging system.
Introduction
As the second leading cancer among men and the fourth leading cancer in both sexes, prostate cancer is a global health problem. In 2012, about 1.1 million patients were estimated to be diagnosed with prostate cancer according to GLOBOCAN. 1 Likewise, prostate cancer is the fifth leading cause of death from cancer in men. 2
In order to establish a proper treatment plan for a case of prostate cancer, multiple domains have to be accounted for, namely: functional domain (including comorbidity and fitness) and tumor domain (including histological grade and stage). 3 The most common staging system for prostate cancer is the American Joint Committee on Cancer (AJCC) system and its successive editions have been published reflecting advances in our understanding of prostate cancer prognosis. 4 For prostate cancer, two different versions of the AJCC staging system were published: the pathological and the clinical staging systems.
Recently, the 8th edition has been published in December 2016 and its implementation was postponed till January 2018.5,6 Important changes in the 8th edition include: (a) pT2 should not be sub-classified based on laterality or extent; (b) grade should be represented by the grade grouping system proposed by the international society of urologic pathology (ISUP); (c) T4N0M0 disease was moved from stage IV to stage IIIb; (d) newer substages were introduced within the domain of stage II and stage III.
The value of successive editions of the AJCC system has been widely accepted among clinically staged patients treated with nonsurgical modalities;7,8 however, it remains to be seen if it is similarly predictive of outcomes among surgically treated/pathologically staged patients.
Evaluation of the prognostic value of the AJCC staging system in the postprostatectomy setting would help clarify its role in the decision-making process; moreover, this may help future improvements in the staging system. The surveillance, epidemiology and end results (SEER) database is a relevant source for this evaluation, as well as for exploration of further refinements because of its rigorous quality assurance and broad coverage. 9
Objective
My objective in this study was to assess the predictive value (for survival) of the AJCC staging system (both 7th and 8th editions) in a cohort of patients with prostate cancer who were treated with radical prostatectomy.
Methodology
The records of this study were extracted from the SEER-18 registry custom data (with additional treatment fields); 10 in lieu of doing this, SEER*Stat software Version 8.3.4 was used.
Selection of the study cohort
The SEER database search was limited to the period from 2006 to 2014 (because of changes in Gleason grading system in 2005). To recruit suitable cases, the International Classification of Diseases-Oncology (ICD-O-3)/World Health Organization 2008 category of ‘prostate’ was chosen. In order to restrict the recruitment to patients treated with radical prostatectomy, cases with radical surgical treatment only were selected. Records with insufficient data about survival, TNM sixth stage, baseline prostatic-specific antigen (PSA) level or Gleason grade/grade group were excluded.
Data collection
Information extracted for each case included age at diagnosis, T, N and M stages (according to the 6th edition), race, PSA level, Gleason grade (both according to the preoperative needle biopsy, as well as according to the surgical specimen), postoperative radiotherapy or systemic therapy (if available) and cause-specific death classification and survival months. AJCC 7th and 8th stage groups were calculated for each case according to PSA, Gleason grade/grade group, available T/N/M stages and pathological tumor extension. Grade groups were calculated based on the available Gleason scores and according to the proposal of the International Society of Urological Pathology: group 1: Gleason score
In the current study, prostate-cancer-specific survival was defined as time from diagnosis to death from prostate cancer. Information about performance and comorbidity score was not available in the SEER database.
Statistical considerations
In this analysis, log-rank testing and Kaplan–Meier analysis were employed for overall survival comparisons according to 7th and 8th editions of the AJCC. Cox proportional hazard model was employed to conduct multivariable analyses; and hazard ratios (with corresponding 95% confidence interval) were produced for factors affecting cancer-specific survival. Concordance index (c-index) was also calculated for the AJCC 8th system as well as for any proposed modification and using mortality from prostate cancer as the dependent variable. C-index was calculated through binary logistic regression followed by a calculation of the area under receiver operating characteristics (ROC) curve. A result was considered statistically significant if a two-tailed p value was <0.05. All of the analyses were conducted through SPSS Statistics 20.0 (IBM, New York, USA).
Results
Patients’ characteristics
A total of 72,999 patients with prostate cancer were identified in the period from 2006 to 2014 and they were included in the study. All patients have undergone surgical treatment of the primary tumor. Complete information about TNM 6th edition, pathological tumor extensions, PSA level, as well as Gleason grade/grade group was available for all patients. Adenocarcinoma, NOS (not otherwise specified) represented the majority of cases (99.9%). Age group < 70 years was 88.3%; while age group
Baseline characteristics of included patients in the study (72,999 patients).

PSA, prostate-specific antigen; AJCC, American Joint Committee on Cancer; NOS, not otherwise specified.
Survival outcomes
Overall survival was assessed according to AJCC 7th and 8th staging systems. The test for trend for overall survival was significant (p < 0.0001) for both staging systems. Moreover, 5-year overall survival according to each stage for both staging systems was reported in Figure 1a and 1b.

Kaplan–Meier curve of (a) overall survival according to the American Joint Committee on Cancer (AJCC) 8th edition; (b) overall survival according to the AJCC 7th edition.
Adjusted cause-specific (cancer-specific) hazard was also assessed according to AJCC 7th and 8th staging system. Moreover, pair-wise hazard ratio comparisons were also conducted among different stages in the 7th and 8th systems (Figure 2a and 2b).
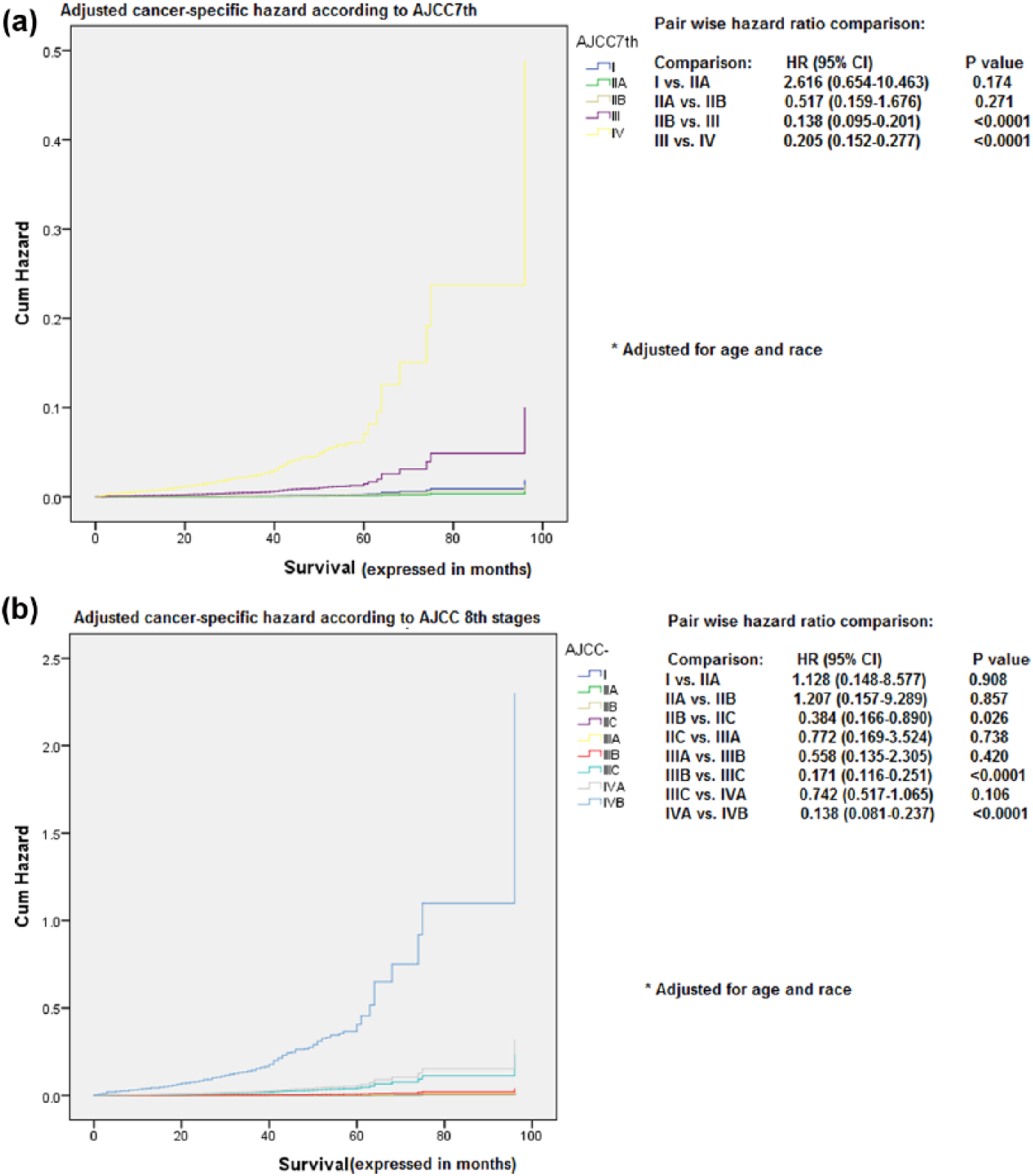
Adjusted cause-specific hazard ratio according to: (a) American Joint Committee on Cancer (AJCC) 8th edition; (b) AJCC 7th edition.*
In order to account for the discriminatory ability of each AJCC edition, c-statistic was calculated for both AJCC 7th and 8th systems. C-index for AJCC 7th system was: 0.791 (SE: 0.017; 95% CI: 0.758–0.825); while c-index for AJCC 8th system was: 0.840 (SE: 0.015; 95% CI: 0.811–0.869).
Cox proportional hazard model analysis for factors affecting cancer-specific survival among M0 patients incorporated the following factors (PSA, grade group, T stage and N stage). Lower-grade group, N0 stage and pT2 stage were associated with better cancer-specific survival (p < 0.01); while PSA level did not predict cancer-specific survival (Table 2).
A multivariate Cox proportional model for factors affecting prostate cancer-specific survival in the post-prostatectomy setting among M0 patients.

There is no pathological T1 in the TNM system for prostate cancer.
HR, hazard ratio; CI, confidence interval; PSA, prostate-specific antigen.
Discussion
The current study provided an assessment of the prognostic performance of the AJCC staging systems (both 7th and 8th) for patients with prostate cancer treated with radical prostatectomy. There is a clear improvement of the discriminatory ability of the AJCC 8th system compared with the 7th system, as evidenced by better c-index. Further work is needed to improve the prognostication of these patients.
Multiple prognostic models have been suggested for prostate cancer, both in the localized as well as advanced stages. These models were assessed by the AJCC committee of Precision Medicine Core.12,13 However, none of the proposed models dealing with localized disease was endorsed by the AJCC. The reason was a reported lack of survival impact validation.
Recent data suggested that genomic classifiers may predict metastatic disease development and augment the prognostic role of traditional pathological features in the postprostatectomy setting; and thus, they may improve the selection process of patients for adjuvant radiotherapy.14,15 It remains to be seen if genomic classifiers may improve prostate-cancer-specific mortality prediction in this setting and whether they may improve the performance of traditional prognostic tools (like the AJCC staging system).
Major setbacks of this study may include: (a) absence of sufficiently reliable and complete information about both postoperative systemic and radiation treatments in the SEER database; (b) absence of data about performance status and co-morbidity index of the included cohort; accordingly, the analysis has been based on cancer-specific plus overall survival in order to avoid any confounding effect resulting from associated co-morbidities; (c) in this relatively large population-based study, patients’ surgical procedures and pathological examinations were conducted at variable centers spanning academic high-volume prostate-cancer centers and community low-volume centers which may have affected the quality of prostate cancer surgery as well as pathological interpretation; (d) there were some concerns about the veracity of the PSA values in the SEER dataset. However, it has to be noted that in the most recent SEER submission (utilized in the current study), the quality of PSA values reported in the SEER database from 2004 to 2014 were rigorously evaluated and checked. Thus, this concern is not applicable to the dataset used in this study; (e) it is known that the SEER registrars rely on ‘best pathology’ when entering the data. If they undertake their data pull after surgery, the pathology will reflect what was seen at the time of operation. However, if they perform their data pull before surgery, then amend the record to reflect that a procedure was performed, the pathology grade and stage will rely on the biopsy and on clinical staging, which is not as reliable. In order to avoid such a confounding factor, only patients with complete surgical pathology data (histology and grade) were included in this analysis and calculations for pathological AJCC stage were made according to surgical pathology findings in all patients; (f) overall, the event rate (as shown in Figure 1a and 1b) is very low and subsequently overall and cancer-specific survival rates for localized prostate cancer are very high at 5 years. This is understood, given the good prognosis of localized prostate cancer patients treated with radical surgery. These findings indicate the need to externally validate the AJCC 8th system in a cohort with a longer follow-up period to try to increase the statistical power of the analysis. As clarified in the methods section of this manuscript, the start date of any population-based validation cohort cannot go beyond 2006 because of changes in the Gleason grading system in 2005.
Additionally, the overall low event rate may explain the nonsignificance seen in some of the pair-wise hazard ratio comparisons and this is, again, expected with a such-good-prognosis disease and presentation.
Previously, a number of validation studies have been conducted to evaluate the performance of AJCC 7th system among radiotherapy-treated patients and they showed an improved performance of the 7th system compared to the 6th system.7,8 However to the best of knowledge, none of these studies evaluated the outcomes of postprostatectomy patients.
The performance of AJCC staging system for surgically treated prostate cancer was questioned previously by many authors. 16 However, it has to be noted that most of these criticisms were directed at the 6th and 7th editions. It remains to be seen whether the 8th AJCC system, with more integration of biological factors (grade group) may play a better role in the prognostication of these patients.
The AJCC 8th staging system places more stress on histological grade in the determination of stage group. In the setting of pathological staging, the standard practice is to use the grade group derived from the surgical pathology specimen; while in the clinical staging, grade group derived from needle biopsy is used. Current analysis sheds light on the discordance between needle biopsy-based versus surgical specimen-based grade grouping in a relatively large population-based study. Further efforts are needed to improve the concordance and standardize the grade group reading between both specimens.17,18
Current treatment algorithms for surgically treated prostate cancer suggest some factors as indications for postoperative hormonal therapy with or without radiotherapy, including: positive nodal deposits (N1), seminal vesicle invasion or extracapsular extension (T3/T4 disease). These factors, in addition to aggressive tumor biology, were associated with poor cancer-specific survival in the current analysis and were included in the AJCC 8th system. Thus, the AJCC 8th system may be useful in patient counseling and therapeutic decision making for postoperative treatment.
Positive surgical margin is another factor which was associated with poor outcomes postprostatectomy. 19 However, because this information is not available in the SEER database, this factor cannot be evaluated in the current study.
Notably, although baseline (preoperative) PSA was included in the AJCC 7th and 8th system, it has no prognostic significance in the prediction of patient outcomes in the multivariate analysis. On the contrary, postoperatively persistent PSA is a well-established poor prognostic marker following prostatectomy and is a solid indication for postoperative treatment. 20 Thus, it may be suggested to remove preoperative PSA level from the pathological AJCC stage grouping and to include, alternatively, postoperative PSA level in this setting. A counter argument to this suggestion may be based on the fact that replacing preoperative PSA with postoperative PSA in various prediction tools has some drawbacks. First, it would delay time when one could calculate the predictions. Second, postoperative PSA is and should overwhelmingly be undetectable, so it may rather be put as a binary variable in the staging system (i.e. detectable or undetectable).
Cancer of the Prostate Risk Assessment-Surgery (CAPRA-S) score is another score based on pathological findings that has been shown to predict postprostatectomy biochemical recurrence-free survival, metastasis and mortality.21–23 Many similar predictive models were proposed and validated in the postprostatectomy setting (e.g. Kattan nomogram). It remains to be seen whether it is possible to integrate any of these models into future editions of the AJCC staging system. 24
There is also a particular need for population-based validation studies for the prostate cancer AJCC 8th staging system among patients from Asian countries. The incidence of prostate cancer was lower in Asian countries compared with Western countries; moreover, there is an overall higher incidence of a more advanced stage and a higher risk in patients from Asian countries.25,26 So, the prognostic performance of the AJCC 8th staging system has to be independently validated among these patients.
Consistent with the findings from the current study, a newly proposed scoring system for advanced prostate cancer (Prostascore) was published. 27 It is based on the same concepts of AJCC staging system (i.e. anatomical extent of the disease, PSA and grade) but for advanced disease (N1 or M1 disease). Hopefully, these simplified biomarker-enriched prognostic systems would improve the therapeutic stratification among patients with prostate cancer among different treatment settings.
In conclusion, there is a clear improvement of the discriminatory ability of the AJCC 8th system compared with the 7th system in the postprostatectomy setting. Further work is needed to improve the prognostication of these patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares that there is no conflict of interest.