
Abstract
Prostate artery embolization (PAE) is emerging as a safe and efficacious treatment which approaches benign prostatic obstruction (BPO) from a unique perspective. This brings with it distinct advantages and solutions, which we discuss along with cost, evidence, complications and disadvantages.
Keywords
Introduction
Benign prostatic obstruction (BPO) is a common and debilitating illness, known to significantly reduce quality of life in those patients affected by it. 1 If medical therapy fails, patients face the prospect of surgery, and with it, the risk of potentially significant associated complications and side effects. 2
Amidst a paradigm shift towards minimal access procedures for BPO, prostate artery embolization (PAE) is emerging as a viable, minimally invasive alternative to surgery. Performed as a day-case procedure, it has only a few complications, 3 while preserving fertility and sexual function, 4 with promising early clinical success rates which are beginning to match certain surgical alternatives. 5
The procedure, initially developed in Brazil and Portugal6,7 is now practiced by interventional radiologists (IRs) internationally.8,9 Despite the increasing popularity of the procedure, it is yet to gain approval by the US Food and Drug Administration, and the UK National Institute for Health and Care Excellence has deemed PAE should only be performed in a research context, pending further data. 10 With a multitude of high-quality studies in progress,11,12 this evidence void is likely to be addressed in the near future, with subsequent changes to national and international guidance.
As the practice of PAE takes off, education and mentoring is essential for its safe uptake worldwide. Clinicians must understand PAE’s role with its strengths and weaknesses to enable optimal patient selection. Equally, urologists and IRs must comprehend the important procedural principles in order to ensure the best results and minimize complications. We therefore aim to outline the method of PAE, while also discussing patient selection, challenges and other current issues facing the technique.
The procedure
The aim of PAE is to achieve targeted ischaemia of the prostate using catheter-directed particulate microembolic agents directly injected into the prostatic artery under fluoroscopic guidance, following peripheral arterial access. Subsequently, ischaemia and tissue infarction evolves with apoptosis of the BPH adenoma as the principle mechanism of action. However, androgen deprivation as well as denervation may well play an important role in reducing prostatic urethral constriction. 13
Preprocedure, workup includes computed tomography (CT) angiography of the prostatic vessels (Figure 1). This is performed as routine in some centres as variable vascular anatomy and frequent anastomoses can present technical challenges during the procedure. 14 No evidence is yet available in support of, or against, this practice. Formal urodynamic studies are advocated to ensure that obstruction is the underlying cause of the patient’s symptoms. 15

Preprocedural computed tomography angiogram delineates the prostatic vascular anatomy and aids procedure planning.
PAE is a day-case procedure performed in an angiography suite. 15 Some centres advocate urethral catheterization for the duration of the procedure with contrast medium in the catheter balloon to enable better identification of the prostatic artery but this practice varies.15,16 The availability of cone-beam CT capability (Figure 2) is an extremely desirable feature due to the importance of the technique in identifying anastomoses and thus performing embolization safely and effectively.17,18
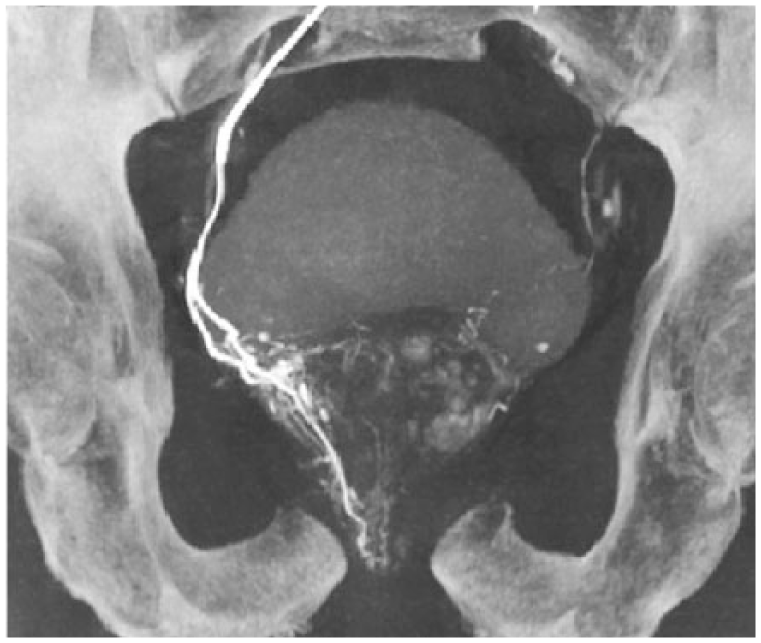
Cone-beam computed tomography during the procedure facilitates the identification of vascular anastomoses with adjacent organs which is the main risk of adverse events during prostate artery embolization.
Most commonly, right common femoral artery puncture is made under a local anaesthetic, 4 although a transradial approach has also been described. 19 The contralateral internal iliac/hypogastric artery is cannulated with a 4 or 5 Fr catheter before superselective catheterization of the prostatic artery is achieved using a coaxial approach with a 2.4–2.5 Fr microcatheter. If significant vascular anastomoses are identified, either the catheter is positioned distal to the vessel or protective coil embolization is performed. Cone-beam CT, a rotation of the C arm around the patient while injecting intra-arterial contrast, produces a three-dimensional image of the vascular anatomy, enhancement of the target tissue and allows better detection of anastomoses and assessment of their significance.17,18 Polyvinyl alcohol microparticles or spherical embolics are then injected until near vascular stasis is achieved. The procedure is then repeated on the ipsilateral side as the initial arterial puncture by forming a Waldtman loop in the contralateral common iliac artery where necessary.
Technical success is reported in 90–98% of cases, with bilateral embolization rates of 82–100%. 4 Initial evidence suggests outcomes may be similar with unilateral embolization, 20 but larger scale data collection is required before a unilateral technique can be advocated.
The procedure can be challenging due to the combination of atherosclerotic vessels in older patients, and the tortuous and variable anatomy of the pelvic vasculature. 21 These variations include more common origins of the prostatic artery, such as from the superior vesicular artery, the gluteopudendal trunk, the obturator artery and internal pudendal artery, but also with more unusual variations such as a prostatic artery arising from a replaced obturator from the external iliac artery. 22 It is therefore vital that practitioners are adequately trained. 15
Patient selection
All patients considered for surgical management of BPO could concurrently be considered for PAE. However, current evidence suggests there are clearly patients particularly suited for PAE and therefore efforts should be made to identify those patients.
Patients with a prostate volume greater than 80 cm3 or deemed unsuitable for transurethral resection of prostate (TURP) 23 are in fact those most likely to benefit from the procedure.8,24 However, a smaller study has found no such correlation between size and outcome. 17 Furthermore, patients with prominent median lobes who are excluded from other minimal access procedures such as UroLift may benefit from PAE. 25 Despite this, some urologists have found that although there is reduction in volume of the median lobe, a ball-valve effect of the lobe can cause continued symptoms. This can be managed by limited resection.
Patients keen to maintain their sexual function or preserve fertility may be particularly interested in PAE due to its advantages in minimizing this risk typically associated with other BPO surgeries. 16 Additionally, it may be the preferred option for those unsuitable for a general or spinal anaesthetic. However, typical contraindications would include patients with poor renal function, those with severe atherosclerosis of the prostatic arteries or additional issues requiring surgery (such as bladder calculi or chronic retention). These factors would preclude PAE in favour of surgical therapies (Table 1). Malignancy needs excluding if possible prior to embolization, although with close follow up (including multiparametric magnetic resonance imaging) areas of concern are occasionally picked up and can be managed as appropriate.
Advantages and disadvantages, inclusion and exclusion criteria for PAE compared with surgery.
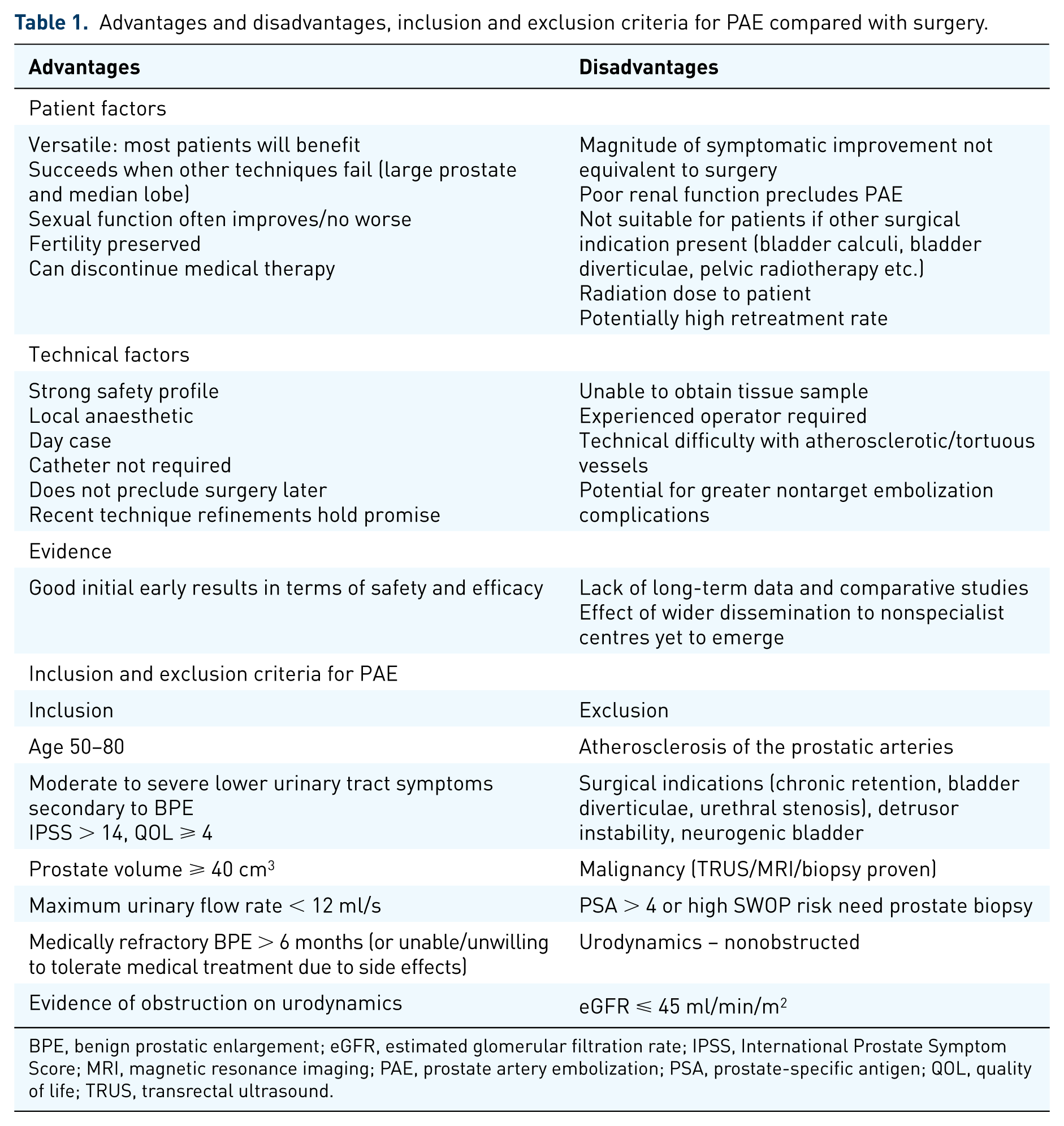
BPE, benign prostatic enlargement; eGFR, estimated glomerular filtration rate; IPSS, International Prostate Symptom Score; MRI, magnetic resonance imaging; PAE, prostate artery embolization; PSA, prostate-specific antigen; QOL, quality of life; TRUS, transrectal ultrasound.
Advantages
From a patient’s point of view, the procedure is attractive for a multitude of reasons; performed under local anaesthetic with minimal intraprocedural/postprocedural discomfort, urethral catheterization is either not required, or only for a short duration during/after the procedure. 15 Subsequent return to normal activities and work is rapid. The main benefits, however, rest with the absence of retrograde ejaculation and thus fertility preservation, in addition to maintaining or improving sexual function in up to half of patients. 16 It should be noted that fertility preservation is presumed through the absence of retrograde ejaculation and no good quality evidence is yet available to properly evaluate this claim.
From a surgical perspective, the procedure is versatile with only few exclusion criteria. PAE works well for patients in whom other surgical options are not ideal or are potentially excluded. PAE is in fact more likely to benefit those with large prostates 24 or large median lobes.25,26 Due to its low complication rate, 27 attempting PAE before considering surgery is a possible treatment strategy. Alternatively, some centres have described PAE as a planned preparatory step prior to TURP in patients with large prostates. 28
Disadvantages
Renal function, not usually a major consideration for surgery, can be an excluding factor for PAE due to contrast requirements during the procedure. Furthermore, patients with other surgical indications such as bladder calculi, diverticulae or previous pelvic radiotherapy are also unsuitable for PAE. 15 The technique does not enable tissue sampling and atherosclerotic or tortuous prostatic vessels can present obstacles during PAE. 15
PAE also involves ionizing radiation whereas standard surgical therapies do not; the dose area product per procedure is around 17,400 μGy/m2, or an effective dose of approximately 47 mSv. 29 This is roughly equivalent to an additional lifetime cancer risk of 0.2% (baseline risk for men is 44.9%) in a patient population with an average age of 65. 30
Finally, thus far, results with PAE appear variable and operator dependent, 20 although concerted educational mentored programmes from organizations such as the Cardiovascular and Interventional Society of Europe are attempting to improve the reproducibility of PAE. 7
Complications
Following PAE, Clavien I complications account for over 99% of all adverse events.27,31 Of these, perineal pain, nausea/vomiting and dysuria, resolved by anti-inflammatory therapy and collectively known as ‘post-PAE syndrome’, 4 is most common and is described in approximately 9% of all patients managed with PAE. 27 Furthermore, transient haematuria, haematospermia and minor rectal bleeding have been described in around 3% of patients. 27 Other Clavien I events include uncomplicated urinary tract infections (UTIs) and a low incidence (<1%) of puncture site haematomas. Most authors describe prophylactic antibiotic prescription to limit the incidence of UTI after PAE. 15
Acute urinary retention following PAE has been described in a minority of studies,32 –34 with an incidence ranging from 24.6% to 31.8% of patients in these papers, but most authors do not report the complication. 27 Several authors describe the use of anti-inflammatory medications (such as nonsteroidal anti-inflammatory drugs) to reduce the chance of retention, but no evidence is available to directly support this practice. 15
A single grade 2 complication has been described; UTI requiring hospital admission and intravenous antibiotics. 35 The only Clavien grade 3 complication to date requiring surgical intervention was an episode of focal bladder ischaemia which required localised resection 1 month after PAE. 16 Therefore, PAE compares favourably with TURP in terms of major complications. 30
Initial outcomes and evidence
Multiple noncomparative studies investigating PAE have been conducted internationally, with a total of 13 identified by a recent meta-analysis. 20 A further meta-analysis 27 determined improvements in both subjective and objective parameters. In terms of subjective analysis, a mean improvement in International Prostate Symptom Score (IPSS) of 20.39 has been demonstrated. In terms of objective parameters, mean postvoid residual volume has been shown to reduce by 85.54 ml, maximum flow rate (Qmax) to increase by a mean of 5.4 ml/s and prostate-specific antigen to reduce by a mean of 0.1–5.8 ng/ml, suggesting PAE is a viable technique for treating BPO. Other studies have looked specifically at men who are catheter dependent, with clinical success (successful removal of the catheter) in 87.5%. 38 However, the efficacy of PAE compared with other surgical techniques is less clear, with only three comparative studies performed thus far.5,33,36 Two of these compared PAE with TURP and one compared PAE with open prostatectomy. Both TURP studies suggested equivalent symptomatic benefit between surgery and PAE, although some questions have been raised about the interpretation of outcomes, such as the classification of complications. 37 More high-quality comparative studies are needed if the role of PAE in the management of BPO is to be identified.
Furthermore, no studies to date have compared PAE with medical therapies, or newer techniques for BPO such as holmium laser enucleation of the prostate, photoselective vaporization of the prostate or UroLift. This is particularly important as these techniques share many of PAE’s advantages over TURP, and neglecting direct comparison will impede clinical decision making between PAE and these therapies.
Although long-term success is reported to be favourable, 21 more long-term data are needed. It has been suggested that the variability in success is likely to be secondary to variable operator technique, including catheter choice, particle type and size, and embolization endpoint, as well as patient anatomical factors. 20 No differential outcome in variable embolic agents or particle size has been identified.5,8,21
Cost
With variable techniques and equipment, the cost of PAE will fluctuate between centres and no cost data are yet available in the literature. The cost is composed of procedural aspects, including staff and equipment totalling around $950–1100 (€900–1030). The fee related to the room is around $600 (€560), meaning a combined cost of $1550–1700 (€1450–1600) per procedure. On the other hand, there are other surgical procedures, such as TURP (around $3300/€3100 per procedure), 37 although workup with pre-embolization CT and clinic time adds additional charges. There may be an increased rate of further procedures required following PAE compared with surgery and this should be considered in any cost analysis.
Future research
In addition to multiple further noncomparative studies internationally, several comparative studies have been established. UK-ROPE, a UK registry comparing PAE with surgery, has finished recruiting, with patients followed up over 12 months. 11 In addition, randomized and nonrandomized trials currently in progress will hopefully add clarity to the PAE debate.12,39,40,41 A sham study is also currently enrolling patients who will be randomized to PAE or a sham procedure, with those participants not receiving the true procedure offered PAE after 6 months. 42
Further considerations
All current trials have been performed in specialist centres by experienced operators. As PAE becomes a more widespread technique and available to less experienced practitioners, there is the potential for clinical efficacy rates to fall, and complication rates to rise, with more frequent nontarget embolization events as a possibility. Addressing this through improved education of potential PAE practitioners is an important step. 15 Alternatively, establishing a tertiary referral system to specialist centres may ensure optimal outcomes for patients.
Although some factors predictive of a good symptomatic outcome have been ascertained, more must be done to identify those patients who will benefit maximally.25,43 As more studies emerge, analysis to evaluate favourable patient variables is essential to further our understanding of which patients to target with PAE.
Finally, modification of the basic PAE technique has already elicited promising outcomes, with the PErFecTED (proximal embolization first, then embolize distal) system demonstrating significantly improved symptomatic outcomes compared with the old technique. Continued developments such as this will aid the emergence of PAE as a leading treatment for BPO.
Conclusion
PAE approaches BPO from an entirely different perspective to traditional surgical techniques and therefore brings with it a unique set of advantages and solutions. Initial evidence suggests PAE certainly has a role to play in the management of BPO, but its role is still evolving. With the expected arrival of more comparative and randomized trials, the role of PAE in the urologists’ toolkit will hopefully emerge, much to the benefit of patients with BPO.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.