
Abstract
Objectives:
New targets and approaches are under investigation for the treatment of nonmuscle invasive bladder cancer (NMIBC). Preclinical data suggest cyclooxygenase-2 (COX-2) as a promising target. Celecoxib, a COX-2 selective inhibitor, inhibits tumor development and enhances survival, both in vitro and in vivo models of bladder cancer. Therefore, we conducted a pilot study of celecoxib to prevent recurrence in patients with intermediate risk NMIBC.
Methods:
Treatment with celecoxib was administered orally for 12 months and compared with a contemporary series of patients treated with intravesical mitomycin C (MMC), given weekly for 4 weeks and then monthly for 11 months. Primary endpoints were time to first recurrence and adverse events.
Results:
From 2003 through 2006, 58 patients were treated with celecoxib and compared with 66 patients receiving MMC. After a median follow up of 75 months, 49 patients were disease free, including 23 (34.85%) in the MMC group and 26 (44.8%) in the celecoxib group. Median disease-free interval was 67 months [95% confidence interval (CI) 35.8 to NA] versus 41 months (95% CI 27.1–67.1; log-rank p = 0.25) for patients treated with MMC and celecoxib, respectively. In the multivariate analysis, treatment was not found to be an independent predictor for recurrence [hazard ratio (HR) 0.76, 95% CI 0.47–1.22, p = 0.25). Overall, 45 AEs were recorded in 35/124 patients. There were no differences between the two groups.
Conclusions:
Our data support a clinical benefit of celecoxib and encourage future trials in which COX-2 inhibitors may be tested in selected patients with NMIBC.
ClinicalTrials.gov identifier: NCT02343614.
Introduction
Treatment options for nonmuscle invasive bladder cancer (NMIBC) are limited. Initial management involves transurethral resection of the bladder tumor (TURBT), with or without adjuvant intravesical instillations of chemotherapy or immunotherapy [Witjes and Hendricksen, 2008]. Commonly used current intravesical therapies include mitomycin C (MMC) and bacillus Calmette–Guérin (BCG). Both of these therapies were introduced several decades ago and have been shown to reduce recurrence rates in intermediate and high risk NMIBC compared with TURBT alone [Witjes and Hendricksen, 2008; Sylvester et al. 2008; Shelley et al. 2001]. Nevertheless, after a median follow up time longer than 5 years, more than 50% of the patients treated either with adjuvant BCG or MMC will recur [Serretta et al. 2004; Oddens et al. 2013]. Furthermore, all available intravesical treatment options have associated toxicities that can impair patient compliance, particularly so for BCG, which routinely causes irritative voiding symptoms, and often causes fever and malaise [Koya et al. 2006; Kilbridge et al. 1994; Colombel et al. 2006]. Thus, new targets and new approaches are under investigation for preventing bladder cancer recurrence at the cost of a lower morbidity [Kamat et al. 2013]. Chemoprevention is one such attractive approach [Busby and Kamat, 2006].
Epidemiological and preclinical evidence suggest that cyclooxygenase-2 (COX-2) plays an important role in urothelial carcinogenesis and is a promising target for bladder cancer. In humans, COX-2 expression in the urothelium is associated with high tumor grade and stage, and is an independent predictor of disease progression and survival [Miyata et al. 2005; Shariat et al. 2003; Ristimäki et al. 2001]. In a rodent urinary bladder model, COX-2 overexpression induces bladder tumorigenesis throughout premalignant hyperproliferation and further transformation; such a process is prevented by the use of COX-2 inhibitors [Klein et al. 2005]. Likewise, celecoxib effectively inhibits development and tumor growth, and enhances survival in a murine model of nitrosamine-induced bladder cancer [Grubbs et al. 2000].
These studies support the development of clinical trials to determine whether COX-2 inhibitors can provide a therapeutic utility for bladder cancer patients. Therefore, we conducted a pilot study of celecoxib to prevent recurrence in patients with intermediate risk (IR) NMIBC after treatment with transurethral resection (TUR).
Patients and methods
Study design
This is a pilot study of celecoxib in patients with IR NMIBC. By definition, IR NMIBC consisted of a heterogeneous group of patients ranging from those with a solitary but recurrent low grade Ta tumor, to those with multiple, recurrent, G1-2 Ta tumors. Treatment with celecoxib was offered to eligible subjects as an alternative to intravesical MMC. Eligibility criteria included complete TUR of any visible bladder tumor and histological confirmation of IR NMIBC. At time of study entry, all subjects were 18 years or older, had a Karnofsky Performance Score ⩾60%, adequate hematologic, liver and renal function, and an imaging study excluding upper urinary tract urothelial cancer (UC). Patients with bladder carcinoma in situ (CIS), any T1 or G3 disease, patients not receiving a single MMC instillation after TURBT, patients receiving cardioprotective doses (⩽100 mg daily) of aspirin, as well as frequent users of full dose nonsteroidal anti-inflammatory drugs (NSAIDs), subjects with a history of coagulation disorder, gastrointestinal disease (such as peptic ulcer or inflammatory diseases) or intestinal bleeding, and patients receiving concomitant investigational medications were all excluded from enrollment. Subjects with a history of myocardial infarction (MI) in the 12 months prior to accrual were non eligible. Furthermore, patients that had MI prior to this period had to document baseline cardiac function within normal limits, with echocardiography. As warnings were published documenting the cardiovascular side effects from COX-2 inhibitors, accrual was interrupted from 22 December 2004 to 1 March 2005. According to an amended protocol, additional criteria excluded from enrollment any patient with a history of cardio- and/or cerebrovascular disease. Furthermore, at study entry, all patients had to document a normal cardiac function and a normal echocardiography.
As a standard practice in our department, a single intravesical instillation of MMC was administered within 12 hours from TURBT. Treatment with celecoxib was started within 4 weeks from TURBT, as histology was obtained. Celecoxib was provided for free by Pharmacia Upjohn. Celecoxib (200 mg) was taken orally, twice a day, for a total daily dose of 800 mg and continued for 12 months, or until documentation of recurrence. Treatment was discontinued for unacceptable or serious adverse event (SAE), or subordinate to patient’s request. For eligible patients, clinical evaluations were performed at baseline and the day of any cystoscopic examination: every 3 months for the first 2 years, every 6 months the third year, and yearly thereafter. Clinical evaluations included a focused history, including smoking habit, physical exam, standard blood tests, urinalysis, bladder cytology, cystoscopic examination and compliance measurement (capsule count). For adverse event (AE) assessment, a case-report form was filed for each contact.
All cases of recurrent NMIBC at cystoscopy underwent histological verification. Whenever indicated, alternative treatment options, including radical cystectomy, were discussed and eventually offered to patients.
Control arm
A control arm including patients treated with TURBT and adjuvant MMC was generated retrospectively for comparison and consisted of a consecutive series of patients with IR NMIBC treated during the same period of time. Eligibility criteria included complete TUR of any visible bladder tumor and histological confirmation of bladder UC. At time of study entry, all subjects were 18 years or older. Patients with histological evidence of bladder CIS, any T1 or G3 disease, patients not receiving a single MMC intravesical instillation after TURBT and patients with an upper urinary tract imaging suspicious for UC at the time of TUR were excluded from enrollment. Adjuvant MMC was administered as an intravesical instillation of 40 mg dissolved in 50 ml saline. Therapy was started within 5 weeks after TURBT. Treatments were given weekly for 4 weeks and then monthly for 11 months. Clinical evaluations were performed as for patients receiving celecoxib.
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All patients provided written informed consent and the study was approved by the University of Bari Institutional Review Board (proposal No. 2401/2002).
Database and statistical analysis
Data were collected prospectively into a database, including preoperative clinical and biological characteristics, patient demographics, surgical data and postoperative parameters. Patient’s baseline characteristics according to treatment group were reported as frequency (percentage) or median interquartile range (IQR) and were compared with Pearson’s χ2 test or Mann–Whitney test for categorical and continuous variables, respectively. Due to the loss of seven subjects to follow up prior to the second visit, a ‘per protocol’ analysis was performed. Time to first recurrence was the primary outcome defined as the length of time from surgery to the first bladder recurrence or until last follow up (if the patient had not experienced a clinical recurrence). Kaplan–Meier method and log-rank test statistics were used to compare probabilities of recurrence-free survival in the two treatment groups. Relative risks of recurrence were calculated by univariate and multivariate Cox proportional hazards model adjusting for the effects of other covariates known to be of prognostic importance such as age, tumor stage and grade, smoking history, tumor size and number of tumors. Subgroup analysis was conducted to evaluate treatment effect in patients treated for at least 6 and 9 months. Results are expressed as hazard ratios (HRs) with their 95% confidence intervals (CIs). Finally, toxicities grade and frequency, as well as mortality data were reported according to treatment group. All the analyses were performed using SAS Statistical Package Release 9.2 (SAS Institute, Cary, NC). A p value <0.05 was considered as being statistically significant.
Results
Patient characteristics
Between January 2003 and June 2006, 192 patients underwent TUR at our department with histologic evidence of IR NMIBC; among those, 65 patients were eligible and willing to receive celecoxib. Major causes for exclusion were use of cardioprotective or full dose aspirin and/or MI history (44 patients), history of gastrointestinal disease (18 patients), inadequate performance status (seven patients) and other causes (10 patients), while 48 eligible patients chose other treatment options. Of the 65 patients, 58 were finally analysed, since seven were lost to follow up (Figure 1). During the same period of time, a consecutive cohort of 78 patients received intravesical MMC. Of those, 66 were finally evaluated, since 12 were excluded either for nonadherence to treatment schedule (nine patients) or because lost to follow up (three patients). Patient’s characteristics and differences according to treatment are described in Table 1.

Flow diagram of the cohort of patients treated with celecoxib.
Baseline characteristics and association with treatment.

IQR, interquartile range.
Recurrence
After a median follow up of more than 6 years (75 months, range 61–90), 49 patients were disease-free, including 23 (34.85%) in the MMC group and 26 (44.8%) in the celecoxib group. Thus, patients assigned to celecoxib or to MMC had a comparable median disease-free interval (67 months; 95% CI 35.8 to NA) versus 41 months (95% CI 27.1–67.1); log-rank p = 0.25). In Figure 2, a Kaplan–Meyer curve describes the probability of remaining recurrence-free for the two cohorts. After 18 months, of the 94 recurrence-free patients, 43 (74.1%) were in the celecoxib group and 51 (77.3%) were in the MMC group. At 60 months, although there was a trend in favor of celecoxib treated patients, the two curves were statistically comparable; thus, 52 patients remained recurrence-free – 27 (46.6%) in celecoxib group and 25 (37.9%) in the MMC group.

Kaplan–Meyer curve describing the recurrence-free survival for patients treated with celecoxib or mitomycin C.
In the Cox univariate regression analysis, a lower recurrence risk for patients treated with celecoxib compared with MMC was found (HR 0.76, 95% CI 0.48–1.21, p = 0.25]. However, a multivariate analysis was performed to assess risk factors associated with recurrence, which comprised treatment, age, tumor size and number, smoke habit, and tumor stage and grade. Only number of lesions and smoke habit were found to be independent predictors for recurrence, while treatment was not (HR 0.76, 95% CI 0.47–1.22, p = 0.25). Data are shown in Table 2. A subgroup analysis, performed to test for differences among patients treated for at least 6 or 9 months, shows a nonsignificant advantage for patients receiving celecoxib (Table 3).
Univariate and multivariate analysis of time to first recurrence.

CI, confidence interval; HR, hazard ratio.
Subgroup analysis of time to first recurrence.

Data adjusted for: smoking habit, number of tumors, tumor size, tumor age and tumor stage.
Toxicity
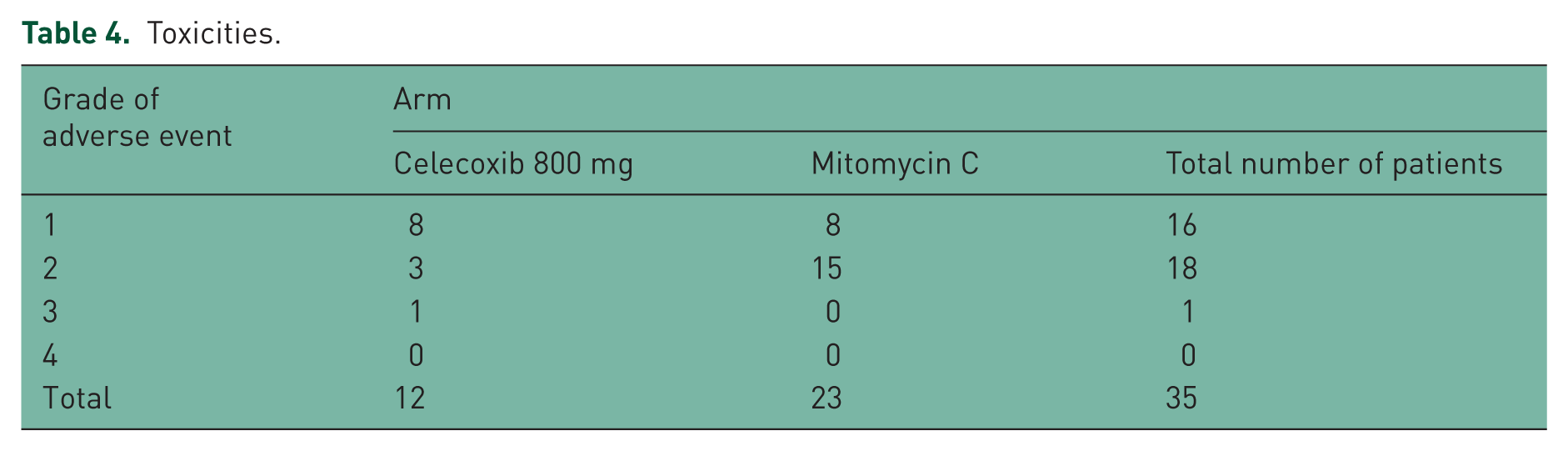
Overall, 45 AEs were recorded in 35/124 (28.2%) patients who entered the study (Table 4). Among those, 12/58 (20.6%) were in the celecoxib cohort, while 23/66 (34.8%) received MMC (p = 0.21). The most commonly reported AEs were: bladder pain in 10 cases; dysuria, arterial hypertension and skin erythema in four cases; localized peripheral edema in three cases; and fever, stress urinary incontinence, macroscopic hematuria, malaise, itchiness and skin rashes in two cases. One patient treated with celecoxib reported after treatment completion a grade 3 event, specifically angina. In this case a correlation to study medication could not be excluded.
Toxicities.
Although no deaths occurred during study medication, a total of 15/124 (12.1%) patients died after drug discontinuation, during follow up. Among those, 6/58 (10.3%) patients were treated with celecoxib, while 9/66 (13.6%) received MMC. Five deaths were caused by progressive bladder cancer, while one patient died during adjuvant chemotherapy. The remaining deaths were neither related to cancer nor attributed to study medications.
Discussion
Several preclinical and translational studies have shown the importance of COX-2 in human bladder cancer growth and aggressiveness, supporting the rationale to test specific COX-2 inhibitors in the clinical setting [Miyata et al. 2005; Shariat et al. 2003; Ristimäki et al. 2001; Klein et al. 2005; Grubbs et al. 2000]. The present study is the first to report the effects of celecoxib given at a daily dose of 800 mg in a population of patients with NMIBC. After TUR, celecoxib was given orally for 1 year and compared with a contemporary population of patients treated with intravesical MMC. After a median follow up of 6 years, median time to first recurrence was 67 months in patients treated with celecoxib compared with 41 months in those receiving MMC. Although statistical significance was not reached, probably related to sample size, these results encourage further examination of celecoxib as an alternative to MMC in NMIBC.
Long-term data from the literature are difficult to compare because of a great heterogeneity between studies in terms of treatment schedule, MMC dosage and patients characteristics. In a prospective randomized study comparing intravesical BCG versus MMC, the 5 years recurrence-free survival in G2 patients, without CIS, was 0.44 and 0.33, respectively [Malmström et al. 1999]. In a meta-analysis of seven EORTC randomized controlled trials of patients with NMIBC, a scoring system was developed to predict the risk for recurrence and progression [Sylvester et al. 2006]. Accordingly, patients with a score between 1 and 9 were considered at IR for recurrence and showed a 5-year recurrence probability of 46–62% [van Rhijn et al. 2009]. Interestingly, 78% of the whole population enrolled in the meta-analysis received intravesical therapy, including MMC. These data are consistent with the results of our study. In fact, we observed a 5 years recurrence rate of 55% and 64% in patients treated with celecoxib and MMC, respectively. Although our results show a trend in favor of celecoxib treated patients, a statistically significant difference was not reached, most likely because of small sample size.
More recently, the results of a placebo-controlled trial of celecoxib [200 mg twice daily (bid)] to prevent bladder cancer recurrence following TUR were presented, supporting a beneficial effect of celecoxib in the treatment of NMIBC [Sabichi et al. 2011]. Compared with this trial, our study is different for several reasons, including daily dose of celecoxib (800 mg versus 400 mg), treatment design/schedule (no adjuvant BCG versus adjuvant BCG prior to celecoxib), and finally the trial by Sabichi and colleagues was placebo controlled. Nonetheless, the observation in our study that celecoxib may be as active or more active than MMC leads to the hypothesis that a higher dose of celecoxib may be more beneficial in patients with NMIBC.
A daily dose of 800 mg (400 mg bid) of celecoxib was chosen for the present study, based on the efficacy observed in randomized trials on bowel polyposis published at the time of study design [Steinbach et al. 2000; Phillips et al. 2002]. Steinbach and colleagues demonstrated that 6 months of daily 800 mg of celecoxib led to a significant reduction in the number of colorectal polyps compared with patients receiving a lower dose of celecoxib or placebo [Steinbach et al. 2000]. A dose response was also shown in the Familial Adenomatous Polyposis (FAP) study with a significant reduction of duodenal polyp burden observed only in the higher dose group (400 mg bid) compared with a lower dose group (100 mg bid) and to placebo [Phillips et al. 2002]. Later trials have confirmed higher doses of celecoxib being more effective in reducing recurrence from colorectal adenomas [Bertagnolli et al. 2006; Arber et al. 2006].
A direct consequence of dose escalation may be the rise in drug toxicity. Although limited by a small sample size, safety analyses did not show an increased overall toxicity in patients receiving celecoxib (p = 0.21). However, one cardiovascular event was registered in the celecoxib cohort, after drug discontinuation (angina); importantly, this patient did not have a history of cardiovascular events at baseline. Indeed, safety data from large randomized trials have raised important concerns regarding the cardiovascular toxicity of celecoxib as well as other COX-2 selective inhibitors [Bombardier et al. 2000; Solomon et al. 2005]. Although celecoxib may increase this risk of cardiovascular events also in healthy subjects, the strongest influence was found to be in subjects with a baseline condition of atherosclerotic heart disease; it was found to be dose-related, being higher in patients receiving daily 800 mg compared with lower doses.
One measure to face toxicity could be the identification of a population of best responders in order to maximize the benefit. Recently, we have made an attempt to assess the response profile of several bladder cancer cell lines to celecoxib and MMC, alone and in co-administration [Pagliarulo et al. 2013]. We found that COX-2 overexpressing cells resembled a more aggressive phenotype with upregulation of breast cancer resistance protein (BCRP), one of the membrane transporters involved in multidrug resistance. Interestingly, when MMC was administered alone, these cells became resistant to MMC killing; however, pretreatment with celecoxib caused an increase in intracellular concentration of MMC with a significant and dose-dependent increase in MMC cytotoxic activity. In cells lacking COX-2 expression (TCCsup, UMUC3 and 5637si-CX), celecoxib was unable to affect MMC killing. Furthermore, in an orthotopic murine model of urothelial carcinoma, celecoxib was shown to improve the effectiveness of intravesical BCG. When compared with intravesical BCG alone and with untreated controls, the combination with celecoxib resulted in increased tumor infiltration of CD4+ T cells and in a significant reduction of tumor burden in a dose-dependent manner [Dovedi et al. 2008]. These findings suggest that patients overexpressing COX-2 may be appropriate subjects to involve in future trials of NMIBC in combination with standard of care. An ultimate support to the role of celecoxib may come from the results of an ongoing phase III randomized controlled trial (BOXIT) conducted in the UK in patients with IR and high risk NMIBC receiving celecoxib 400 mg versus placebo.
This study is subject to limitations, particularly the nonrandomized comparison with a cohort of patients treated with MMC. Although, data from these patients were prospectively inserted in a database created for the management and follow up of patients with NMIBC, the study is subject to a risk of selection and information bias. In addition, sample size was too small to provide significant statistical power to the study. Accrual was strongly affected by the release of information regarding the cardiovascular toxicity of celecoxib; although the protocol was amended in 2005 and new exclusion criteria added, few additional patients were enrolled in the study.
In conclusion, our data are limited to support any change in the contemporary treatment of NMIBC. However, they encourage future trials in which COX-2 inhibitors may be tested either as a standalone therapy in selected patients or as a combination therapy to improve the effectiveness of drugs with a well-known activity on NMIBC. Two conditions yet need to be addressed in order to appropriately utilize COX-2 inhibitors in the future; first is the development of measures to predict and eventually protect from the risk of cardiovascular events, and second is the definition of tools to predict best responders.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.