
Abstract
Prostate cancer is the second leading cause of cancer death in men and there is an urgent clinical need to improve its detection and treatment. The introduction of prostate-specific antigen (PSA) as a biomarker for prostate cancer several decades ago represented an important step forward in our ability to diagnose this disease and offers the potential for earlier and more effective treatment. PSA measurements are now routinely conducted alongside digital rectal examination, with raised PSA levels leading to biopsy. PSA is also used to monitor disease and assess therapeutic response. However, there are some important limitations to its use, not least its lack of specificity for prostate cancer, and increased PSA screening may have resulted in overdiagnosis and overtreatment of early, low-risk prostate cancer. Therefore, there is a need for more specific and sensitive biomarkers for the diagnosis and monitoring of prostate cancer and treatment response; in particular, biomarkers of response to hormonal treatments in prostate cancer and predictive biomarkers to identify who is most likely to respond to these treatments. Here we review the current utilization of PSA and data on potentially more specific and sensitive biomarkers for the diagnosis and monitoring of prostate cancer: prostate cancer antigen 3 (PCA3) and the TMPRSS2-ERG fusion gene. A description of the design of an ongoing study of the 6-month extended release formulation of leuprorelin acetate (Eligard® 45 mg) will provide preliminary data on the potential utility of these new biomarkers for detecting therapeutic response after hormonal therapy.
Introduction: the need for biomarkers in prostate cancer
Prostate cancer is one of the most common epithelial tumour types and the second leading cause of cancer death in men in the USA [Jemal et al. 2009]. Prostate-specific antigen (PSA), a serine protease secreted by epithelial cells of the prostate, is the most widely used tumour biomarker for early detection of prostate cancer [Shariat et al. 2011]. Since the first measurement of PSA in the blood more than 30 years ago [Rao et al. 2008], diagnosis and management of prostate cancer has been increasingly reliant upon PSA monitoring. In addition, PSA progression (defined as an increase of ≥25% above the nadir and an absolute increase of ≥2 or 5 ng/ml) may be used to predict overall survival in metastatic prostate cancer [Hussain et al. 2009].
However, PSA is prostate-specific but not cancer-specific and therefore its use has several limitations. PSA is elevated in noncancerous conditions such as benign prostatic hyperplasia (BPH) and prostatitis [Bickers and Aukim-Hastie, 2009], and certain subgroups of prostate cancer do not produce PSA [Shariat et al. 2011]. There is also a lack of correlation between PSA and tumour grading and staging [Bickers and Aukim-Hastie, 2009]. Therefore, there is a clinical need for more specific and sensitive tumour markers to assist clinicians in the management of prostate cancer. More specifically, given the wealth of tumour biomarkers recently described in the literature (see reviews by Shariat and colleagues [Shariat et al. 2011] and Bickers and Aukim-Hastie [Bickers and Aukim-Hastie, 2009]), there is a need for validation of these biomarkers in specific patient populations being treated with particular therapies and to identify predictive biomarkers that may indicate which patients will respond best to given treatment strategies.
The National Cancer Institute’s dictionary of cancer terms defines a biomarker as a ‘biological molecule found in blood, other body fluids, or tissues that is a sign of a normal or abnormal process or of a condition or disease’ [National Cancer Institute, 2013]. Table 1 lists the different ways in which biomarkers can be used at different stages of the disease pathway [Shariat et al. 2011]. Prostate cancer antigen 3 (PCA3) and the fusion transcript of transmembrane protease serine 2 (TMPRSS) and v-ets erythroblastosis virus E26 oncogene (ERG), TMPRSS2-ERG, are two prostate cancer specific molecular biomarkers that have demonstrated diagnostic utility in urine specimens [Groskopf et al. 2006; Hessels et al. 2007], and may have value as biomarkers of treatment response.
The uses of prostate cancer biomarkers.
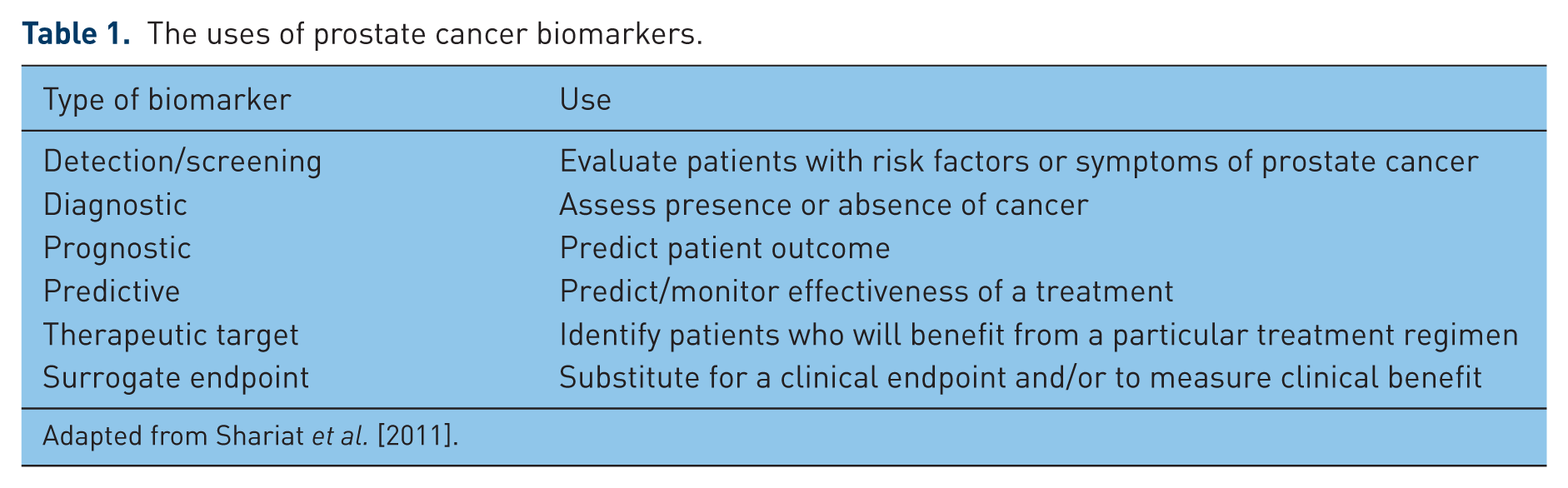
Adapted from Shariat et al. [2011].
This paper reviews the literature on prostate cancer biomarkers, including serum/blood markers [PSA, PSA-messenger RNA (mRNA), PCA3-mRNA and TMPRSS2-ERG-mRNA] and urine markers (PCA3). The ongoing EFFECT trial is described as an example of the type of trial required to validate such biomarkers. This is a phase IV exploratory study designed to assess the effect of a 6-month extended release formulation of leuprorelin acetate (Eligard® 45 mg, Astellas Pharma Europe Ltd) on the above-mentioned biomarkers in patients with metastatic prostate cancer over a 24-week period.
How this review was conducted
An English language literature review of published data on biomarkers and prostate cancer in the MEDLINE database (1990 to February 2012) was undertaken. The keywords used were prostate cancer, urine, blood, diagnostic and prognostic biomarkers, PSA, PSA-mRNA, PCA3, PCA3-mRNA and TMPRSS2-ERG-mRNA. The resulting literature was reviewed for the latest data on each of the biomarkers and their role in diagnosis and/or monitoring treatment response or disease progression.
The role of PSA in prostate cancer
PSA is an androgen-regulated gene product that is normally secreted into the lumen of the prostate gland. However, in cancerous situations, serum PSA levels rise [Agoulnik and Weigel, 2006]. In post-therapy follow up, total PSA change is easily assessable, quantitative, reproducible and inexpensive to monitor. PSA levels are also effective indicators of response to non androgen-based therapies, e.g. chemotherapy, cytotoxic therapy and radiation therapy [Lee et al. 2012]. Initial studies found that a confirmed PSA decline of ≥50% following chemotherapy was highly prognostic [Bubley et al. 1999], while in phase III clinical trials, PSA decline was found to be a potential surrogate marker for overall survival [Armstrong et al. 2007; Petrylak et al. 2006]. PSA doubling time (PSADT) has been identified as a powerful independent prognostic factor of nonmetastatic prostate cancer aggressiveness [Smith et al. 2005, 2011; Tombal, 2012].
Although PSA measurement has been highly effective in increasing detection rates of early prostate cancer, screening for prostate cancer by PSA measurement has also exposed patients to possible overtreatment of cancers that might never have become clinically significant [Shariat et al. 2011]. The latest guidelines for the treatment of prostate cancer from the National Comprehensive Cancer Network express concern over this problem [National Comprehensive Cancer Network, 2012], but there is uncertainty over how it should be addressed [The Lancet, 2012].
The measurement of total serum PSA levels as a marker of prostate cancer has several limitations [Shariat et al. 2011]. Although elevated PSA levels can certainly be indicative of cancer, they are not specific for cancer and levels may be elevated for other reasons (e.g. BPH). In addition to the lack of specificity, there is a large degree of intra- and inter-patient variability in PSA levels, which results from differences in analytical technique (e.g. different laboratories, assays or protocols) and biological variation. There has also been some controversy over what level of total PSA should be considered indicative of prostate cancer. Early studies reported values for the upper limit of normal from as low as 2.6 ng/ml [Kuriyama et al. 1980], while a later study used 7.5 ng/ml as the cutoff value [Kuriyama et al. 1982]. An analysis of the Prostate Cancer Prevention Trial investigated the prevalence of prostate cancer at PSA levels ≤4.0 ng/ml in men receiving placebo treatment [Thompson et al. 2004]. Among 2950 men (aged 62–91 years) with ‘normal’ PSA levels (≤4.0 ng/ml) and normal digital rectal examination (DRE) who underwent a prostate biopsy at the end of the study, prostate cancer was detected in 15.2%: a larger proportion than would be expected in a group where all indicators were normal [Thompson et al. 2004]. There was a positive association between total PSA level and prevalence of prostate cancer, with the prevalence of high-grade cancer reaching 25.0% for PSA levels of 3.1–4.0 ng/ml. However, there is no evidence that reducing the PSA threshold to below 4 ng/mL will improve long-term survival in men with prostate cancer, and these data may simply emphasize that the specificity and sensitivity of total PSA for diagnosing prostate cancer is imperfect. Indeed, treatment monitoring is the most accepted clinical application for total PSA [Shariat et al. 2011].
PSA monitoring may not be useful in all aspects of the prostate cancer disease spectrum [Armstrong et al. 2012]. For example, sipuleucel-T was shown to improve overall survival without affecting early PSA levels [Kantoff et al. 2010]. PSA measurement has not been validated with many novel agents and the threshold of response is not clear. The PSA response is not entirely consistent: PSA can rise or ‘flare up’ in a minority of patients after therapy has been initiated.
Alternative techniques to enhance the diagnostic accuracy of PSA
Enhancing the diagnostic accuracy of total PSA, particularly specificity, is critical, not least because a greater specificity would reduce the number of (unnecessary) biopsies performed. With this aim, several derivatives of PSA have been investigated, including age-specific total PSA cutoffs, total PSA density, total PSA density of the transition zone, total PSA velocity and alternative molecular forms of PSA [Schröder et al. 2008; Shariat et al. 2008].
The age-specific PSA reference range is based upon the fact that PSA levels tend to increase with age; however, there is concern that their use may delay diagnosis [National Cancer Institute, 2012]. The PSA density of the transition zone is defined as the blood level of PSA divided by the volume of the prostate transition zone (the interior part of the prostate that surrounds the urethra) [National Cancer Institute, 2012]. A low PSA density is generally inferred to reflect a low risk of having prostate cancer [National Comprehensive Cancer Network, 2012]. PSA velocity refers to the serial evaluation of serum total PSA concentration over time (generally expressed as ng/ml per year), and the PSADT describes the time over which a man’s PSA level doubles. Smith and colleagues found that 40% of the men with prostate cancer and a rising PSA after radical prostatectomy and/or radiation therapy who were treated with celecoxib, a selective cyclooxygenase-2 inhibitor, had post-treatment PSADTs ≥200% of baseline values [Smith et al. 2006]. Available data suggest that PSA velocity has limited value in prostate cancer screening and prognostication due to its poor sensitivity, imprecision due to biological and analytical intra-individual variability, and poor predictive accuracy in relation to prostate cancer detection [Shariat et al. 2011; Vickers et al. 2011].
Finally, different PSA isoforms can be measured such as free PSA and bound PSA (complexed to α2-macroglobulin, α1-protease inhibitor or α1-antichymotrypsin) [Shariat et al. 2011]. The predictive value of percentage-free PSA was examined in a multicentre, prospective trial in 773 men with either prostate cancer or benign prostatic disease, and total PSA levels between 4.0 and 10.0 ng/ml [Catalona et al. 1998]. The study showed that the percentage-free PSA was an independent predictor of prostate cancer (odds ratio 3.2; 95% confidence interval 2.5–4.1; p < 0.001) and was significantly more predictive than age or total PSA level. Furthermore, a recent retrospective study of 76 patients with biochemical PSA recurrence following radical prostatectomy found that [-2]pro-prostate-specific antigen, a proform of PSA, was a statistically significant predictor of imaging-proven metastatic prostate cancer [Sottile et al. 2012]. Further investigation of all of these PSA derivatives will be of great interest.
In terms of non-PSA biomarkers for prostate cancer, several markers with clinical promise, including PCA3 and TMPRSS2-ERG fusion gene, are being actively investigated [Salagierski and Schalken, 2012]. Conversely, a number of proteins, coding genes and tissue markers that were previously proposed as potential prostate cancer markers have not been adopted into clinical practice. These include microRNAs (miRNAs) and tissue markers such as ki-67, PTEN, E-cadherin and EZH2. Factors contributing to the lack of uptake of these techniques in the clinical setting include: (i) inconsistent patterns when used in screening, in the case of miRNAs, where patterns of both upregulation and downregulation of miRNAs have been found in tumour tissue when compared with normal tissues [Lu et al. 2005; Volinia et al. 2006]; and (ii) poor predictive utility for disease progression, e.g. ki-67 and E-cadherin [McLoughlin et al. 1993; Ruijter et al. 1998; Stapleton et al. 1998; Brewster et al. 1999].
An emerging diagnostic role for PCA3
Another potentially important biomarker for prostate cancer is PCA3 (differential display clone 3), a noncoding RNA gene that is only expressed in human prostate tissue and is highly overexpressed in prostate cancer. PCA3 mRNA is measured in urine sediment and several commercial assays for this are available [Sardana et al. 2008]. PCA3 is largely undetectable in other tissues such as bladder and testis [Hessels et al. 2003; Schalken et al. 2003]. Overexpression of PCA3 mRNA has been detected in 95% of prostate cancers tested, with a median 66-fold upregulation versus adjacent noncancerous prostate tissue [Hessels et al. 2003]. This higher specificity of PCA3 is likely to represent the major advantage over PSA testing.
The PCA3 test is approved by the US Food and Drug Administration (FDA) and commercially available (Progensa® PCA3, Gen-Probe, San Diego, CA) to help physicians determine the need for repeat prostate biopsies in men who have had a previous negative biopsy [Groskopf et al. 2006; US Food and Drug Administration, 2012]. The test quantitatively detects the expression of PCA3 mRNA in urine after DRE using transcription-mediated amplification and the PCA3 score is subsequently calculated as PCA3 mRNA / PSA mRNA × 1000. Several studies have shown the superiority of PCA3 score to serum PSA level in predicting biopsy outcome [Roobol et al. 2011]. A European, prospective, multicentre study of 516 men with total PSA levels of 2.5–10 ng/ml reported a higher mean PCA3 score in men with a positive versus a negative biopsy outcome (69.6 versus 31.0; p < 0.0001); this score was independent of age, total PSA level and prostate volume [de la Taille et al. 2011]. The PCA3 score (cutoff of 35) had a sensitivity of 64% and specificity of 76%.
To date, there are few data on whether PCA3 has utility as a marker of treatment response [Auprich et al. 2011]. For example, in a pilot study of nine patients with localized prostate cancer, the effect of dutasteride, a dual 5α-reductase inhibitor, on PCA3 score was variable [van Gils et al. 2009]. It appears likely that the value of PCA3 in diagnosis and prognosis may yet be further improved by combining it with other new biomarkers such as TMPRSS-ERG fusion transcripts [Auprich et al. 2011; Cornu et al. 2013; Leyten et al. 2014].
TMPRSS2-ERG fusion gene
Rearrangement of genes is frequently seen in cancer. The most common fusion in prostate cancer is between the androgen-regulated TMPRSS2 gene transcriptional promoter and the oncogene ERG. This fusion results in an androgen-regulated TMPRSS2-ERG fusion gene. Similarly to the PCA3 gene, TMPRSS2-ERG rearrangement can be detected in urine after DRE and thus used to assist with diagnosis of prostate cancer [Laxman et al. 2006; Hessels et al. 2007]. The detection of TMPRSS2-ERG gene fusion in urine has over 90% specificity and 94% positive predictive value for the presence of prostate cancer [Hessels et al. 2007].
TMPRSS2-ERG gene fusions have been associated with aggressive prostate cancer in a transgenic mouse model, detected in distant metastases and also linked with aggressive prostate cancer phenotypes in humans [Mosquera et al. 2009; Barwick et al. 2010]. Combining the PCA3 test and the TMPRSS2-ERG fusion test is a potential way to improve diagnostic accuracy. Hessels and colleagues analysed the urinary sediments of 108 men for the presence of both PCA3 and TMPRSS2-ERG products and showed that, by combining the two assays, the sensitivity of prostate cancer detection increased from 63% for PCA3 alone to 73% for both tests without compromising the specificity [Hessels et al. 2007]. In a more recent study, expression levels of PCA3 and TMPRSS2-ERG were examined in tissue samples from BPH, normal prostate adjacent to prostate cancer and prostate cancer [Robert et al. 2013]. Of seven PCA3 false negatives, four were corrected by TMPRSS2-ERG testing, and a cutoff had to be defined to avoid eight false positives. These findings support a higher sensitivity for prostate cancer diagnosis when the two markers are combined.
To date, there are few data on whether TMPRSS2-ERG has utility as a marker of treatment response. In a small study of 21 chemotherapy-naïve men with castration-resistant prostate cancer (CRPC), it was investigated whether harbouring the androgen-dependent TMPRSS2-ERG fusion gene could indicate dependence on androgen receptor signalling and define a tumour subgroup of CRPC patients with a higher response rate to abiraterone acetate [Attard et al. 2008]. The PSA decline rate appeared to be higher in patients with an ERG rearrangement. A recent meta-analysis concluded that TMPRSS2-ERG, according to currently available evidence, was best suited as a diagnostic tool [Pettersson et al. 2012]. The analysis included 1052 men treated with radical prostatectomy and showed that TMPRSS2-ERG was associated with tumour stage at diagnosis, but was not associated with biochemical recurrence or mortality [Pettersson et al. 2012].
The lack of agreement between these cited studies indicates that there is insufficient evidence regarding the prognostic value of TMPRSS2-ERG, highlighting the need for more studies in this area; specifically, studies using overall survival as the primary endpoint. This said, there is general consensus among studies for a strong association between TMPRSS2-ERG and tumour stage. However, the role of TMPRSS2-ERG as a marker for treatment response or prostate cancer progression is yet to be confirmed.
Rationale and design of the EFFECT trial
To optimize patient treatment strategy and healthcare costs in the field of prostate cancer, there is a need for advancements in relation to disease diagnosis, management, indicators of treatment response and tools for predicting treatment success. More specific prostate cancer biomarkers will permit these sought-after medical advancements. Furthermore, biomarker improvements are important, particularly for metastatic patients, as there can be a disconnect between radiographic progression observed on imaging and PSA levels. Serum PSA is currently the only biomarker used to measure disease burden; however, its surrogacy for survival and prediction accuracy for treatment response is not sufficient. Due to heterogeneity in metastatic lesions, one may be progressing while another is regressing. Therefore, it is paramount to identify at the early stages of the disease (even before radiographic progression) which biomarkers are non-normal, so that targeted treatment can be provided.
Many ongoing clinical trials are investigating how new and established prostate cancer therapies impact on novel and experimental biomarkers. There is a reasonable body of evidence on the utility of biomarkers in diagnosis, but their role in monitoring disease progression and assessing treatment response is often less clearly defined. Recently, authors have stated that there is a need for validation of these biomarkers in certain patient populations being treated with specific therapies (see reviews by Shariat and colleagues [Shariat et al. 2011] and Bickers and Aukim-Hastie [Bickers and Aukim-Hastie, 2009]). We are particularly interested in finding effective biomarkers for assessing treatment response to hormonal agents in prostate cancer. PCA3 and TMPRSS2-ERG show great promise in diagnostics, but more data are needed on their utility as markers of treatment response.
The EFFECT trial (EudraCT 2012-000101-69) is an ongoing, prospective, exploratory, open-label, single-arm, multicentre study that will assess the effect of a 6-month extended release formulation of leuprorelin acetate (Eligard® 45 mg) on the following prostate cancer biomarkers: PSA in serum; PCA3 in urine; TMPRSS2-ERG-mRNA in blood/peripheral blood mononuclear cells (PBMCs); PSA-mRNA in blood/PBMCs; and PCA3-mRNA in blood/PBMCs.
The study aims to enrol 50 patients with histologically confirmed metastatic prostate cancer for which androgen deprivation therapy is indicated and an expected survival of ≥12 months. Patients will receive a single subcutaneous depot of leuprorelin acetate. Blood and urine samples will be collected pre-injection on day 1 and at 6, 12 and 24 weeks postinjection for analysis of biomarkers at a central laboratory. Urine samples will be taken post-DRE and assessed for PCA3 in patients with an intact prostate only. PCA3 in urine will be assessed using the Progensa® assay. TMPRSS2-ERG mRNA, PSA mRNA and PCA3 mRNA in PBMCs will be analysed using a real time detection and quantification method based on nucleic acid sequence-based amplification (reverse transcription polymerase chain reaction). The relationship between ‘classic’ (testosterone and PSA) and ‘modern’ (PCA3 and TMPRSS2-ERG gene fusion) biomarkers will be explored using correlation and other appropriate techniques.
Conclusion
Better cancer biomarkers have the potential to improve diagnosis, treatment strategy, disease monitoring and prediction of treatment success [Bhatt et al. 2010]. In prostate cancer, where the uptake of PSA testing has arguably led to overdiagnosis and overtreatment, there is a clear need for more specific biomarkers to guide the physician and many different biomarkers are being investigated. There is a particular need for reliable markers of treatment response to hormonal therapy in cancer, but few data on whether markers such as PCA3, PCA3-mRNA or TMPRSS2-ERG-mRNA can fulfil this role. The EFFECT trial will provide preliminary data on the potential utility of these biomarkers for detecting therapeutic response after hormonal therapy using a 6-month extended release formulation of leuprorelin acetate (Eligard® 45 mg).
Footnotes
Funding
The EFFECT study is funded by Astellas Pharma Europe Ltd. Medical writing assistance was provided by Lindsay Napier (Darwin Healthcare Communications), funded by Astellas Pharma Europe Ltd. Editorial assistance was provided by David McMinn (Complete HealthVizion), funded by Astellas Pharma Europe Ltd.
Conflict of interest statement
E.B.B. is an employee of Astellas. J.S., S.D. and I.V.O. have no conflicts of interest to declare.