
Abstract
Objectives:
The aim of the study was to increase the efficiency of treatment for severe symptoms of overactive bladder (OAB) with antimuscarinic drugs in elderly men and women.
Methods:
A total of 341 patients over 65 years of age (average age 69.9; 186 women and 155 men) with severe symptoms of OAB (frequency of incontinence episodes [IEs] ≥ 3/day) underwent examination. Patients were distributed into three main groups: A (n = 58; trospium 60 mg/day + solifenacin 20): three cycles, each cycle 8 weeks, with an 8-week interval; B (n = 55; trospium 30 mg/day + solifenacin 10), regimen was the same as in group A; C (n = 62; trospium 30 mg/day + solifenacin 10) daily during 1 year.
Results:
The most successful treatment for the clinical and urodynamic symptoms of OAB was observed in group A, without an increase in the quantity or intensity of side effects (IEs = 4.8 (0.9) → 1.4 (0.8); p ≤ 0.01). Groups B and C also demonstrated positive effects for most of the markers for lower urinary tract state with statistical significance p ≤ 0.01. Nonparametric correlation between decrease in IEs and relative number of patients who accurately fulfilled prescriptions was in group A, r = 0.53, p ≤ 0.05; in group B, r = 0.61; p ≤ 0.05; in group C, r = 0.55, p ≤ 0.05.
Conclusions:
Cyclic therapy with two different spectrum antimuscarinics appears to be effective for controlling severe OAB in elderly patients. One-year cyclic therapy with a trospium and solifenacin combination provides a high compliance level (76–84%). However, continuous therapy with standard doses of trospium and solifenacin results in low adherence and high rates of treatment withdrawals (≥ 66%) despite satisfactory clinical and urodynamic results.
Introduction
It is well known that the main symptoms of overactive bladder (OAB), that is, incontinence, urgency, and frequent urination, cause suffering for people of any age, but elderly men and women have particularly poor tolerance of these symptoms [Kraus et al. 2010; Yoo et al. 2011; Natalin et al. 2013]. The prevalence of OAB increases after 40 years of age. Recent epidemiological studies in the USA showed that the prevalence of OAB among people aged over 40 years is 26–33% for men and 27–46% for women (with race differences); among people aged over 65 years it reaches 40.4% and 46.9% for men and women, respectively [Sexton et al. 2011; Coyne et al. 2012; Griebling, 2013; Milsom et al. 2013].
Manageability of OAB symptoms in elderly people has increased significantly recently. This is due to the introduction of new antimuscarinic drugs, which enable good therapeutic results to be obtained and avoid many of the undesirable effects that are common for first-generation drugs [Erdem and Chu, 2006; Wagg et al. 2007]. Of course, drugs with other mechanisms of action on the detrusor, such as onabotulinumtoxin A and antagonists of beta-3 adrenoreceptors (mirabegron) are also being investigated [Igawa et al. 2010; Andersson, 2013; Chapple et al. 2014], but the current range of antimuscarinic drugs still has potential for increasing effectiveness, and optimization of treatment regimen for OAB in elderly patients remains an important issue. Studies of rational approaches to the application of antimuscarinic drugs in elderly patients with due consideration of ‘old’ bladder and behavioral stereotypes, which are common for elderly people, are still performed [Geoffrion, 2012; Veenboer and Ruud Bosch, 2014; Sicras-Mainar et al. 2014].
Previously we studied the effectiveness of management of OAB symptoms in elderly men and women with combined high doses of antimuscarinic drugs. It was established that administration of trospium and solifenacin over 5 weeks significantly improved the urodynamics of the lower urinary tract (LUT) without increasing side effects [Kosilov et al. 2013].
This study aimed to compare the effectiveness and safety of cyclic and permanent 1-year treatment for OAB symptoms in elderly patients with consideration of the problems related to the accuracy of fulfilling prescriptions in cases of long-term administration of drugs [Noe et al. 2004; Shaya et al. 2005; D’Souza et al. 2008].
Methods
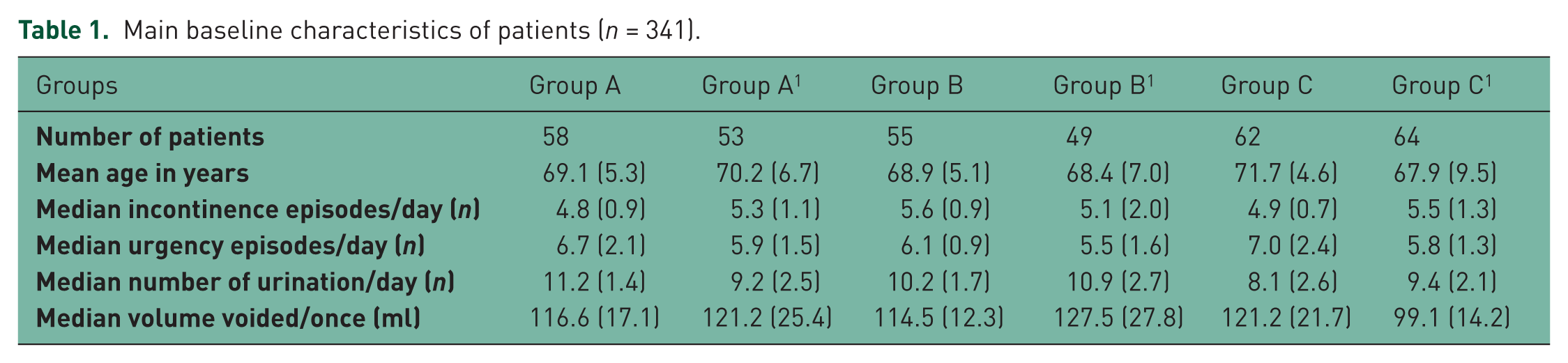
A longitudinal, randomized study was performed from 1 March 2012 to 1 June 2013 in the neurourological department of Primorsky Regional Diagnostic Center. A total of 341 patients over 65 years of age (average age 69.9 years; 186 women and 155 men) were enrolled. All participants were outpatients. The total patient number was 516, of whom 175 were excluded at the preliminary stage. The basic characteristics of the patients are shown in Table 1. Research was performed in accordance with the Declaration of Helsinki, international rules and standards for urodynamic examinations [Brown et al. 2013; Gurpreet et al. 2010; Schafer et al. 2002; Schroder et al. 2009; Singh et al. 2010]. Patients with severe symptoms of OAB (frequency of incontinence episodes [IEs] ≥ 3/day) were included in the study [Rovner, 2005; Dmochowski et al. 2009; Wu et al. 2011]; patients with chronic active diseases and patients with intolerance to antimuscarinic drugs were excluded. Patients had not taken antimuscarinics for at least 1 year prior to study entry. Patients with exacerbations of chronic diseases as well as individuals with antimuscarinic intolerance, central nervous system organic lesions, and a history of long QT syndrome or ventricular flutter were excluded from the study. Generation of random-number sequences during patient selection was performed using the median of squares method. Stratified randomization was used during group formation adjusting for important characteristics influencing the treatment results such as sex and OAB severity. Strata included individuals according to week days. All study participants (patients and staff) were blinded to treatment allocation: all medications (antimuscarinics and placebo) had a similar appearance, taste, and dosage regimen.
Main baseline characteristics of patients (n = 341).
The algorithm of clinical and urodynamic examination of patients is shown in Figure 1. The aim of the study was to determine the efficacy of a cyclic regimen of trospium and solifenacin in elevated and standard doses versus continuous regimens in standard doses for the control of severe OAB in elderly patients. The study endpoints were LUT clinical and urodynamic parameters after 12 months of treatment as well as the percentage of compliant patients.
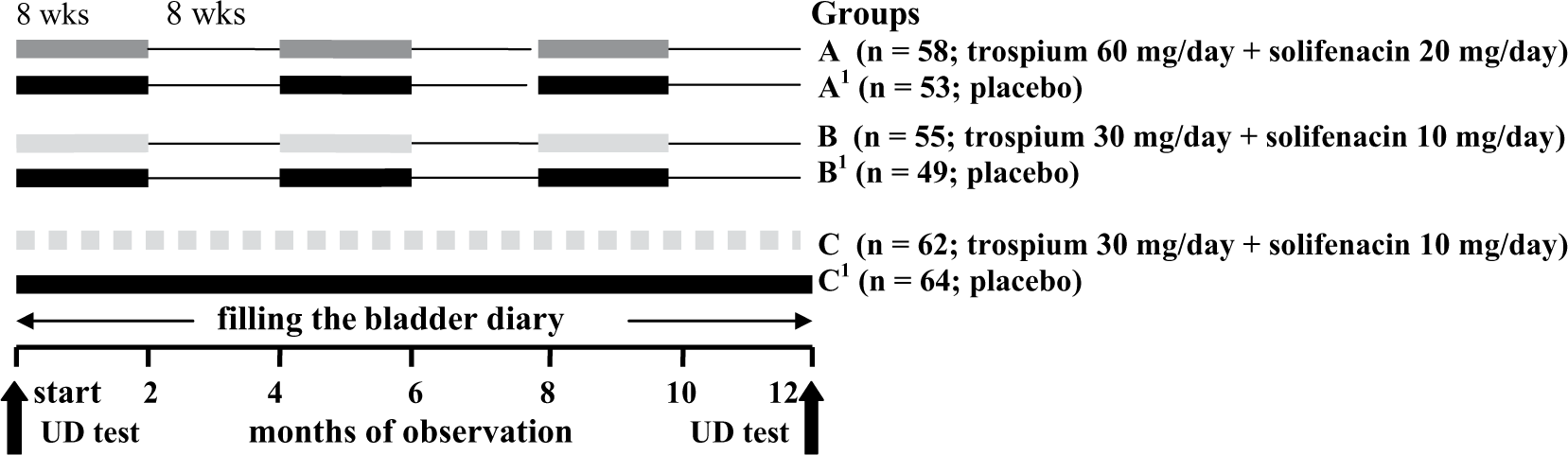
Algorithm of observation and treatment of elderly patients with severe symptoms of overactive bladder (n = 341).
In accordance with the guidelines for administration of drugs patients were distributed into the following groups: A (n = 58; trospium 60 mg/day + solifenacin 20): three cycles of drug therapy, 8 weeks each, with an 8-week interval during 1 year; B (n = 55; trospium 30 mg/day + solifenacin 10), the algorithm is the same as in group A; C (n = 62; trospium 30 mg/day + solifenacin 10), daily over 1 year. In control groups A1 (n = 53), B1 (n = 49), C1 (n = 64) patients received placebo. In our study all medications were free for our patients in accordance with the national obligatory medical insurance program.
The primary outcome measures were decrease in IEs to ≥ 1.5/day and optimization of LUT urodynamic parameters, that is, at least 30% increase in median reflex volume, bladder capacity, and detrusor compliance against background. The above changes in IEs and urodynamic parameters suggest significantly effective therapy [Rovner, 2005; Dmochowski et al. 2009; Wu et al. 2011]. Criteria for accuracy of prescription fulfillment were observation of dosage instruction and time of administration not less than six times a week. Urodynamic examination was performed at the beginning and at the end of the twelfth month of the study. All patients filled standard OAB questionnaires recommended by the International Continence Society at the beginning and end of the follow-up period, and during the year they kept daily bladder diaries where they recorded data concerning frequency of IEs, volume of single urination, quantity of urinations and urgencies per day, and they also marked the time and dose of administered drugs [Amundsen et al. 2006; Parsons et al. 2007; Tissot et al. 2008].
The program JMP SAS Statistical Discovery 8.0.2 (SAS Institute, Cary, NC, USA) was used for the statistical processing of data. To reveal a 5% difference in significance level with 80% power and assumed for such study type standard deviation we needed to recruit 54 patients per treatment and control groups. Patient numbers were somewhat increased to take into account any drop outs. Thus the total number of patients was 341. p < 0.05 was considered statistically significant. The Wilcoxon and Kruskal–Wallis tests were used to compare results in each group; the Kruskal–Wallis rank test was used for control of equality of medians from different groups. One-way analysis of variance with Tukey–Kramer honestly significant difference was used to compare effects in three and more groups, and Spearman’s correlation coefficient was applied to study dependence between processes.
Results
The results of urodynamic examination in group A (Table 2) demonstrate a notable improvement in state of the LUT. Differences are significant in all cases, statistical significance of change of postvoid residual (14.1 (2.9) →31.3 (3.4)), reflex volume (116.7 (19.3) →178.4 (21.9)), and bladder capacity (166.2 (27.2) →248.1 (21.4)) is p ≤ 0.01. Improvement of indexes in group C was also noted (p ≤ 0.05). Cross-sectional analysis of urodynamic parameters during control examination demonstrated significant differences between treatment and control groups for most paired comparisons. The exception was for postvoid residual in A–A1 and B–B1 pairs due to high within-group variation. Reflex volumes were significantly different in A–A1 and B–B1 pairs (178.4 (21.9) versus 136.0 (14.6); p < 0.05, and 188.1 (24.2) versus 121.3 (41.4); p < 0.05, respectively). The most prominent difference between treatment and control groups was revealed for bladder capacity: A–A1: 248.1 (21.4) versus 145.8 (35.8); p < 0.01; B–B1: 241.0 (34.7) versus 147.7 (29.4); p < 0.01. Detrusor compliance values were also markedly higher after treatment in the A1 group (p < 0.01).
The results of urodynamic studies (before treatment n = 341).
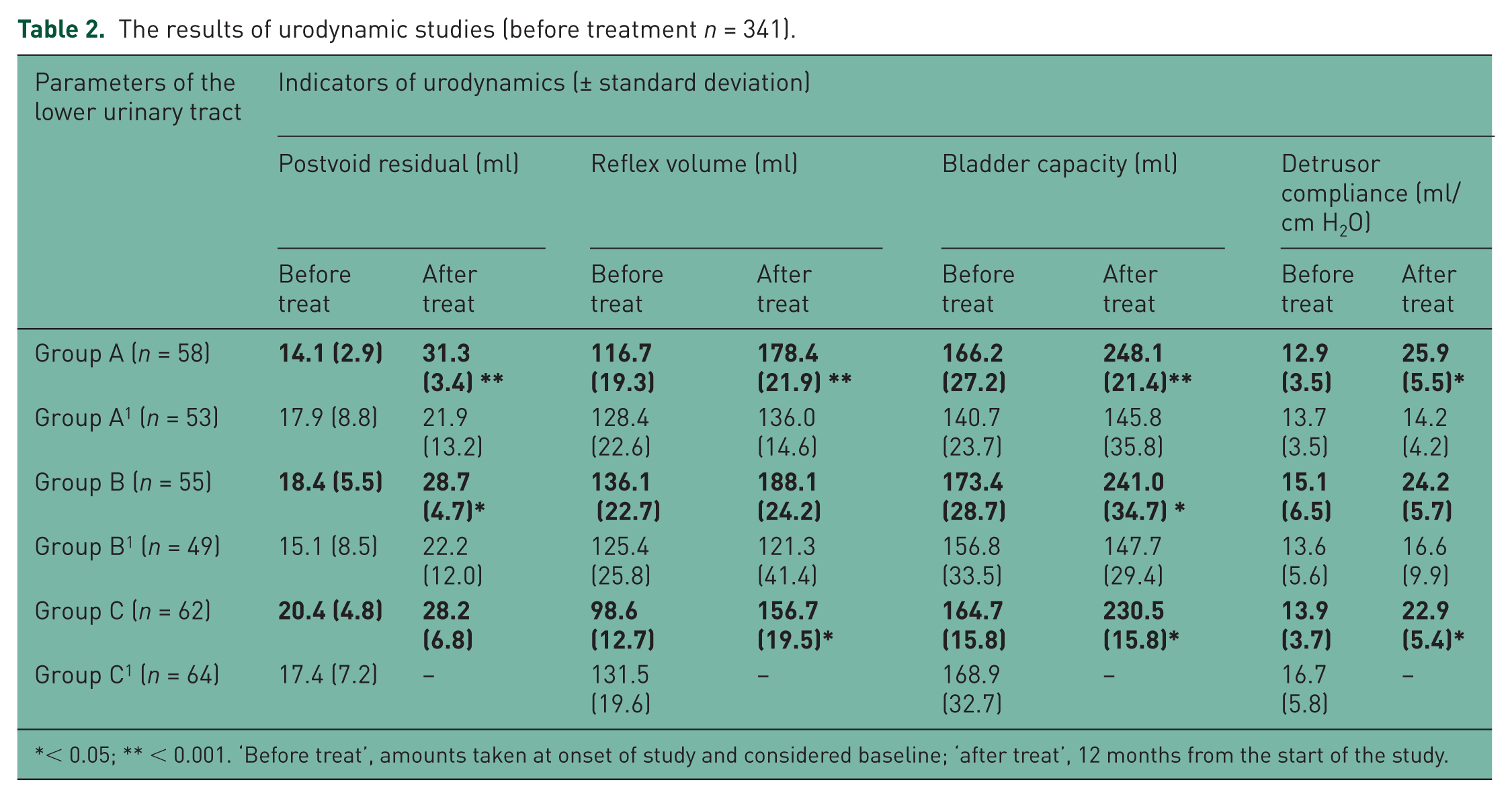
< 0.05; ** < 0.001. ‘Before treat’, amounts taken at onset of study and considered baseline; ‘after treat’, 12 months from the start of the study.
Frequency of IEs (Figure 2, Table 3) in group A decreased to 3.3/day (p ≤ 0.01) after the second month of follow up; by the end of the sixth month this index decreased to 3.8 /day (p ≤ 0.01) from initial data, reached 1.3/day in absolute terms, and remained consistently low during all of the follow-up period. Decrease in frequency of daily urinations and urgencies was related to the value of IEs (r = 0.65 (p ≤ 0.05) и r = 0.59 (p ≤ 0.05)).

Dynamics of the decrease in frequency of incontinence episodes in elderly patients according to group. y-axis, median of absolute values from baseline in number of incontinence episodes per day. x-axis, months of observation.
Results of clinical assessment (n = 341).
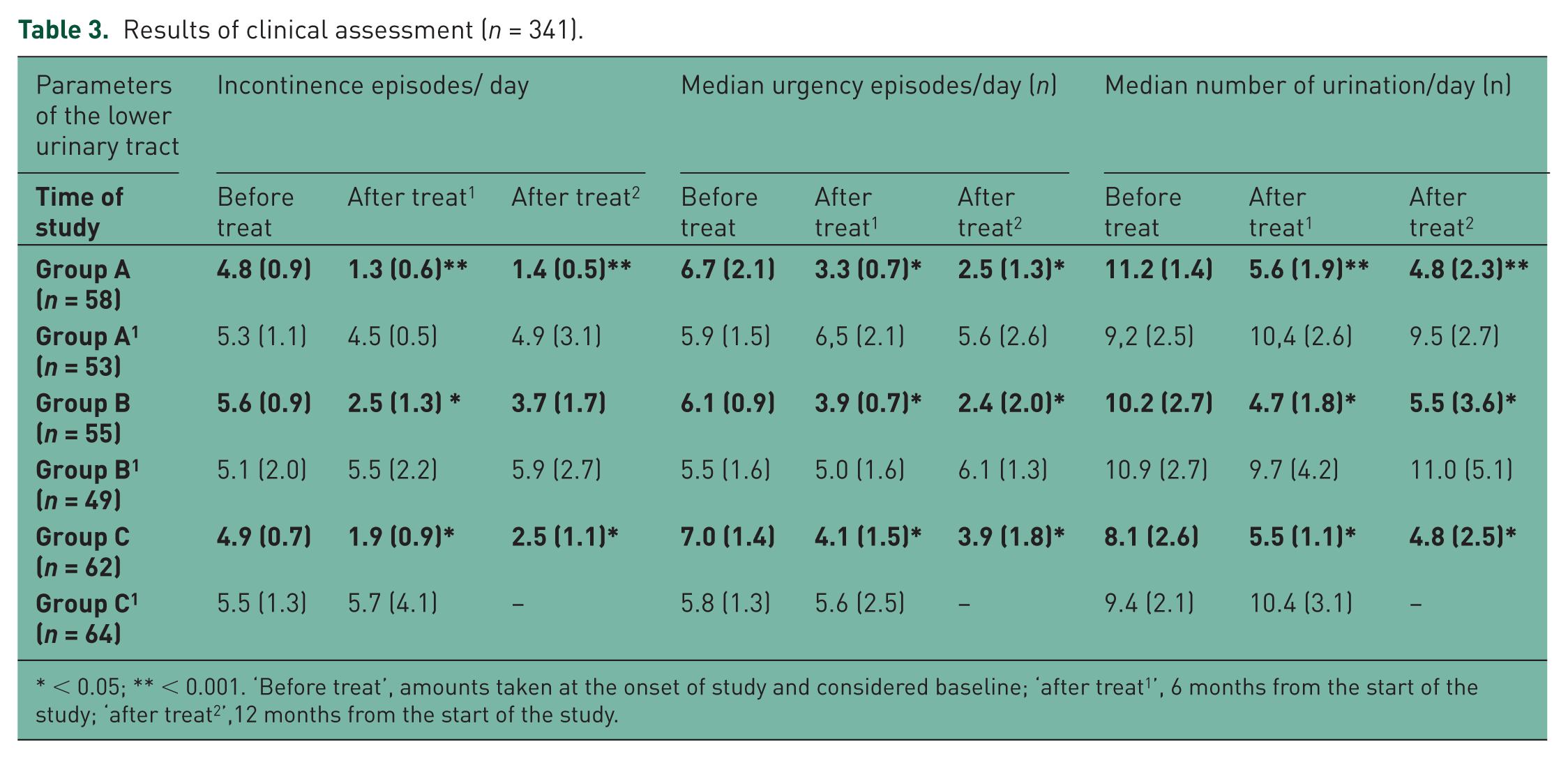
< 0.05; ** < 0.001. ‘Before treat
Cross-sectional analysis of clinical urination parameters suggested that the number of daily IEs in group A after 12 months of follow up was significantly different from that in group B (1.4 (0.5) and 3.7 (1.7), p < 0.05). However this parameter was not significantly different between groups A and C, neither after 6 nor 12 months (p ≥ 0.05). Data obtained throughout the study showed that daily values of median urgency episodes and median number of urinations were changing synchronously without significant differences between groups A, B, and C (p ≥ 0.05). Paired comparisons of these parameters at 6 and 12 months after treatment initiation demonstrated significant differences in treatment and placebo groups (p < 0.05 for all comparisons).
The dynamics of the percentage of patients who accurately followed drug instructions is shown in Figure 3. In group A the number of patients who fulfilled all prescriptions at the end of the study decreased for nine persons in comparison with the beginning of the study and reached 85.5%, which was not significantly different from the results in group B (76.5% (p ≥ 0.05). At the beginning of the third cycle the percentage of patients who followed all instructions in control groups A1 and B1 (66.0% and 59.2%) decreased significantly in comparison with groups A and B (87.9% and 81.8%) (p ≤ 0.05 and p ≤ 0.05, respectively), and almost did not differ between themselves (p ≥ 0.05).

Changes in number of elderly patients who accurately followed instructions for the administration of drugs, in percentage (a) during first 3 months of follow up, (b) throughout the year. y-axis, percentage of patients; x-axis, months of observation.
The percentage of patients who accurately followed all instructions in group C demonstrated a steady decreasing trend from the beginning of the study, and after the fifth month of follow up it was significantly different from that in groups A and B (p ≤ 0.05 with both groups). The decreasing trend continued and at the end of follow up the percentage of such patients was 30.6%. The number of patients who failed to fulfill prescriptions in control group C1 grew rapidly, and by the end of the third month the percentage of patients who followed instructions was 76.5%, by the end of fourth month, 53.1%, by the end of fifth month, only 17.1%, and after 6 months a majority of patients refused to continue the treatment (89.1%).
During the first 2-month cycle of follow up the percentage of patients who failed to follow instructions or refused to continue the therapy in the main groups was insignificant (6.6–8.6%). At the end of the sixth month, however, the difference between groups A (87.9%) and B (85.4%), on the one part, and C (66.1%), on the other part, became statistically significant (p ≤ 0.05).
Correlation of decreasing trend for number of patients who accurately fulfilled prescriptions in groups A and B was high: r = 0.89 (p ≤ 0.01). In group C the accuracy of prescription fulfillment decreased steadily, and by the end of the fifth month the percentage of such patients was significantly different from the initial data (72.5%; p ≤ 0.05), by the end of the sixth month, from results in group A (87.9) and group B (85.4) with p ≤ 0.05. Calculation of nonparametric correlation between frequency of IEs and the relative number of patients who accurately fulfilled prescriptions, demonstrated moderate direct correlation in groups A (r = 0.53; p ≤ 0.05), B (r = 0.61; p ≤ 0.05), and C (r = 0.55; p ≤ 0.05).
Seven patients (12.1%) in group A reported side effects, and among them one patient (1.7%) refused to continue the treatment due to the side effects. In group B side effects were also reported by seven patients (12.7%), but none stopped treatment for this reason. In group C 12 patients (19.3%) noted side effects during the treatment and 3 patients (4.8%) refused to continue the treatment. The reason for discontinuation of the treatment in all cases was intolerably dry mouth. Other side effects included dry and itching skin (six patients), dizziness and disorder of coordination (five), headache (one), nausea (one), and flatulence (one). In total, four patients discontinued treatment due to adverse events; three patients (all from group C) withdrew due to lack of treatment efficacy; four patients discontinued treatment for other reasons. Data on withdrawals and adverse events are shown in Table 4.
Cases of side effects and discontinuation of treatment (n = 341).

The figures in parentheses indicate the number of patients who refused further therapy because of side effects.
Discussion
Treatment-effect studies of two antimuscarinics have already been carried out before by our group as well as by other investigators [Diokno et al. 2001; Kosilov et al. 2013]. Combination of two antimuscarinics affecting different bladder receptors has been proved to be an effective and safe method for long-lasting and therapy-resistant OAB.
Continuous monotherapy or combination therapy with antimuscarinics for up to 1 year or more for OAB is recommended by many authors [Dmochowski et al. 2009; Wu et al. 2011; Andersson, 2013; Veenboer and Ruud Bosch, 2014]. However, long-term treatment is associated with the risk of patient noncompliance [Zinner et al. 2008; Yi et al. 2013]. In our study we compared patient compliance in the groups of cyclic and continuous antimuscarinic treatment over a 1-year period.
As a result of the study it was established that the urodynamic indexes for the LUT changed the most rapidly in the group of elderly patients treated with high-dose trospium and solifenacin in cyclic form. In group A significant differences in median values of urodynamic indexes were observed. In groups B and C the urodynamic state also improved in the majority of patients, but not all indexes demonstrated significant differences from the initial data.
The frequency of IEs in patients from group A rapidly decreased by the second month of follow up (-3.3, p ≤ 0.01) and remained steadily low (-3.4; -3.8) during the course of the follow up. In group C the pattern of improvement in frequency of IEs was smoother; in group B the frequency of IEs decreased by the end of the cycle and somewhat increased (insignificantly) when patients stopped administration of antimuscarinic drugs.
Thus we determined that continuous treatment with two antimuscarinics resulted in synchronic change of clinical outcome measures (IEs, median urgency episodes, and median number of urinations), those being significantly different versus baseline and controls. The majority of urodynamic parameters were significantly different in treatment and control groups both at baseline and at the end of the study. Similarly most urodynamic parameters in each treatment group differed from the same parameters in the control group. This provides evidence that in elderly patients with severe OAB the combination of two antimuscarinics affecting different receptors in standard doses is an effective method regardless of treatment schedule, either continuous or cyclic.
Quite a different situation occurs with the adherence to cyclic and continuous treatment regimens (the second study endpoint). In general, under cyclic therapy patients, who were treated with standard-dose and high-dose antimuscarinic drugs, demonstrated a high level of discipline in fulfillment of prescriptions. In other words, the accuracy of prescription fulfillment in groups with cyclic treatment was steadily high during the year of follow up. On the contrary, in the continuous treatment group, in spite of satisfactory therapeutic effect, compliance decreased below the critical threshold at the study midpoint, retaining less than one third of patients by the end of study.
Such results let us suppose that short-term treatment with high-dose antimuscarinic drugs in elderly patients with severe symptoms of OAB is more effective because it keeps at least some of the patients, who have problems with operative memory and possibly lack of will to follow instructions accurately, focused on the treatment and helps to increase motivation for accurate fulfillment of prescriptions. Discontinuity of cyclic therapy provides some effect of novelty and positive expectations at the beginning of the next course, which makes such an algorithm more effective in comparison with long continuous treatment with antimuscarinics [Diokno et al. 2001; Horstmann et al. 2006; Amend et al. 2008; Chapple et al. 2008; Smith et al. 2011].
However, if elderly patients do not receive a treatment effect in a short timescale, motivation to adhere to treatment declines, resulting in poor compliance with incorrect schedules, missing doses, and self-administered dose changes as well as treatment discontinuation.
Conclusion
Cyclic therapy with two different spectrum antimuscarinics appears to be effective for controlling severe OAB in elderly patients. One-year cyclic therapy with trospium and solifenacin combination provides a high compliance level (76–84%). However, continuous therapy with standard doses of trospium and solifenacin results in low adherence and high rates of treatment withdrawals (≥ 66%), despite satisfactory clinical and urodynamic results.
Footnotes
Funding
Funding study researches were conducted without the involvement of third-party grants, solely on the own funds of the authors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.