
Abstract
Introduction:
Peyronie’s disease (PD) is a chronic wound-healing disorder characterized by formation of fibrous inelastic scarring of the tunica albuginea resulting in a variety of penile deformities. In most cases, PD is accompanied by a physical and psychological impact. Xiaflex® is an injectable collagenase clostridium histolyticum (CCh) preparation consisting of a predetermined mixture of two distinct collagenases. Recently the US Food and Drug Administration (FDA) approved Xiaflex® for the nonsurgical treatment of men with PD with curvature of 30° or more and tangible scar tissue plaque in their penis.
Method:
This article presents a comprehensive review of the updated information on the use of Xiaflex® for the nonsurgical treatment of PD.
Results:
Mean improvements in penile curvature ranging from 29% to 34% and in bother domain scores have been reported. The majority of the reported adverse effects are mild or moderate and 79% resolve without intervention.
Conclusion:
The combined results of these trials have led to the FDA approval of CCh for the treatment of PD. However, the long-term effects and results need further investigation, with large follow-up series. Considering these results, future perspectives will probably result in the use of a combined or sequential therapy including CCh.
Introduction
Peyronie’s disease (PD) is a chronic wound-healing disorder characterized by formation of fibrous inelastic scarring of the tunica albuginea following trauma of the penis and causing a variety of deformities, including curvature, shortening, narrowing and hinge defect [Taylor and Levine, 2007; Devine et al. 1997]. In most cases it is associated with a variable degree of erectile dysfunction (ED), which significantly affects the quality of life of the patient and his partner [Bjekic et al. 2006; Qian et al. 2004; Gelbard et al. 1990; Mulhall et al. 2006].
In addition to physical symptoms, the psychological impact of PD should be considered. Studies show that many patients experience clinical depression, emotional and relationship difficulties, and poor self-esteem [Nelson et al. 2008; Smith et al. 2008].
Surgical therapy remains the gold standard for correcting erect penile deformity as a result of PD, and should be indicated in the chronic phase (at least 6 months of stable disease) and when penile curvature precludes intercourse [Ralph et al. 2010].
Nonsurgical treatments already tested are vitamin E, potaba, tamoxifen, colchicine, carnitine and pentoxifiline. Intralesional injectable agents such as interferon, collagenase and verapamil, and more recently, electromotive therapy, iontophoresis, radiation therapy and traction therapy, have been studied. The majority were ineffective or not suitable for clinical use.
Collagenase clostridium histolyticum (CCh) was first introduced nearly 20 years ago as a potential novel approach to treat Dupuytren disease [Shaunak et al. 2011]. The first study describing the use of collagenase in PD was conducted by Gelbard in 1985 with 31 patients; it concluded that collagenase seemed to be effective in the treatment of PD [Badalamente and Hurst, 2007; Gelbard et al.1985]. In 2010 the US Food and Drug Administration (FDA) approved Xiaflex (® Auxilium Pharmaceuticals, Inc, Malvern, PA) as an office-based nonsurgical treatment for adult patients with Dupuytren’s contracture with a palpable cord. Treatment consists of collagenase injection directly into Dupuytren’s affected cords, followed by a standardized finger extension procedure.
The association between Dupuytren’s disease and PD is widely described in the literature and is supported by an inherited autosomal dominant pattern [Chilton et al. 1982; Carrieri et al. 1998].
Xiaflex is an injectable collagenase preparation consisting of a predetermined mixture of two distinct collagenases that cleave collagen strands at different sites. AUX I (a class I Clostridium histolyticum collagenase) cleaves the terminal ends of collagen, and AUX II (a class II C. histolyticum collagenase) cleaves internal sections of collagen [French et al. 1987; Gelbard et al.1985]. Until recently, Xiaflex was considered to be an investigational treatment for PD, and its use was limited to clinical trials. However, the FDA has now approved Xiaflex for the nonsurgical treatment of men with PD who have a curvature of 30° or more and tangible scar tissue plaque in their penis [http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm377849.htm].
Literature review methods
Numerous clinical studies have been conducted to define the effects and outcomes of CCh in PD from 1985 to the present day. This article presents a comprehensive review of the updated information available on the use of CCh for the nonsurgical treatment of PD.
A systematic literature search of Medline was performed by the authors using the Medical Subject Headings (MeSH) database. The search included the MeSH terms ‘penile induration and collagenase’, Xiaflex, and ‘Peyronie’s disease and collagenase’. The search included all relevant articles published in English language up to January 2014.
Results
As a result of the Medline search, six studies conducted between 1985 and 2013 were identified that determined the efficacy and safety of CCh in the treatment of PD. We focused on the last three studies (one phase II study published in 2012 and two phase III studies published in 2013) submitted to FDA during the product’s approval process.
In 2012, Gelbard and colleagues reported the results of a phase IIb multicentre, prospective, randomized, placebo-controlled study to determine the safety and efficacy of CCh [Gelbard et al. 2012]. Patient-reported outcome questionnaires were used. In this phase II study, a total of 147 subjects with PD (27% of patients with a history of PD < 12 months), stratified by degree of curvature (30–60º or >60º) were randomized into four groups to receive CCh versus placebo (3:1), with or without plaque modelling (1:1). Per-treatment cycle, two injections of CCh 0.58 mg (10,000 units) were given 24–78 h apart. Subjects received up to three cycles at 6-week intervals. Penile modelling consisted of a gentle stretching of the flaccid penis in the opposite direction to the curvature. The physician held the stretched position for 30 s, before allowing the penis to return to the nonmodelled position for 30 s. This procedure was repeated three times. When designated, investigator modelling was applied 24–72 h after the second injection of each cycle.
Primary efficacy endpoints were the change from baseline in penile curvature and the change in total score for each PD-PRO domain score (a nonvalidated 15-question, disease-specific, patient reported outcome measure for quantifying the psychosexual impact, resulting from the physical and psychological symptoms of PD, in accordance with established scientific standards and guidance from the FDA to advance the research and understanding of PD), and International Index of Erectile Function (IIEF) score. Safety analysis was based on the adverse event (AE) incidence, and the change from baseline in laboratory values and vital signs.
After CCh treatment, significant mean improvements in penile curvature (29.7% versus 11%, p = 0.001) and patient-reported outcome symptom bother scores (p = 0.004) were observed compared with placebo. Subjects who underwent the modelling procedure showed a mean 32.4% improvement in penile curvature versus a mean 2.5% worsening in curvature for the placebo group (p < 0.001). Subjects without modelling experienced a 27.1% mean improvement in penile curvature when treated with CCh, which did not statistically significantly differ from the 27.9% mean improvement observed for placebo. No significant differences in IIEF were observed. Efficacy and safety assessments were recorded over 36 weeks, and AEs were mostly mild or moderate (injection site bruising, oedema, rash, penile pain). No treatment-related serious AEs were reported.
More recently, Gelbard and colleagues published the results of two phase III multicentre, prospective, randomized, double-blind and placebo controlled studies (IMPRESS I and IMPRESS II) to determine the clinical efficacy and safety of intralesional CCh in subjects with PD. In both studies, the primary goal was to assess the change in penile curvature. A total of 417 and 415 patients, respectively, were enrolled. The main duration of PD history was 4.1 years. Patients received up to four cycles of 0.58 mg CCh, consisting of two injections per cycle with a 6-weeks interval between each cycle. One to three days later, penile plaque modelling was conducted. The results showed a mean improvement in penile curvature (34% versus 18%; p < 0.0001) and in bother domain score (p < 0.0037) assessed using the Peyronie’s Disease Questionnaire (PDQ; the first validated PD-specific patient-reported measure of psychosexual impact). Secondary endpoints were the percentage of global responders, PDQ psychological and physical symptoms, IIEF overall satisfaction, percentage of composite responders (patients with 20% or greater improvement in penile curvature plus an improvement in the PDQ PD bother score of 1 or greater), and plaque consistency [Gelbard et al. 2013]. The post hoc meta-analysis, which combined the study databases to improve statistical power, revealed statistical significance in all secondary endpoints except penile length and penile pain based on the multiple comparison algorithm.
Table 1 illustrates the baseline characteristics of the patients enrolled in the CCh trials.
Summary of baseline characteristics of patients.
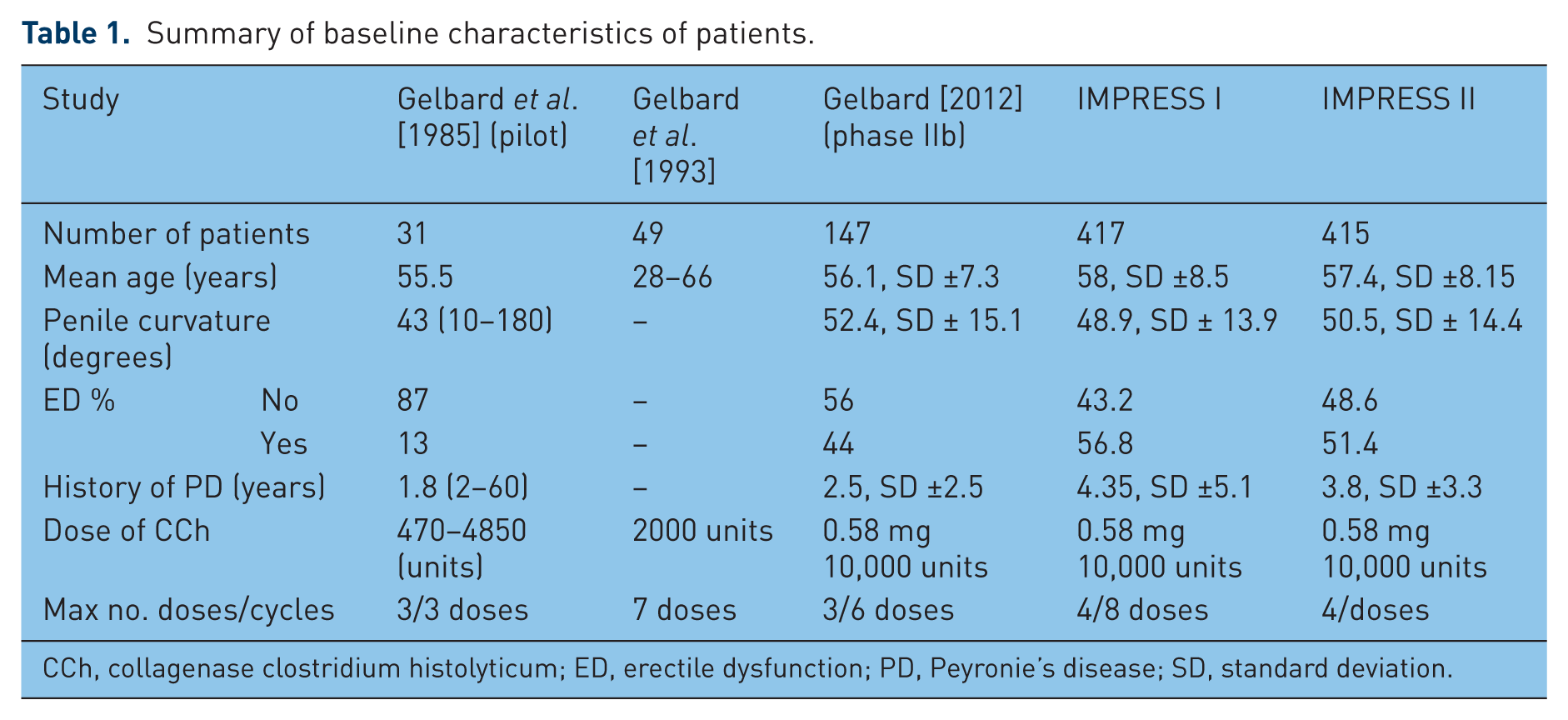
CCh, collagenase clostridium histolyticum; ED, erectile dysfunction; PD, Peyronie’s disease; SD, standard deviation.
AEs were found in 82.4% of patients treated with CCh compared with 36.3% receiving placebo. The only AEs exceeding 5% in this series were pain at the injection site, swelling, and bruising. All the reported AEs were mild or moderate, and 79% resolved without intervention within 14 days. Six patients experienced serious AEs, including three penile hematomas and three corporeal ruptures that required surgical repair.
The standard dose was established at 0.58 mg, equivalent to 10,000 units divided into four cycles of two injections per cycle.
No cases of anaphylaxis were reported across any of the trials. The long-term immune responses to collagenase are currently being studied as requested by the FDA.
Table 2 illustrates the results of the three main CCh trials: phase IIb trial, IMPRESS I, and IMPRESS II.
Summary results of randomized clinical trials.
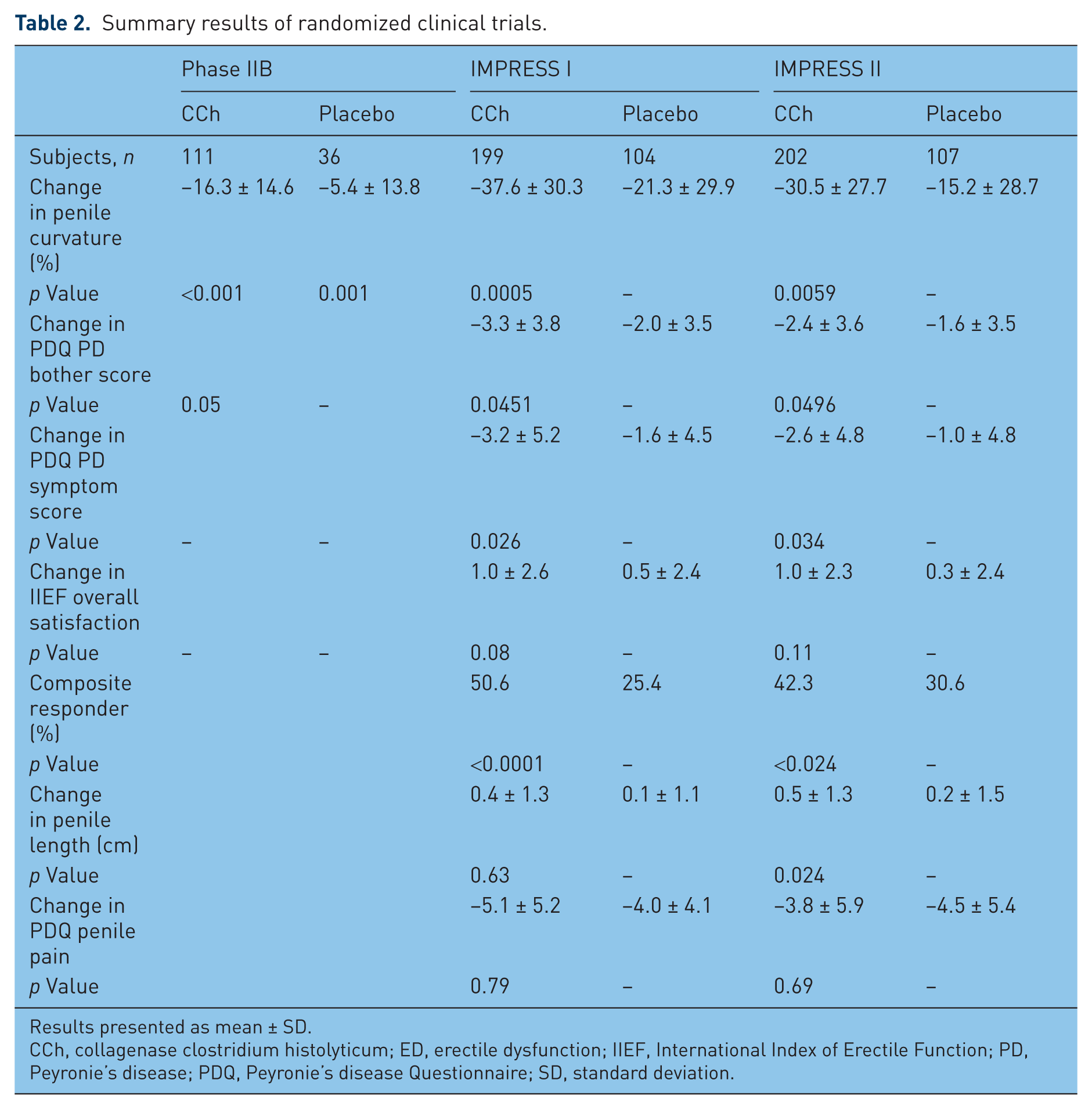
Results presented as mean ± SD.
CCh, collagenase clostridium histolyticum; ED, erectile dysfunction; IIEF, International Index of Erectile Function; PD, Peyronie’s disease; PDQ, Peyronie’s disease Questionnaire; SD, standard deviation.
Discussion
A number of medical therapies have been tried for the treatment of PD; unfortunately not many have been subjected to double-blind drug testing. However, data from controlled studies showing efficacy are limited for most historically available minimally invasive treatments. The FDA approval of CCh represents a renewed interest in the conservative management of PD. A key benefit of minimally invasive treatment is the improvement in PD signs, such as penile curvature and psychosocial symptoms, with less morbidity than with surgery [Gelbard et al. 2013].
The European Association of Urology (EAU) guidelines provided recommendations for the diagnosis and treatment of congenital and acquired PD penile curvature [Hatzimouratidis et al. 2012]. This should be focused on patients in the early stage of the disease when symptoms are present and the plaque is not densely fibrotic or calcified [Rybak et al. 2012]. The role of conservative treatment in men with stable or chronic disease has not been adequately defined. Under these directions, conservative management in the acute PD phase is obtaining a progressively larger consensus among experts [Hatzimouratidis et al. 2012; Jordan, 2008]. Moreover, the EAU considers that intralesional treatment with clostridial collagenase showed significant decreases in the deviation angle, plaque width and plaque length, and recommended its use with a level of evidence 2b and recommendation grade C, based on two small studies, with poor samples of patients and insufficient follow-up periods [Rybak et al. 2012; Gelbard et al. 1993]. However, the last update of the guidelines (2012) was made before the trials for the FDA approval were published [Gelbard et al. 2013].
The preliminary experience of the use of CCh for the treatment of Dupuytren’s disease concludes that the application of continuous traction in Dupuytren’s contracture increases the activity of degradative enzymes. This initially leads to a loss of tensile strength and ultimately to solubilization. It is followed by an increase in newly synthesized collagen [Gilpin et al. 2010]. This phenomenon is called mechanotransduction. The principle of mechanotransduction (a cellular process that translates mechanical stimuli into a chemical response that leads to activation of cell proliferation) has been applied to the use of penile traction therapy (PTT) in the nonsurgical treatment of PD. Data from studies are encouraging; also, in our preliminary experience, PTT was found to be safe and effective [Martínez-Salamanca et al. 2011; Abern et al. 2012]. Recently our group published the results of a prospective, randomized and controlled trial to determine the efficacy of PTT on the conservative treatment of the acute phase (AP) of PD, A total of 55 patients underwent PTT for 6 months and were compared with 41 patients with AP of PD who did not receive active treatment (‘no intervention group’). After 6 months of treatment and a mean follow up of 9 months, we found a statistically significant decrease in the mean curvature, from 33° at baseline to 15° at 6 months and 13° at 9 months, with a mean decrease of 20° (p < 0.05). Also, there was a significant increase in stretching penile length and flaccid girth (p = 0.03) [Martínez-Salamanca et al. 2014]. Moreover, we identified predictors of treatment success: penile curvature greater than 45° at baseline, visual analogue scale score for penile pain greater than 5, time from diagnosis less than 3 months, absence of plaque on the ultrasound study, and age under 45 years.
The three studies comparing the efficacy of CCh and penile modelling in the treatment of PD showed a statistically significant reduction in penile curvature in patients treated with CCh and modelling over CCh alone. These data suggest that modelling further decreases the restrictive effects of the plaque on tunica albuginea expansion during erection. However, these trials are often unclear as to whether the patients under evaluation include those in the early (acute) phase, the late fibrotic (stable) phase, or a combination of patients of both phases. Treatment in the early inflammatory phase can theoretically reduce the degree of inflammation and break the cycle of fibrin deposition and abnormal tissue remodelling [Russell et al. 2007]. Further evaluation regarding the effect of treatment in patients with PD in AP (< 12 months) should be conducted. Because the duration of the disease is significantly less in patients with low baseline curvature severity, this suggests that earlier treatment may be indicated to promote improved responses.
Even the pathophysiology of the disease continues to be the subject of discussion. It is clear that collagenase induces a tissue response that is more effective in those patients with early disease. This effect can be enhanced by a mechanotransduction response-induced therapy (a key ‘step’ in the remodelling phase) like modelling. A similar phenomenon occurs with PTT, which proves to be more effective in the AP. Taking into account these results, future perspectives probably will lie in the use of a combined or sequential therapy, including both CCh and PTT.
The treatment of PD has been and continues to be largely surgical, although in selected patients nonsurgical alternatives appear to be useful to treat this disease. Clinical studies have shown that CCh is effective and safe when administered correctly, although long-term effects and results need further investigation, with large follow-up series. Comparison studies between collagenase and standard surgical treatment (plication or grafting) have not been conducted yet. As the financial costs of the treatment become more affordable (approximately 800 euros per dose), and the long-term effects better elucidated, CCh might be able to shift the current treatment paradigm.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.