
Abstract
Background:
The first Italian national guidelines were developed by the Italian Association of Urologists and published in 2007. Since then, a number of new drugs or classes of drugs have emerged for the treatment of lower urinary tract symptoms (LUTS) related to benign prostatic hyperplasia (BPH), new data have emerged on medical therapy (monotherapies and combination therapies), new surgical techniques have come into practice, and our understanding of disease pathogenesis has increased. Consequently, a new update of the guidelines has become necessary.
Methods:
A structured literature review was conducted to identify relevant papers published between 1 August 2006 and 12 December 2010. Publications before or after this timeframe were considered only if they were recognised as important milestones in the field or if the literature search did not identify publications within this timeframe. The quality of evidence and strength of recommendations were determined according to the Grading of Recommendations Assessment, Development and Evaluation framework.
Main findings:
Decisions on therapeutic intervention should be based on the impact of symptoms on quality of life (QoL) rather than the severity of symptoms (International Prostate Symptom Score (IPSS) score). A threshold for intervention was therefore based on the IPSS Q8, with intervention recommended for patients with a score of at least 4. Several differences in clinical recommendations have emerged. For example, combination therapy with a 5α-reductase inhibitor plus α blocker is now the recommended option for the treatment of patients at risk of BPH progression. Other differences include the warning of potential worsening of cognitive disturbances with use of anticholinergics in older patients, the distinction between Serenoa repens preparations (according to the method of extraction), and the clearly defined threshold of prostate size for performing open surgery (>80 g). While the recommendations included in these guidelines are evidence based, clinical decisions should also be informed by patients’ clinical and physical circumstances, as well as patients’ preferences and actions.
Conclusions:
These guidelines are intended to assist physicians and patients in the decision-making process regarding the management of LUTS/BPH, and support the process of continuous improvement of the quality of care and services to patients.
Introduction
Benign prostatic hyperplasia (BPH) is a complex pathological disease that is progressive in a large proportion of older men. BPH may be associated with bothersome lower urinary tract symptoms (LUTS), which can negatively impact quality of life (QoL) [Emberton et al. 2008]. LUTS/BPH are also associated with considerable healthcare costs [van Exel et al. 2006], and the economic impact is likely to increase in line with the aging of populations.
The Italian Association of Urologists (AURO.it) guidelines were previously updated in 2006 [Spatafora et al. 2007]. Since then, a number of new drugs or classes of drugs have emerged for the treatment of LUTS related to BPH, new data have emerged on medical therapy (monotherapies and combination therapies), new surgical techniques have come into practice, and our understanding of disease pathogenesis has increased. Consequently, a new update of the guidelines has become necessary. This article provides a summary of the updated guidelines. Only key studies are included, with the full list provided in the online version [AURO.it, 2011].
Scope and characteristics of the guidelines
The focus of the guidelines is LUTS that are considered to be related to BPH (LUTS/BPH); they do not cover LUTS that are secondary to other pathologies. LUTS secondary to BPH include symptoms associated with bladder storage and bladder voiding, and also the postmicturition period [Abrams et al. 2003]. The guidelines are intended to assist physicians and patients in the decision-making process regarding the management of LUTS/BPH, and support the process of continuous improvement of the quality of care and services to patients.
Target population
The target population is men with LUTS considered related to uncomplicated BPH.
Intended users
Intended users are clinicians involved in various aspects of LUTS/BPH management, including general practitioners, urologists, geriatricians, specialists in internal medicine, radiologists; members of organisations/health managers who are involved in the continuous improvement of the quality of care and patient empowerment; and decision makers in the public and private health service.
Development commission
Core panel comprising members of AURO.it (www.auro.it), in collaboration with the Italian Association of Family Physicians (www.aimef.org), individual geriatricians, radiologists and healthcare administrators.
Planned time of next update
The next update is planned to be carried out not more than 5 years from the current revision.
Methodology
The literature research was conducted in accordance with recommendations from the Centre for Reviews and Dissemination, University of York, UK. The quality of evidence and strength of recommendations was determined according to the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework [Guyatt et al. 2008a, 2008b, 2008c]. Lastly, the final report was prepared according to the recommendations of the Conference on Guidelines Standardization [Shiffman et al. 2003].
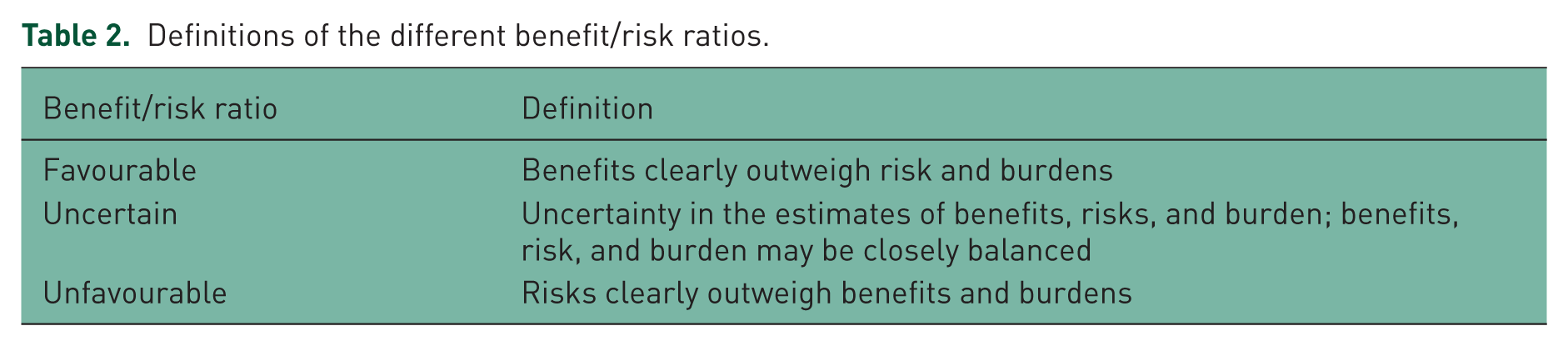
The commission defined the scope of the guidelines, the clinical questions, other relevant aspects (populations, interventions, outcomes, acceptable study designs), and literature search strategies. The following databases were searched: Medline, Embase, CRD database, NHS Economic Evaluation Database, Health Technology Assessment Database. Specific search strategies were defined for each of the following areas: risk factors for disease progression; watchful waiting (WW); lifestyle modifications; medical therapy with α blockers; medical therapy with 5α-reductase inhibitors (5ARIs); medical therapy with anticholinergics; medical therapy with phosphodiesterase-5 (PDE5) inhibitors; alternative medical therapies; combination therapies; surgical therapy; laser therapy; minimally invasive therapy; acute urinary retention; follow up following medical therapy; follow up following surgical therapy. Additional sources of information included Cochrane Library, European Association of Urology and American Urological Association (AUA) congress abstracts, ClinicalTrials.gov, and all literature reviewed for the production of the previous guidelines and revisions. Searches were restricted to the timeframe of 1 August 2006 to 12 December 2010. Publications before or after this timeframe were considered only if they were recognised as important milestones in the field or if the literature search did not identify publications within this timeframe. Each article identified was evaluated by two members of the commission, who applied an agreed checklist to select articles for further evaluation. Data on the effectiveness and adverse events (AEs) were extracted from selected records and summarised in an evidence profile. Extracted data and evidence profiles were reviewed by the commission for inclusion/exclusion; for included articles, the quality of evidence was assigned by the commission (evidence profiles are available in Italian in the extended online version of the guidelines [AURO.it, 2011]). The GRADE methodology framework was applied to rate the quality of evidence presented and grade the strength of treatment recommendations (Table 1) [Guyatt et al. 2008a, 2008b, 2008c]. Flow charts were defined for medical and surgical therapy that described the current standard therapeutic pathways at the commencement of work to update the guidelines; this enabled identification of decision points, and the definition of relevant clinical questions based on the PICOT (Population, Intervention, Comparison, Outcome of interest, Type of study) system. Outcomes were identified and their importance classified as important and essential (score 7–9), important but not essential (score 4–6), or not important (score 1–3) based on the votes of the core panel. On the basis of this classification, outcomes were given greater or lesser consideration in the literature review and subsequent formulation of recommendations. For each intervention, the commission voted on the strength of recommendation (applying previously published rules) [Schünemann et al. 2006] and also the benefit/risk ratio (see Table 2 for definitions). A total of 2328 papers/abstracts were identified by the literature search: 1690 of these were extracted, 1357 were eliminated with reason, and 333 were assessed.
GRADE system used to rate the quality of evidence and grade the strength of recommendations.

Definitions of the different benefit/risk ratios.
Discrepancies between current clinical practice and scientific evidence, and any controversies identified in the literature, were discussed and voted on at a consensus conference in June 2011 attended by 69 delegates (including urologists, geriatricians, health decision makers, general practitioners, epidemiologists, methodologists, representatives of complementary medicine, patient representatives and a judge). The outcomes of the discussions and consensus votes were considered by the commission when developing/revising draft guidelines. The guidelines underwent revision by a multidisciplinary group of professionals (recognised as experts in their respective fields) who had not participated in their development, including urologists, geriatricians, general practitioners and health economists.
The commission felt strongly that decisions on therapeutic intervention should be based on the impact of symptoms on QoL rather than the severity of symptoms (International Prostate Symptom Score (IPSS) score). A threshold for intervention was therefore set based on the IPSS Q8, with intervention recommended for patients with an IPSS Q8 score of at least 4. The commission also regarded it as important that recommendations were written in such a way as to include information on the following parameters (Figure 1): target population; intervention; recommendation; description of patients in whom the treatment can be a therapeutic option (when applicable); strength of recommendation; statement on the quality of evidence; opinion of the benefit/risk ratio.
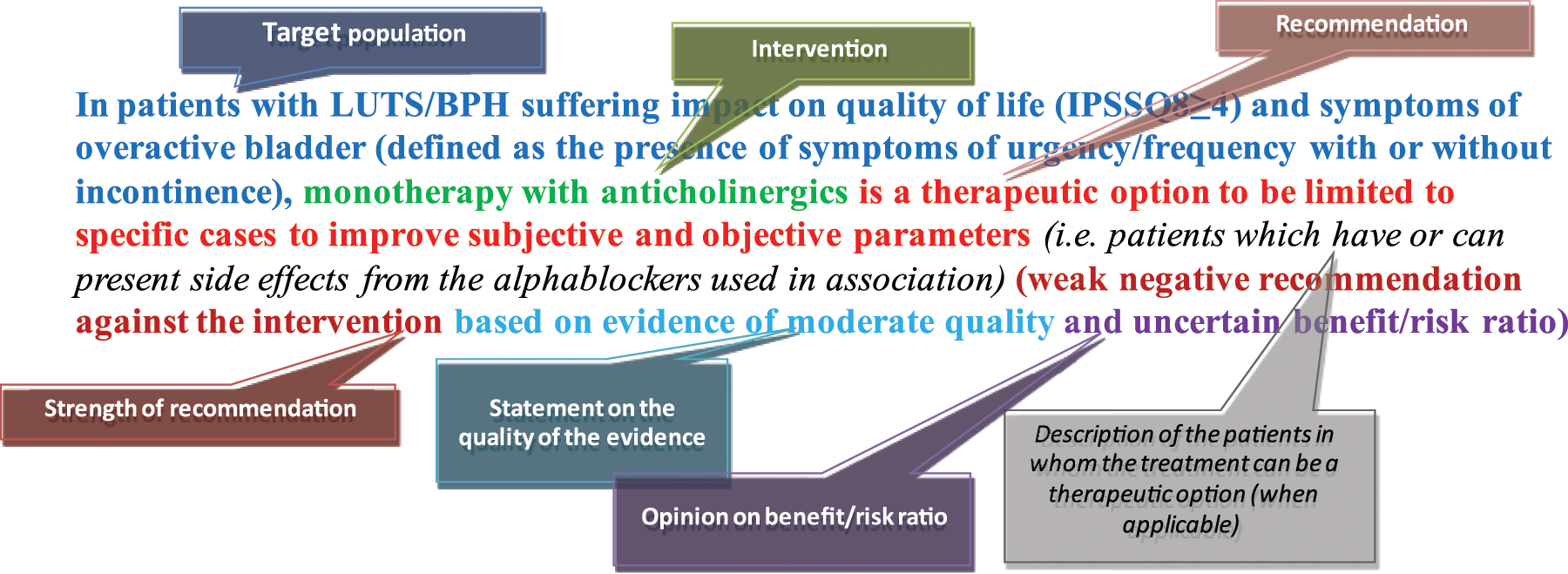
Structure of each recommendation.
Progression of lower urinary tract symptoms/benign prostatic hyperplasia
The commission defined BPH progression a priori as the appearance of one of the events considered to be an index of its progression. The indices of progression are: worsening of symptoms (increase of three points in the IPSS); any deterioration of QoL score; acute urinary retention (AUR); recurrent urinary tract infection; urinary incontinence; formation of calcium deposits in the bladder; obstructive renal insufficiency; BPH-related surgery.
Based on the quality of evidence found in the literature, the commission suggests the following in relation to progression of LUTS/BPH. Prostate-specific antigen (PSA), prostate volume and age can be considered as risk factors for progression, and should be taken into consideration when making therapeutic choices (quality of evidence, low). Maximal urinary flow rate (Qmax), symptom severity, postvoiding residual urine volume and prostate inflammation should not be considered as risk factors for BPH progression (quality of evidence, low). The commission was unable to express a judgement on the use of other parameters as risk factors for BPH progression due to lack of evidence.
Conservative treatment of lower urinary tract symptoms/benign prostatic hyperplasia
Watchful waiting
In a study comparing WW and transurethral resection of the prostate (TURP) in men with moderate BPH symptoms (n = 556), those who underwent surgery had improved bladder function compared with the WW group [Flanigan et al. 1998]. At the 5-year follow-up, 26% of the WW group had therapeutic failure, 4% had severe symptoms and 5.8% had AUR; in the TURP group, 10% had therapeutic failure, 0.3% had severe symptoms and 0.4% had AUR. A second study compared WW with a program of lifestyle changes in men with moderate to severe LUTS and compromised QoL [Brown et al. 2007]. Lifestyle changes significantly reduced the frequency of treatment failure and severity of urinary symptoms.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, WW should not be considered as a treatment for improving subjective and objective parameters (strength of recommendation, strong negative; quality of evidence, very low; unfavourable benefit/risk ratio).
Lifestyle changes
A multidisciplinary panel developed a self- management program of lifestyle and behavioural interventions for men with uncomplicated LUTS/BPH [Brown et al. 2004]. This program has been compared with WW in a randomised, controlled trial, and was shown to be associated with significantly reduced frequency of treatment failure and improvement in urinary symptoms [Brown et al. 2007].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, changes in lifestyle are a therapeutic option that might be taken into consideration for the improvement of subjective and objective parameters (strength of recommendation, weak positive; quality of evidence, low; favourable benefit/risk ratio).
Medical (drug) treatment of lower urinary tract symptoms/benign prostatic hyperplasia
α Blockers
All α blockers have similar efficacy for improving symptoms, QoL and Q max when used at appropriate doses [AUA, 2010; Chapple et al. 2011]. Long-term studies show that α blockers significantly reduce the risk of symptom deterioration, but have no effect on other BPH progression events such as AUR or BPH-related surgery [McConnell et al. 2003; Roehrborn et al. 2010; Lepor, 2007; Roehrborn, 2008].
The major AEs associated with α blockers are orthostatic hypotension, dizziness, headache, asthenia, nasal congestion and ejaculation problems; vasodilating effects appear to be more common with doxazosin and terazosin than with other α blockers [Oelke et al. 2011; Roehrborn, 2009]. Ejaculation problems appear to be more common with tamsulosin and silodosin (Table 3).
Ejaculation disorders reported for tamsulosin and silodosin.

EjD, ejaculatory dysfunction.

Treatment algorithm for medical therapy.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with tamsulosin, alfuzosin, or silodosin is an option that can be taken into consideration for the improvement of subjective and objective parameters (strength of recommendation, weak positive; quality of evidence, high; favourable benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with α blockers is a therapeutic option that should be reserved for particular cases in order to reduce the risk of AUR, BPH-related surgery, worsening of QoL and worsening of symptoms (i.e. patients in whom only the reduction of worsening of symptoms is important) (strength of recommendation, weak negative; quality of evidence, high; uncertain benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with doxazosin or terazosin is a therapeutic option that should be limited to specific patients (i.e. those in whom possible hypotensive effects will not cause clinical problems) (strength of recommendation, weak negative; quality of evidence, moderate; uncertain benefit/risk ratio).
Recommendation Due to incompleteness of literature data, the commission is unable to express a judgement on the differences in benefit/risk between the different α blockers (strength of recommendation, not applicable; quality of available evidence, moderate/high; uncertain benefit/risk ratio).
5α-reductase inhibitors
In placebo-controlled studies, finasteride improved symptom scores by 0.6–2.2 points, and improved Q max by 0.2–1.7 ml/s [Gormley et al. 1992; Tammela and Konturri, 1995; Andersen et al. 1995; Nickel et al. 1996; Marberger, 1998; McConnell et al. 1998]. These benefits of finasteride are greater in men with larger prostate volumes (≥30–40 ml) and higher PSA levels (>1.4 ng/ml), with the greatest effects after 12 months of treatment [Boyle et al. 1996; Roehrborn et al. 1999; Kaplan et al. 2011]. Fewer data exist on QoL benefits, with reported improvements modest and at the limit of significance [Bruskewitz et al. 1999; Lepor et al. 1998; Lowe et al. 2003]. After 2–4 years’ treatment, finasteride reduced the risk of AUR by 34–57% and the risk of BPH surgery by 40–55%, with the magnitude of benefit related to treatment duration and risk factors for BPH progression (prostate volume and PSA) [Marberger, 1998; McConnell et al. 1998].
In a combined analysis of three randomised, placebo-controlled trials in men with prostate volume at least 30 ml and PSA at least 1.5 ng/ml, dutasteride significantly improved symptoms, QoL (BPH impact index), and Q max compared with placebo [Roehrborn et al. 2002; O’Leary et al. 2003]. Compared with placebo, dutasteride reduces the relative risk of AUR and BPH-related surgery by 57% and 48% (both p < 0.001). For both outcomes, the risk reduction appears to be greater in men with prostate volume greater than 40 ml than in men with prostate volume of 30–40 ml [Gittelman et al. 2006].
5ARIs are associated with sexual adverse effects (altered libido, erectile dysfunction, reduced ejaculation volume), particularly during the first year of treatment [Lowe et al. 2003; Wessels et al. 2003; Andriole and Kirby, 2003; Debruyne et al. 2004].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with finasteride is a therapeutic option that should be limited to selected cases to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, moderate; uncertain benefit/risk ratio); it is a therapeutic option that can be taken into consideration to reduce the risk of AUR, BPH-related surgery, worsening of QoL and/or worsening of symptoms in men with prostate volume greater than 30–40 ml (strength of recommendation, weak positive; quality of evidence, moderate; favourable benefit/risk ratio).
Recommendation In patients with LUTS/BPH, IPSS Q8 of at least 4 and prostate volume greater than 30 ml, monotherapy with dutasteride is a therapeutic option that can be taken into consideration to improve subjective and objective parameters (strength of recommendation, weak positive; quality of evidence, high; uncertain benefit/risk ratio), and to reduce the risk of AUR, BPH-related surgery, worsening of QoL and/or worsening of symptoms in men with prostate volume greater than 30–40 ml (strength of recommendation, weak positive; quality of evidence, high; favourable benefit/risk ratio).
Recommendation Due to the absence of reliable data, the commission is unable to express a judgement on the differences in benefit/risk between the different 5ARIs.
Anticholinergics
A randomised, placebo-controlled trial was identified that assessed tolterodine extended release (ER), tamsulosin or both in men with LUTS (IPSS ≥ 12) and overactive bladder [Kaplan et al. 2006]. In this study, monotherapy with tolterodine ER was not significantly different to placebo in terms of changes in IPSS total score, IPSS Q8 score or Qmax. The most common AE with tolterodine monotherapy was xerostomia.
Other studies have reported a potential worsening of cognitive disturbances in older patients treated with anticholinergics [Schiefe and Takeda, 2005; Landi et al. 2007; Ancelin et al. 2006]. On the basis of these reports, an anticholinergic with low haematoencephalic barrier permeability should be considered for the treatment of older patients.
Recommendation In patients with LUTS/BPH, IPSS Q8 of at least 4 and symptoms of overactive bladder (defined as the presence of symptoms of urgency/frequency with or without incontinence), monotherapy with an anticholinergic is a therapeutic option to be limited to specific cases to improve subjective and objective parameters (i.e. patients who have or are at risk of side effects from α blockers used in association) (strength of recommendation, weak negative; quality of evidence, moderate; uncertain benefit/risk ratio).
Phytotherapies
In a double-blind, randomised, placebo-controlled trial (n = 85), Serenoa repens (hexane extracted) resulted in a statistically significant improvement in urinary symptom score (4.4 versus 2.2, p = 0.038) but had no measurable effect on urinary flow rate [Gerber et al. 2001]. A meta-analysis of all available published trials did show a significant improvement in Qmax (2.2 ml/s versus 1.2 ml/s, p = 0.042) compared with placebo [Boyle et al. 2004]; trials included in this analysis were considered to be of low or very low quality. In another double-blind, randomised, placebo-controlled trial (n = 225), S. repens (CO2 extracted) did not improve symptoms or objective measures of BPH [Bent et al. 2006].
A meta-analysis of studies of Pygeum africanum concluded that it may be a useful treatment option for men with BPH/LUTS, although the quality of included studies was very low [Wilt et al. 2002]. Men treated with P. africanum were more likely to report symptom improvement than those who received placebo; episodes of nocturia, residual urine volume and Qmax were also improved.
A low-quality randomised, double-blind, parallel-group study of mepartricin has indicated improvements compared with placebo in symptom and QoL scores, and Qmax [Denis et al. 1998]. However, at 6 months the improvements in objective parameters with mepartricin were not statistically significant compared with placebo.
The combination of S. repens (other extracts) and Urtica dioica has been shown to significantly improve symptom score compared with placebo in a randomised, double-blind study [Lopatkin et al. 2005]. This study was considered to be of low quality due to limited internal validity.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with S. repens (hexane extracted) is a treatment option to be limited to specific cases to improve subjective and objective parameters (e.g. patients who wish to be treated with phytotherapy) (strength of recommendation, weak negative; quality of evidence, very low; uncertain benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with S. repens (other extracts) is a treatment option that should not be taken into consideration to improve subjective and objective parameters (strength of recommendation, strong negative; quality of evidence, high; unfavourable benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with P. africanum and mepartricin should not be considered a treatment to improve subjective and objective parameters (strength of recommendation, strong negative; quality of evidence, low to very low; uncertain benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, the combination of S. repens (other extracts) and U. dioica is a treatment option that should be limited to selected cases (e.g. patients who wish to be treated with phytotherapy) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, low; uncertain benefit/risk ratio).
Phosphodiesterase-5 inhibitors
In a 12-week dose-finding study, tadalafil significantly improved LUTS, erectile function and QoL compared with placebo [Roehrborn et al. 2008a]. The frequency of AEs was dose dependent, and tadalafil 5 mg provided the best risk–benefit profile. Vardenafil and sildenafil have also been shown to significantly improve LUTS, erectile function, and QoL in 8- and 12-week randomised, double-blind, placebo-controlled studies respectively [Steif et al. 2008; McVary et al. 2007]; these studies were considered to be of low quality. AEs were higher with both vardenafil and sildenafil (13.7% and 32% respectively) compared with placebo. None of these studies showed a significant effect of PDE5 inhibitors on Qmax.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with tadalafil 5 mg is a treatment option that should be limited to selected cases to improve subjective and objective parameters (e.g. patients with LUTS/BPH and erectile dysfunction who wish to simultaneously treat both conditions) (strength of recommendation, weak negative; quality of evidence, moderate; uncertain benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monotherapy with vardenafil or sildenafil should not be considered a treatment to improve subjective and objective parameters (strength of recommendation, strong negative; quality of evidence, low; uncertain benefit/risk ratio).
Combination therapy: α blockers and 5α-reductase inhibitors
In the Medical Therapy of Prostatic Symptoms (MTOPS) study, combination therapy (finasteride plus doxazosin) significantly improved symptom score and Q max compared with placebo, and also compared with either monotherapy [McConnell et al. 2003]; it was not reported whether these improvements had an impact on QoL. The Combination of Avodart and Tamsulosin (CombAT) study specifically included men at increased risk of BPH progression (prostate volume ≥ 30 ml and PSA ≥ 1.5 ng/ml). The combination of dutasteride plus tamsulosin provided significant improvements in symptom score and Qmax compared with either monotherapy; these improvements were reflected in significant improvements in QoL measures with combination therapy compared with either monotherapy [Roehrborn et al. 2010; Montorsi et al. 2010].
Across both the MTOPS and CombAT studies, combination therapy with 5ARI plus an α blocker was more effective for preventing disease progression events (symptom progression, AUR, BPH-related surgery) compared with either monotherapy (Table 4); the reduction in risk of AUR and BPH-related surgery with combination therapy was not statistically significant compared with 5ARI monotherapy. However, the number of progression events was low in MTOPS and in the subgroup of patients with prostate volume less than 40 ml in CombAT [McConnell et al. 2003; Roehrborn et al. 2011].
Combination therapy (5α-reductase inhibitor plus α blocker) versus monotherapies: incidence and relative risk of benign prostatic hyperplasia progression events.

Source data: McConnell et al. [2003]; Roehrborn et al. [2010].
5ARI, 5α-reductase inhibitor; AUR, acute urinary retention; BPH, benign prostatic hyperplasia; CI, confidence interval; IPSS, International Prostate Symptom Score; RR, relative risk.
In patients at risk of progression, dutasteride plus tamsulosin was significantly superior to tamsulosin monotherapy at reducing the relative risk of AUR or BPH-related surgery (68% and 71%, respectively; p < 0.001); the reduction in risk of AUR and BPH-related surgery with combination therapy was not statistically significant compared with dutasteride monotherapy [Roehrborn et al. 2010]. Combination therapy was also significantly superior to both monotherapies at reducing the relative risk of BPH clinical progression. Symptom progression was reduced by 35% and 41% respectively compared with dutasteride and α-blocker monotherapy [Roehrborn et al. 2010]. The cumulative incidence of progression events (7–14%) and the absolute risk reductions (4–6%) in CombAT were clinically relevant.
AEs with combination therapy were generally similar to those for each drug alone. A combined analysis of all randomised controlled trials of 5ARI plus α-blocker combination therapy showed that differences in incidences of AEs are low, ranging from −0.2% to +2.4% for cardiovascular AEs and from +0.3% to +3% for sexual AEs (Table 5).
Combination therapy (5α-reductase inhibitor plus α blocker) versus monotherapies: cumulative incidence and relative risk of adverse events.

Source data: McConnell et al. [2003]; Roehrborn et al. [2008b]; Lepor et al. [1996]; Debruyne et al. [1998]; Kirby et al. [2003].
5ARI, 5α-reductase inhibitor; C, combination; CI, confidence interval; ED, erectile dysfunction; EjD, ejaculatory dysfunction; NS, nonsignificant; RR, relative risk.
Two studies were identified that assessed the impact of α-blocker withdrawal following a period of combination therapy [Barkin et al. 2003; Nickel et al. 2008], but were deemed to have limitations in design and methodology that impeded assessment of benefit/risk profile.
Recommendation In the general population of patients with LUTS/BPH and IPSS Q8 of at least 4, the combination of α blockers and 5ARI is a treatment option to be limited to selected cases to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, moderate; uncertain benefit/risk ratio); this combination should not be considered as a therapeutic option to reduce the risk of AUR, BPH-related surgery, worsening of QoL, or worsening of symptoms (strength of recommendation, strong negative; quality of evidence, moderate; uncertain benefit/risk ratio).
Recommendation In patients with LUTS/BPH, IPSS Q8 of at least 4 and risk of progression (defined as prostate volume > 30 ml and PSA > 1.5 ng/ml), the combination of α blockers and 5ARI is a therapeutic option recommended to improve subjective and objective parameters (strength of recommendation, strong positive; quality of evidence, high; favourable benefit/risk ratio), and to reduce the risk of AUR, BPH-related surgery, worsening of QoL or worsening of symptoms (strength of recommendation, strong positive; quality of evidence, high; favourable benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, the suspension of α blockers after a period of combination therapy is a therapeutic option that should be limited to selected cases (e.g. patients in whom control of symptoms is less important than reducing the risk of AUR and BPH-related surgery) (strength of recommendation, weak negative; quality of evidence, very low; uncertain benefit/risk ratio).
Combination therapy: α blockers and anticholinergics
Two studies were identified that assessed the combination of α blocker plus anticholinergic in patients with LUTS/BPH and overactive bladder. In one study, significantly more patients who received tolterodine ER plus tamsulosin reported treatment benefit by week 12 than patients who received placebo, tolterodine ER monotherapy, or tamsulosin monotherapy [Kaplan et al. 2006]. Significant improvements for combination therapy compared with placebo in IPSS and QoL item score were also reported. In the other study, tamsulosin combined with ER oxybutynin resulted in significantly greater improvements in IPSS (−6.9 versus −5.3; p = 0.006) and QoL (IPSS Q8: −1.3 versus − 0.8; p < 0.01) at 12 weeks compared with tamsulosin plus placebo [MacDiarmid et al. 2008]. In both studies the most frequent AE was xerostomia. As indicated previously, other studies have indicated a worsening of cognitive disturbances in older patients treated with anticholinergics [Scheife and Takeda, 2005; Landi et al. 2007; Ancelin et al. 2006].
Recommendation In patients with LUTS/BPH, IPSS Q8 of at least 4 and symptoms of overactive bladder (defined as symptoms of urgency/frequency with or without incontinence), the combination of an α blocker and anticholinergic is a therapeutic option that can be taken into consideration to improve subjective and objective parameters (strength of recommendation, weak positive; quality of evidence, high; uncertain benefit/risk ratio).
Combination therapy: α blockers and phytotherapies
Two studies were identified that have assessed the combination of tamsulosin and S. repens; one was a prospective observational study [Hizli and Uygur, 2007] and one a double-blind randomised trial [Glemain et al. 2002]. Neither showed any additional benefit of adding phytotherapy to tamsulosin. Despite the absence of data to show a benefit of this combination, it is widely used in Italy. The benefit/risk ratio was considered as uncertain/favourable by 43% of experts at the consensus conference, while 44.5% considered it to be uncertain/unfavourable.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, the combination of α blocker and phytotherapies is a therapeutic option that should be limited to selected cases to improve subjective and objective parameters (e.g. patients in receipt of α blockers who also wish to be treated with phytotherapies) (strength of recommendation, weak negative; quality of evidence, very low; uncertain benefit/risk ratio).
Surgical treatment of lower urinary tract symptoms/benign prostatic hyperplasia
Open surgery
Open surgery is associated with QoL improvements of 2–2.8 points at 18–24 months post operation [Naspro et al. 2006; Skolarikos et al. 2008]. Studies of patients with an average prostatic weight of approximately 80 g show that open surgery improves the IPSS by 11–20 points after 12 months’ follow up [Skolarikos et al. 2008; Ou et al. 2010; Suer et al. 2008; Gacci et al. 2003]; one randomised study showed an improvement of 18 points at 5-year follow-up [Kuntz et al. 2008]. A rate of early complications of 17.3% has been reported [Gratzke et al. 2007], and the technique is associated with long hospitalisation and recovery times.
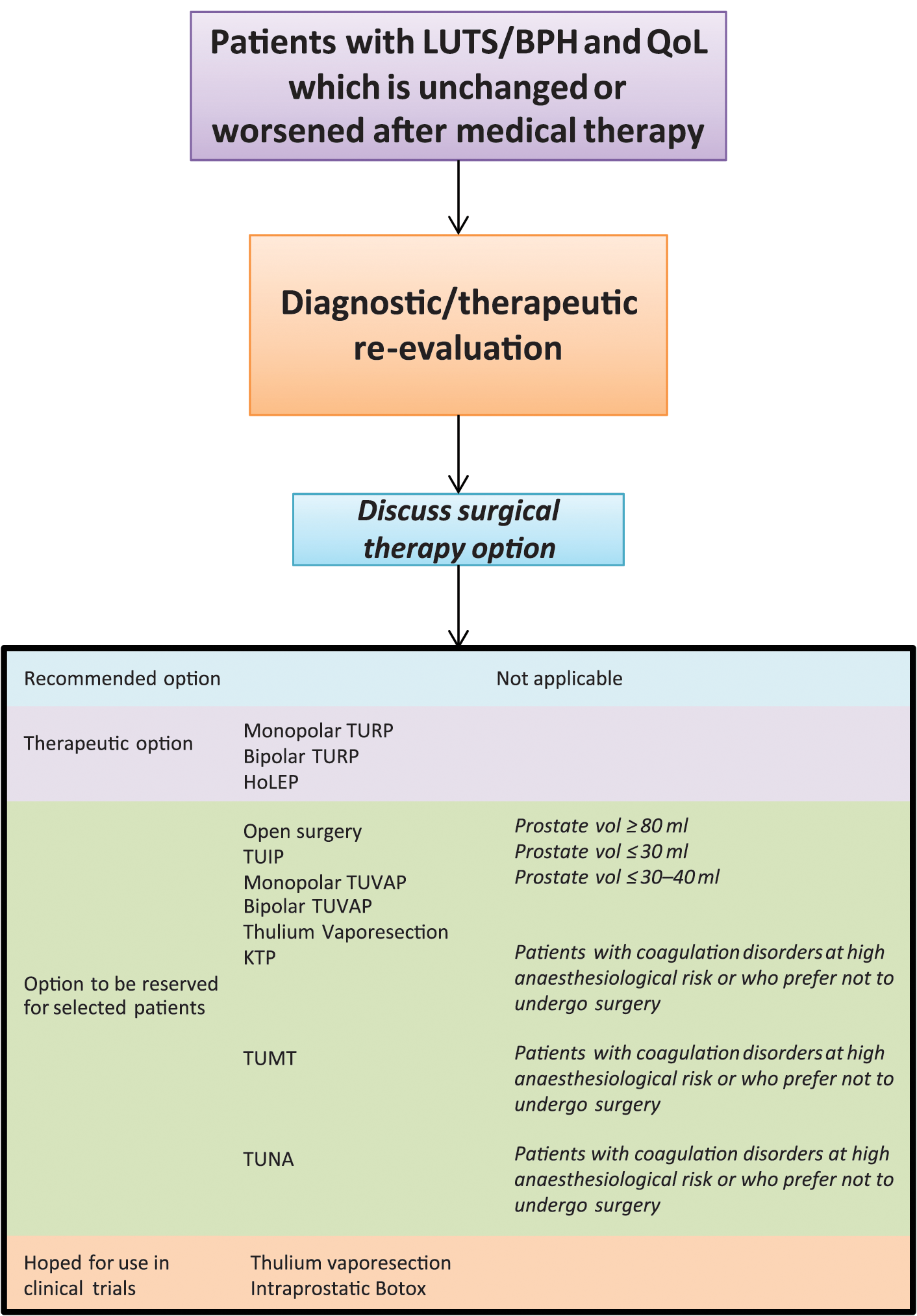
Treatment algorithm for surgical therapy.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, open surgery is a therapeutic option to be limited to selected cases (i.e. patients with prostates > 80 g; this value was established from the literature analysis and the opinions of experts at the consensus conference) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, very low; uncertain benefit/risk ratio).
Transurethral resection of the prostate
In randomised studies, monopolar and bipolar TURP provided similar improvements in QoL and symptom scores [Yang et al. 2004; Singh et al. 2005; Seckiner et al. 2006; Iori et al. 2008; Autorino et al. 2009; Kong et al. 2009; Singhania et al. 2010; Nuhogğlu et al. 2006; Patankar et al. 2006; Erturhan et al. 2007; Ho et al. 2007; Yoon et al. 2006; Chen et al. 2010; Bhansali et al. 2009]. In observational studies, QoL improvements of 2.4–4.4 points have been reported for monopolar TURP after 12 years’ follow up [Mishriki et al. 2008; Masumoiri et al. 2010]. Complication rates are slightly higher with monopolar TURP than with the bipolar procedure [Ahyai et al. 2010].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monopolar TURP is a therapeutic option that can be taken into consideration to improve subjective and objective parameters (strength of recommendation, weak positive; quality of evidence, low; favourable benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, bipolar TURP is a therapeutic option that can be taken into consideration to improve subjective and objective parameters (strength of recommendation, weak positive; quality of evidence, low; favourable benefit/risk ratio).
Transurethral incision of the prostate
QoL and symptom improvements with transurethral incision of the prostate (TUIP) have been shown in randomised trials (average prostatic weight approximately 30 g) to be not significantly different to those with monopolar TURP [Tkocz and Prajsner, 2002; Larsen et al. 1987; Dørflinger et al. 1992; Riehmann et al. 1995; Saporta et al. 1996; Jahnson et al. 1998]. Intra- and postoperative complication rates with TUIP are generally similar to those with TURP; reintervention rate is significantly higher with TUIP than with TURP, while ejaculatory dysfunction is significantly lower [Lourenco et al. 2010].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, TUIP is a therapeutic option that should be limited to selected cases (i.e. patients with prostates < 30 g; this value was established from the literature analysis and the opinions of experts at the consensus conference) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, low; uncertain benefit/risk ratio).
Transurethral electrovaporisation of the prostate
Three randomised trials comparing monopolar transurethral electrovaporisation of the prostate (TUVAP) and TURP in patients with prostate size 30–40 g were identified [Hammadeh et al. 2003; Gallucci et al. 1998; Nuhogğlu et al. 2005]. The two procedures provided similar improvements in QoL and symptom score, and rates of complications and reintervention for BPH were also generally similar (except for AUR due to clotting, which was significantly lower with TUVAP than with TURP).
Four randomised studies comparing bipolar TUVAP and TURP were identified; across all the studies the maximum prostate size was 80 g [Geavlete et al. 2010; Hoekstra et al. 2010; Hon et al. 2006; Kaya et al. 2007]. Improvements in QoL score and IPSS were similar for the two procedures. Rates of complications and reintervention for BPH were also similar, except for significantly lower rates of capsule perforation and AUR due to clotting with TUVAP. There are, as yet, insufficient data to determine the medium- to long-term benefits of bipolar TUVAP. A potential issue with bipolar TUVAP is the risk of urethral stenosis due to the use of high-calibre endoscopic instruments.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, monopolar TUVAP is a therapeutic option that should be limited to certain cases (i.e. patients with small- to medium-volume prostates (<30–40 g); this value was established from the literature analysis and the opinions of the commission) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, low; uncertain benefit/risk ratio).
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, bipolar TUVAP is a therapeutic option that should be limited to selected cases (e.g. patients with prostates of 60–80 g (this value was established from the literature analysis and the opinions of the commission) or patients with coagulation problems or taking anticoagulant medication) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, low; uncertain benefit/risk ratio).
Laser treatment of lower urinary tract symptoms/benign prostatic hyperplasia
Holmium laser enucleation of the prostate
Holmium laser enucleation of the prostate (HoLEP) provides similar improvements in QoL score (2.6- to 3.6-point improvement compared with baseline) to open surgery and TURP over 2 years’ follow up [Naspro et al. 2006; Wilson et al. 2006], and similar improvements in IPSS over 5–6 years [Kuntz 2006]. Complication rates with HoLEP are generally similar to rates with open surgery or TURP; catheterisation time and duration of hospital stay appear to be shorter with HoLEP [Naspro et al. 2006; Kuntz et al. 2008; Wilson et al. 2006; Neill et al. 2006; Ahyai et al. 2007]. Despite favourable results obtained with HoLEP, relatively few centres are competent in what is a technically challenging procedure.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, HoLEP is a therapeutic option to be taken into consideration to improve subjective and objective parameters (strength of recommendation, weak positive; quality of evidence, moderate; favourable benefit/risk ratio).
Thulium laser
A single, prospective randomised study was identified that compared thulium vaporesection and standard TURP in patients with symptomatic BPH, with follow up of 12 months [Xia et al. 2008]. No differences were observed between the two treatments in terms of symptom improvement and urodynamic findings. Thulium laser resection was associated with significantly shorter catheterisation times and duration of hospital stay, while the rate of late complications was similar in the two groups. An observational study (deemed to be very low quality) has indicated that the benefits of thulium vaporesection are maintained over a follow-up period greater than 12 months [Bach et al. 2010].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, thulium vaporesection is a therapeutic option that should be limited to selected cases (e.g. patients treated in centres highly trained in the technique) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, low; uncertain benefit/risk ratio).
Recommendation The commission and consensus conference agree that currently available data are limited and of very low quality. Based on this, and the uncertain benefit/risk ratio, the commission is unable to express a clinical recommendation for the use of thulium laser vapoenucleation to improve subjective and objective parameters in patients with LUTS/BPH; it is hoped that more data on the procedure will be provided by future randomised clinical trials (quality of evidence, very low; uncertain benefit/risk ratio).
Potassium titanyl-phosphate laser
Data from randomised clinical trials indicate that improvements in QoL and symptom scores with potassium titanyl-phosphate (KTP) laser treatment are similar to those with open surgery and monopolar TURP [Skolarikos et al. 2008; Bouchier-Hayes et al. 2009; Al-Ansari et al. 2010]. Improvements in symptom scores and QoL appear to be maintained during follow up of up to 3 years [Al-Ansari et al. 2010]. KTP laser treatment results in shorter catheterisation times and duration of hospital stay compared with open surgery or TURP, although the reported reintervention rate is higher with the laser therapy [Skolarikos et al. 2008; Bouchier-Hayes et al. 2009; Al-Ansari et al. 2010; Horasanli et al. 2008; Tugcu et al. 2008].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, the KTP laser is a therapeutic option that should be limited to selected cases (e.g. patients with blood coagulation disorders, or at high cardiovascular and anaesthesiologic risk) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, low; uncertain benefit/risk ratio).
Minimally invasive therapies for lower urinary tract symptoms/benign prostatic hyperplasia
Transurethral microwave thermotherapy
Improvements in QoL with transurethral microwave thermotherapy (TUMT) may be lower than with TURP, especially with longer-term follow up [D’Ancona et al. 1998; de la Rosette et al. 2003; Mattiasson et al. 2007]. Data on symptom improvement are inconsistent, with one study showing similar improvements with TUMT and TURP and another suggesting greater benefit with TURP [D’Ancona et al. 1998; de la Rosette et al. 2003]. Reported rates of postoperative complications such as AUR and urinary tract infection are higher with TUMT than with TURP, as is the reintervention rate [D’Ancona et al. 1998; de la Rosette et al. 2003; Mattiasson et al. 2007].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, TUMT is a therapeutic option that should be limited to selected cases (e.g. patients with blood coagulation disorders, at high anaesthesiologic risk or who prefer not to undergo surgery) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, moderate; uncertain benefit/risk ratio).
Transurethral needle ablation
Long-term (5- and 7-year follow-up) data are available from prospective, randomised trials comparing transurethral needle ablation (TUNA) and TURP [Hill et al. 2004; Chandraskar et al. 2003]. These studies indicate good durability of improvement in symptom score and QoL with TUNA. Although the improvements appear to be less than those obtained with TURP, TUNA is associated with a lower risk of AEs. TUNA is also associated with a shorter duration of hospitalisation than TURP, although the reintervention rate is higher [Hill et al. 2004; Chandraskar et al. 2003].
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, TUNA is a therapeutic option that should be limited to selected cases (e.g. patients with blood coagulation disorders, at high anaesthesiologic risk or who prefer not to undergo surgery) to improve subjective and objective parameters (strength of recommendation, weak negative; quality of evidence, moderate; uncertain benefit/risk ratio).
Intraprostatic Botox
A review of seven studies of Botox, deemed to be of very low quality, suggests QoL and symptom score improvements of 1.3 and 11 points respectively after 11 months’ follow up compared with preoperative scores [Chartier-Kastler et al. 2011]. The rate of postoperative AUR was reported as 10%.
Recommendation The commission is unable to make a recommendation due to the lack of available data; randomised clinical studies are urgently needed.
Prostatic stent
Two systematic reviews are available that have assessed use of an epithelialising stent [Armitage et al. 2007] and a thermo-expandable metallic stent [Armitage et al. 2006]. In both reviews, improvements in symptoms and Qmax were noted, however high rates of failures and stent removal were reported.
Recommendation In patients with LUTS/BPH and IPSS Q8 of at least 4, prostatic stents are a therapeutic option that should not be taken into consideration to improve subjective and objective parameters (strength of recommendation, strong negative; quality of evidence, very low; unfavourable benefit/risk ratio).
Follow up of patients treated for lower urinary tract symptoms/benign prostatic hyperplasia
Patients on medical (drug) therapy
There are limited, very low quality data available on which to base recommendations about the optimal follow-up process for patients receiving drug treatment for LUTS/BPH. A schedule of follow-up appointments has been proposed by the commission and approved by the consensus conference of experts (Table 6).
Proposed follow-up schedule for patients treated with medical therapy.

5ARI, 5α-reductase inhibitor; PDE5, phosphodiesterase 5.
Patients undergoing invasive therapy
There is a lack of information in the literature on which to base recommendations for the follow up of patients who have received invasive therapy. A schedule of follow-up appointments has therefore been proposed by the commission and approved by the consensus conference of experts (Table 7).
Proposed follow-up schedule for patients treated with invasive therapy.

Management of acute urinary retention
Data were assessed from three randomised, controlled trials of α blockers in men with AUR secondary to BPH who had been catheterised [Lucas et al. 2005; McNeill and Hargreave, 2004; Prieto et al. 2008]. Across the three studies, 53% of men who also received an α blocker had a successful trial without catheter, compared with 39% of men who were catheterised without the addition of an α blocker (Table 8). Compared with catheterisation alone, the relative risk of spontaneous micturition recovery in men who also received an α blocker was 1.4 (95% confidence interval 1.14–1.68, p < 0.001). Across the studies, there was wide variation in the duration of catheterisation and α-blocker treatment such that no conclusions can be drawn on the ideal length of each treatment.
Catheter versus catheter plus α blockers: relative risk of recatheterisation.

CI, confidence interval; RR, relative risk.
Recommendation Combining bladder catheterisation and α-blocker therapy is an option that can be taken into consideration to manage BPH-related AUR (strength of recommendation, weak positive; quality of evidence, very low; favourable benefit/risk ratio).
Recommendation Bladder catheterisation alone is a therapeutic option that should be limited to selected cases, such as patients who are unable to tolerate α-blocker therapy (strength of recommendation, weak negative; quality of evidence, very low; uncertain benefit/risk ratio).
Summary
These updated guidelines reflect the emergence in recent years of new drugs or classes of drugs for the treatment of LUTS related to BPH, new data on medical therapies (monotherapies and combination therapies), and new surgical techniques. As with our previous recommendations [Spatafora et al. 2007], decisions on therapeutic intervention are based on the impact of symptoms on QoL, rather than the severity of symptoms. Unlike our previous recommendations, a threshold for intervention was set based on the IPSS Q8, with intervention recommended for patients with an IPSS Q8 score of at least 4. This represents a divergence from other LUTS/BPH guidelines, which recommend interventions on the basis of symptom severity [AUA, 2010; Oelke et al. 2011].
Another distinction between the present update and our previous update is the application of the GRADE methodology framework to rate the quality of evidence presented and grade the strength of treatment recommendations [Guyatt et al. 2008a–c]. GRADE is considered to be the best methodology for the development of clinical practice guidelines, and the most widely used by major scientific/medical associations around the world.
In addition to differences in the philosophy and methodology behind our guidelines compared with others in the field, there are a number of differences in clinical recommendations that have emerged due to interpretation of the literature or availability of new information. For example, combination therapy with a 5ARI plus an α blocker is the recommended option for the treatment of patients at risk of BPH progression, rather than just a therapeutic option. This is based on greater improvement in QoL compared with monotherapies, and the commission’s belief that the absolute reduction in the risk of AUR or BPH-related surgery is clinically relevant in the group of patients with enlarged prostates. Other differences in clinical recommendations include the warning of potential worsening of cognitive disturbances with use of anticholinergics in older patients, the distinction between S. repens preparations (according to the method of extraction), and the clearly defined threshold of prostate size for performing open surgery (>80 g).
While the recommendations included in these guidelines are evidence based, there are also other factors to consider when making treatment decisions. In addition to the research evidence, clinical decisions should be informed by patients’ clinical and physical circumstances, as well as patients’ preferences and actions [Haynes et al. 2002]. Clinical expertise is also needed to bring these three aspects together and recommend a treatment that is acceptable to the patient.
Implementation of any guidelines can present challenges, and will require a collective effort. Previous experience suggests that small-group local meetings between general practitioners and urologists, in which best practice is discussed and shared, can be useful in promoting at least some changes to clinical practice. As previously described [Spatafora et al. 2007], collaboration between local administrators and all clinicians involved in BPH management in each local health unit will also be central to facilitating adoption of these guidelines.
Footnotes
Acknowledgements
Medical writing support for the development of this manuscript was provided by Tony Reardon of Spirit Medical Communications. We are grateful to the following members for their participation in the development of the guidelines.
Consultants: Nunzio Costa, general practitioner, Stornarella-FG; Federica Marchesotti, urologist, Casale Monferrato-AL; Giorgio Mazzi, health decision maker, Reggio Emilia; Giorgio Napodano, urologist, Nocera Inferiore-SA; Afro Salsi, geriatrician, Bologna; Domenico Viola, urologist, Reggio Emilia
Reviewers: Carlo Adriano Biagini, geriatrician, Pistoia; Massimo Brunetti, health economist, Modena; Salvatore Campo, general practitioner, Palermo; Giario Conti, urologist, Como; Paolo Gontero, urologist, Turin; Giovanni Muto, urologist, Turin; Arcangelo Pagliarulo, urologist, Bari; Furio Pirozzi Farina, urologist, Sassari; Tommaso Prayer Galletti, urologist, Padua; Domenico Prezioso, urologist, Naples; Paolo Puppo, urologist, Genoa; Alessandro Sciarra, urologist, Rome; Andrea Tubaro, urologist, Rome
Funding
The preparation of these guidelines was supported by an unrestricted educational grant from GlaxoSmithKline. Funding for medical writing support for the development of this manuscript was provided by the Italian Association of Urologists.
Conflict of interest statement
SS has received consulting fees from GSK and Nycomed, and support for congress participation from GSK; AC has received consulting fees from Eli Lilly and Pfizer, and support for congress participation from GSK and Astellas; AF has received consulting fees from GSK, and support for congress participation from Sigma Tau and Pierre Fabre; CG has received support for congress participation from Sanofi-Aventis; RH has received support for congress participation from GSK; EM and CN have no relevant conflicts to declare; MP has received consulting fees from GSK and Nycomed, and support for congress participation from GSK, Nycomed and Bayer; RS has received consulting fees from GSK and Nycomed, research funding from Janssen-Cilag, and support for congress participation from GSK, Nycomed, Teleflex, Johnson & Johnson and Pierre Fabre; GLP has received consulting fees from Pfizer, Merck-Sorono, Bayer, Eli Lilly and IBSA, and support for congress participation from GSK.