
Abstract
Erectile dysfunction (ED) is one of the complications associated with pelvic surgery. The significance of ED as a complication following pelvic surgery, especially radical prostatectomy (RP), lies in the negative impact that it has on patients’ sexual and overall life. In the literature, rates of ED following RP range from 25% to 100%. Such variety is associated with pelvic dissection and conservation of neurovascular structures. Another important factor impacting on postoperative ED is the preoperative erectile function of the patient. Advances in the knowledge of pelvic anatomy and pathological mechanisms led to a refinement of pelvic surgical techniques, with attention to the main structures that if damaged compromise erectile function. These improvements resulted in lower postoperative ED rates and better erectile recovery, especially in patients undergoing RP. Furthermore, surgery alone is not sufficient to prevent this complication, and thus, several medical strategies have been tested with the aim of maximizing erectile function recovery. Indeed it seems that prevention of postoperative ED must be addressed by a multimodal approach. The aim of this review is to give a picture of recent knowledge, novel techniques and therapeutic approaches in order to reach the best combination of treatments to reduce the rate of ED after pelvic surgery.
Introduction
Prostate cancer, radical prostatectomy, and erectile dysfunction
Radical prostatectomy (RP) in any form (open, laparoscopic, or robotic) is the most frequently performed procedure for patients with localized prostate cancer (PCa) and a life expectancy greater than 10 years. The goal of RP is to eradicate disease while preserving continence and potency whenever possible [Cooperberg et al. 2004; Bianco et al. 2005; Stanford et al. 2000; Heidenreich, 2008]. Erectile dysfunction (ED) is defined as the inability to develop and maintain an erection for satisfactory sexual intercourse or activity in the absence of an ejaculatory disorder. Research data have shown that about 25–90% of men undergoing RP experience postoperative ED [Walsh et al. 2000; Mulhall et al. 2010; Anastasiadis et al. 2003; Fowler et al. 1993; Goeman et al. 2006; Kundu et al. 2004; Litwin et al. 1999; Menon et al. 2007; Rabbani et al. 2000; Rozet et al. 2005; Sanda et al. 2008]. Such discrepancies in the statistics may be due to the lack of a standardized and agreed-on definition of postoperative ED recovery [Schover et al. 2002; Mulhall et al. 2009; Matthew et al. 2005]. Moreover a recent review by Burnett and colleagues has underlined the need to apply well defined rigorous procedures for future studies on this subject, due to inconsistency and diversity of literature results [Burnett et al. 2007]. It should be taken in consideration that minimally invasive techniques decrease postoperative hospital stay and have comparable oncological outcomes compared with open surgery for experienced surgeons [Bivalacqua et al. 2010]. However the risk of incontinence and ED with minimally invasive techniques may not be improved versus open surgery [Hu et al. 2009]. Furthermore, the impact of sexual dysfunction is greater than that of incontinence [Arai et al. 1999] and can have a significant negative impact on quality of life [Litwin et al. 1999].
Because preoperative potency is a major factor associated with the recovery of erectile function after surgery, patients being considered for a nerve-sparing radical prostatectomy (NSRP) should ideally be potent [Montorsi et al. 2004]. However, Briganti and colleagues demonstrated that, the current classification according to the International Index of Erectile Function (IIEF) is not completely reliable in the sexual function evaluation of patients affected by PCa waiting for RP because of the psychogenic influences that may strongly alter patients’ sexual life preoperatively. So they proposed to eliminate this bias by administering the IIEF questionnaire at the time of biopsy [Briganti et al. 2005]. It is well known that ED is a long-term and sometimes permanent complication, even when maximal cavernous nerve-sparing techniques are applied. Sexual function is one of the most afflicted domains of health-related quality of life by prostate cancer therapy [Sadovsky et al. 2010].
Previous studies demonstrated that patient satisfaction depends on therapeutical effectiveness and on psychological and physical side effects. Current possible treatments differ considerably for side effects. For this reason, urologists should advise the best available personalized therapy, after sharing clinical decision-making with the patient and the family members [Wagner et al. 2011].
However, it must be underlined that a significant proportion of patients have optimistic expectations regarding sexual function after surgery, despite extensive counseling. Indeed, Wittman and colleagues demonstrated that, even though patients were educated to expect lower sexual function, they await a similar or a better sexual function 1 year after surgery, in comparison with baseline [Wittmann et al. 2011].
Other studies showed that many patients accepted side effects related to prostate cancer treatment, because a feeling of relief prevailed. They were so happy to have survived a condition they perceived as life threatening, that side effects were of minor importance to them [Korfage et al. 2006].
This review discusses the new therapeutic options from both a pharmacological and surgical point of view for treating ED after RP. We begin by analyzing the physiological and pathological mechanisms behind ED and then assess current and future options to improve the recovery of erectile function.
Concept of penile rehabilitation
Briganti and Montorsi first used the term penile rehabilitation, although other terms like erectile rehabilitation were used earlier with an analogous meaning [Briganti and Montorsi, 2006]. Penile rehabilitation is defined today as the use of any drug or device at or after RP to maximize erectile function recovery [Mulhall, 2009]. The concept of penile rehabilitation is based on the research findings that the loss of daily and nocturnal erections after RP leads to poor corporal oxygenation with penile atrophy, veno-occlusive dysfunction, and smooth muscle apoptosis. To break this vicious cycle, early intervention is suggested. Montorsi and colleagues were the first to apply this concept to patients after RP by early intracavernous injections of alprostadil [Montorsi et al. 1997; Magheli and Burnett, 2009].
To appreciate the strategy of penile rehabilitation after RP, a number of concepts need to be understood, namely the anatomy and physiology of erection and the pathophysiology of ED after RP.
Anatomy and physiology of erection
A multistep process is necessary to obtain an erection. The first step is tumescence. The two major physiological events in tumescence are arterial and arteriolar vasodilatation, which causes increased blood flow to the lacunar spaces and simultaneous relaxation of the sinusoidal smooth muscle, allowing distension. The second step is veno-occlusion that causes rigidity of the penis. The increase in blood flow actually raises pressure in the male organ and compresses the subtunical venular plexus between the tunica albuginea and the peripheral sinusoids, thus reducing the venous outflow. The tunica is stretched to its capacity, and the emissary veins between the inner circular and the outer longitudinal layers are occluded, with a decrease in the venous outflow to a minimum. At this point there is an increase in partial pressure of oxygen (to about 90 mmHg) and in intracavernous pressure (around 100mm Hg) that brings the penis to its erect state. When ischiocavernous muscles tense, the pressure in the corpora cavernosa rises to several hundreds of millimeters of mercury and causes the rigid-erection phase [Dean and Lue, 2005].
The level of contractility of the corporal myocytes is the critical determinant of the erectile phenomenon. It is the result of a complex scenario made by the contemporaneous action of neurotransmitters, neuromodulators, and hormones [Gratzke et al. 2010].
Corporal smooth muscle relaxation and erection
After a visual or tactile stimulus, nonadrenergic, noncholinergic nitrergic neurons and endothelial cells release nitric oxide (NO), which is an unstable, gaseous, and transient mediator synthesized by endothelial nitric oxide synthase (eNOS) and by neural nitrous oxide synthase (nNOS). NO passes through smooth muscle cell (SMC) membrane and interacts with soluble intracellular cytoplasmic guanylate cyclase (GC). GC activity is important to amplify NO signal through the conversion of guanosine monophosphate (GMP) to cyclic GMP (cGMP). After that, cGMP interacts with protein kinase, which phosphorylates several cellular proteins (K+ channels, myosin binding protein, Ca2+ channels, and pumps). Phosphodiesterase 5 (PDE5) downregulates cGMP levels through the enzymatic degradation in GMP. The NO effect on corporal smooth muscle could also be obtained by other neurotransmitters/neuromodulators, such as vasoactive intestinal polypeptide (VIP), calcitonin gene-related peptide, and prostaglandins E1 and 2 (PGE1 and PGE2), which increase cyclic nucleotide and reduce Ca2+ intracellular levels [Christ and Lue, 2004].
Corporal smooth muscle contraction and detumescence
Detumescence of the penis is obtained through activation of the α1 adrenoreceptor or endothelin a (ETa)/endothelin b (ETb) receptors (that bind principally ET1 but also ET2 and ET3) and activation of protein Gq, that causes activation of phospholipase C, that cleaves PIP2 in inositol triphosphate (IP3) and diacylglycerol (DAG). IP3 causes the release of intracellular calcium through interaction with the IP3 receptor, and calcium together with DAG activates protein kinase C (PKC). However, activation of the α1-adrenoreceptor or ETa receptor subtype causes activation of Rho A/Rho kinase and triggers cycling of myosin crossbridges along actin filaments and the development of force through inhibition of myosin light chain phosphatase [Bivalacqua et al. 2004]. The signaling downstream effect is increased corporal SMC tone obtained, thanks to increased intracellular levels of calcium and increased calcium sensitization [Christ and Lue, 2004; Andersson, 2001; Christ, 2000; Toda et al. 2005].
GAP junctions
The supply of autonomic fibers to smooth muscle is limited; actually there is not a one-to-one ratio between nervous fibers and SMCs. It was first postulated and then demonstrated that coordinated responses to obtain penis erection/detumescence are due to GAP junctions (connexin 43) among corporal myocytes [Christ and Lue, 2004; Toda et al. 2005; Christ, 2000].
Pathophysiology of erectile dysfunction after radical prostatectomy
After NSRP, spontaneous erectile function is frequently impaired, probably because of a reversible injury of the cavernous nerves, a process known as neurapraxia. This temporary deficit can abolish any form of erection and can last up to several years. Walsh and Donker made the first etiologic classification in 1982 where they identified the surgical injury to the pelvic nerve plexus as the cause of ED [Walsh and Donker, 2002]. However, recent series have demonstrated that the classification system for post-RP ED etiology is more complex. Today we recognize three main pathological factors contributing to post RP ED.
(1) Venogenic: ED is principally due to hypoxia-induced fibrosis and consequent venous leakage. It has been demonstrated in rats that a reduction in the percentage of sulfur dioxide (hypoxia) induces collagen synthesis by transforming growth factor (TGF) β1 and inhibits the production of PGE1 [Moreland, 1998]. Mulhall et al. [2002] evaluated the penile vascularization of post-NSRP nonpharmacologically treated patients with duplex Doppler ultrasound or dynamic infusion cavernosometry and cavernosography. They found that 75% of patients had vascular alteration, of whom 26% had venous leakage. Furthermore it appeared that the prognosis for the return of functional erections is worst when venous leakage is present. The underlying pathophysiological mechanism is still little known. Fibrosis reduces nervous vitality and it alters smooth muscle stretch capacity and corporeal veno-occlusive mechanism, similarly to RP injuries. For that reason we could assume that systemic sclerosis ED could be a mice model for post-RP fibrosis. Excessive corporal fibrosis, increased collagen synthesis by SMCs, and the accumulation of extracellular matrix have been observed [Nehra et al. 1995]. We could then hypothesize that fibrotic tissue impairs the corpora cavernosa elasticity compressive action on subtunical venules and induces abnormal venous drainage.
(2) Arteriogenic: ED is due to the excision of accessory and aberrant pudendal arteries that may originate from external iliac, hypogastric, or obturator arteries. Their presence varies from 4% to 75%, and they perfuse the corpora cavernosa unilaterally or bilaterally. In certain patients these arteries are the only ones responsible for blood supply to the corpora cavernosa [Walz et al. 2010]. Consequently, in such selected cases, surgeons must carefully preserve accessory and aberrant pudendal arteries. However, their preservation in nonselected cases (corpora cavernosa blood supply not exclusive to accessory and pudendal arteries) has favorably influenced the recovery of sexual function and the interval to recovery after RP [Rogers et al. 2004]. In 2008, Mulhall and colleagues introduced the concept of artery-sparing RP because of the increasing evidence of postbilateral NSRP ED caused by vascular abnormalities. It is still to be determined which accessory and aberrant pudendal arteries have to be spared [Mulhall et al. 2008].
(3) Neural injury: ED is due to cavernous nerve traction, dissection, or transection. Neurapraxia ensues from even minor neural trauma. Any neural trauma causes a reversible reduction in nonadrenergic, noncholinergic nitrinergic neurons in rats [Carrier et al. 1995] and has also been confirmed in humans. A study by Walsh and colleagues reported a number of patients who regained potency after preservation of only one neurovascular bundle [Walsh et al. 1987]. This means that post-RP regeneration of nitrinergic neurons, that is, return to potency, can happen only if one of the prostatic neural branches is preserved.
Published clinical studies about phosphodiesterase 5 inhibitor therapeutic efficacy in erectile dysfunction (ED).
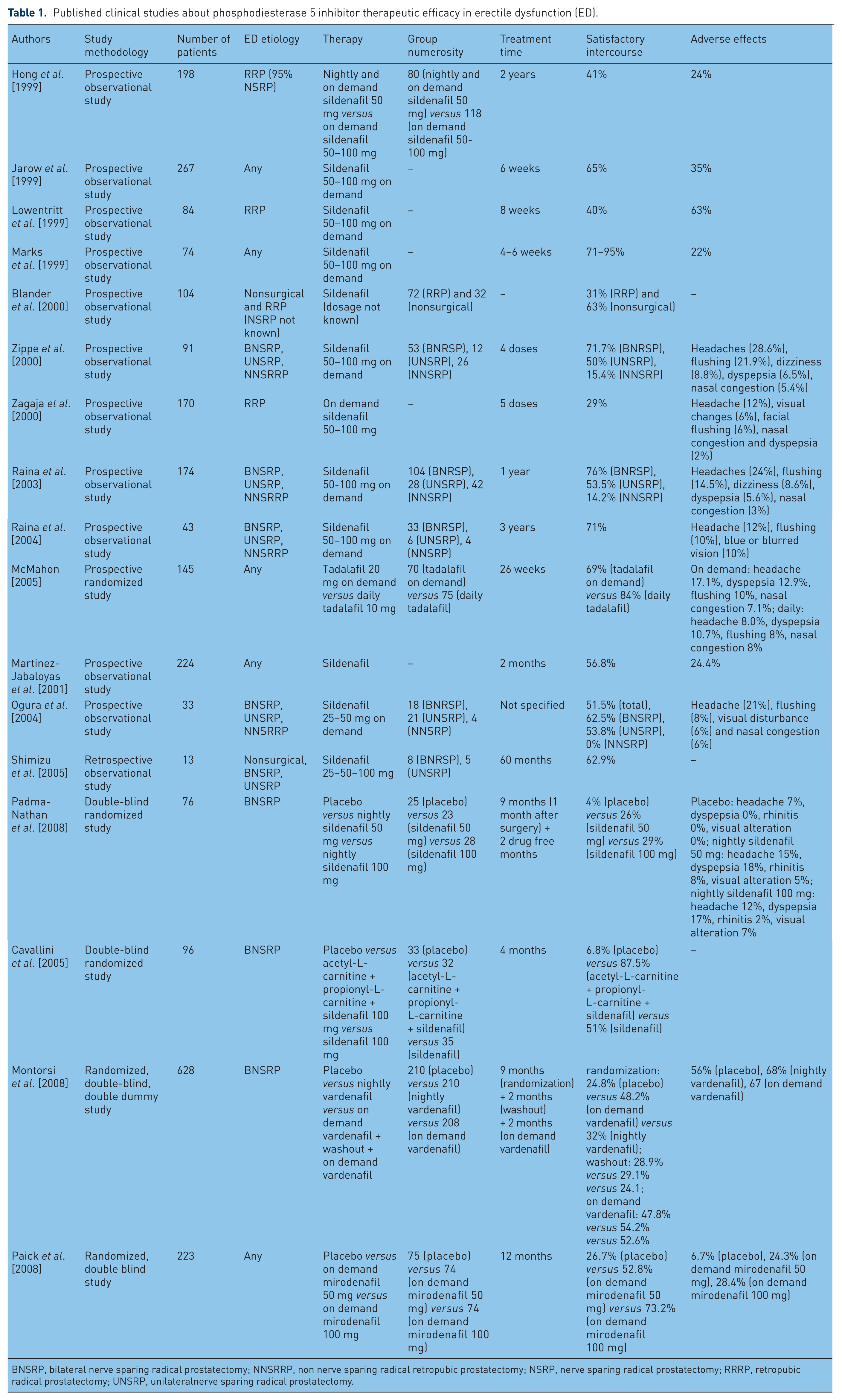
BNSRP, bilateral nerve sparing radical prostatectomy; NNSRRP, non nerve sparing radical retropubic prostatectomy; NSRP, nerve sparing radical prostatectomy; RRRP, retropubic radical prostatectomy; UNSRP, unilateralnerve sparing radical prostatectomy.
Surgical advances in urology: robot-assisted laparoscopic prostatectomy
The recent introduction of advanced robotic devices such as the Da Vinci Surgical System (Intuitive Surgical Inc, Sunnyvale, CA, USA) to the field of urological surgery has added new hopes of reducing operative times and postoperative complications and increasing postoperative potency and continence rates.
Preliminary data indicate that the oncological and functional outcomes of robot-assisted RP (RARP) are comparable with those of laparoscopic RP (LRP) and open RP. In particular Box and colleagues in 2008 demonstrated that potency rates with or without the use of any medication is around 80% at 1 year [Box and Ahlering, 2008]. In 2009, a prospective randomized trial by Lee and colleagues followed 77 patients who underwent nerve-sparing robotic hand-assisted prostatectomy in the postoperative penile rehabilitation protocol. Patients received either sildenafil citrate or tadalafil three times a week. They found that 72% of the men had discontinued PDE5 inhibitor (PDE5-I) therapy by 6-month follow up due to elevated costs.
Potency is one of the most difficult outcomes to compare after RP. Factors other than the surgeon or the approach have a significant effect on recovery of potency, including patient age, type and quality of the nerve sparing, and use of medications. Also, the assessment of postoperative continence is not standardized, including nonvalidated questionnaires and open interviews. Whether there is a difference in the potency rates after retropubic RP (RRP), LRP, or RARP is still not clear. It has been proposed that RARP may prevent damage to the neurovascular bundle because the three-dimensional magnified vision offered by the Da Vinci Surgical System allows more precise dissection and prevents inadvertent incision, traction, or incorporation of the neurovascular bundle into the suture or clip. Tewari and colleagues demonstrated better and earlier functional recovery after RARP compared with RRP [Tewari et al. 2003]. Patients who underwent RARPs showed a more rapid return of erections (50% at a mean follow up of 180 days versus 50% at a mean of 440 days after RRP) and to intercourse (50% at 340 days versus 50% at 700 days for RRP) compared with RRP patients. Furthermore they encouraged patients to try PDE5-I early to prevent fibrosis. Contrary to these results, the matched-pair analysis conducted by Krambeck and colleagues showed no differences in self-reported potency rates between the two groups at 1-year follow up (RARP 70.0%, RRP 62.8%; p = 0.08) [Krambeck et al. 2009]. However, Joseph and associates compared RARP and LRP in a single retrospective study [Joseph et al. 2005]. The assessment of EF after surgery was inconclusive and at 3-month follow up, only a nonstatistically significant trend in favor of RARP was observed. Coelho and colleagues evaluated functional outcomes of several large series of RRP, LRP and RARP currently available in the literature and demonstrated that the weighted mean potency rates for bilateral nerve sparing were higher for RARP compared with the other two surgical approaches (93% versus 60.6% for RRP versus 54% for LRP) [Coelho et al. 2010]. The poor methodology of the published studies and the absence of randomized clinical trials prevent any definitive conclusions.
Pharmacological treatment of erectile dysfunction following radical prostatectomy
Once the diagnosis of ED post RP is reached via patient history, the use of sexual function questionnaires such as the IIEF, and/or more elaborate testing such as penile Doppler ultrasonography, several treatment options are available to patients. They range from medical, to more invasive self-administrated therapies, to surgical means of therapy [Burnett, 2005].
Phosphodiesterase type 5 inhibitors
PDE5-Is are a class of pharmacological agents that act principally on a particularly isoenzyme family, PDE5, which are present in penis SMCs. Inhibition of PDE5 is responsible for an increase in cGMP and its downstream effects. Because these drugs require the presence of NO, PDE5-I could have an effect only in NSRP. They can be taken orally, and their administration is uncomplicated, which patients find favorable [Tewari et al. 2003]. Sildenafil is the drug that has been studied most extensively in post-NSRP patients since its introduction in 1998. Response rates to sildenafil after NSRP range from 10% to 76%; the rates after non-nerve-sparing NSRP vary from 0% to 15% [Hong et al. 1999; Jarow et al. 1999; Lowentritt et al. 1999; Marks et al. 1999; Blander et al. 2000; Ozden et al. 2011; Zippe et al. 2000; Zagaja et al. 2000; Raina et al. 2003, 2004; McMahon, 2005; Baniel et al. 2001; Martinez-Jabaloyas et al. 2001; Ogura et al. 2004; Shimizu et al. 2005].
In a randomized, double-blind, placebo-controlled parallel-group fixed-dosed study of 76 men who underwent bilateral nerve-sparing RP, Padma-Nathan and colleagues gave placebo, 50 mg or 100 mg sildenafil citrate nightly. They reported that 27% of the men on sildenafil regained potency compared with only 4% on placebo. Their results also showed that an earlier pharmacological intervention enhanced the recovery of spontaneous erections. There was no difference in rates of potency recovery between the two doses of sildenafil [Padma-Nathan et al. 2008].
Another prospective randomized study showed that propionyl-L-carnitine (PLC) plus acetyl-L-carnitine (ALC) improved mitochondrial respiration and increased antioxidant activity resulting in an improved effectiveness of sildenafil in restoring sexual potency in 96 men after bilateral nerve-sparing RRP; 33 patients were given placebo (group 1), 32 used PLC 2 g/day plus ALC 2 g/day plus sildenafil 100 mg when needed (group 2), and 35 used sildenafil alone (group 3) [Cavallini et al. 2005]. The efficacy of sildenafil increases with time, and best results are obtained 12–24 months after surgery [Meuleman and Mulders, 2003].
A randomized, double-blind, double-dummy, multicenter parallel-group study conducted at 87 centers assessed the efficacy of on-demand versus nightly dosages of vardenafil versus placebo in 628 patients after bilateral NSRP with normal preoperative erectile function. Dropout rates were 31%, 35%, and 33% in the placebo, nightly vardenafil, and on-demand vardenafil groups, respectively. Erectile function and sexual intercourse completion rates improved significantly in both treatment arms compared with placebo during the initial double-blind period. These data indicated that the use of on-demand vardenafil is of greater benefit than nightly treatment in patients following NSRP surgery, and in general, support the on-demand use of PDE5-Is following NSRP surgery over a daily dosing regimen [Montorsi et al. 2008].
Tadalafil is a more selective drug for PDE5 and has fewer visual side effects than other drugs [Bischoff, 2004]. However, it has high affinity for PDE11, causing myalgia and back pain [Taylor et al. 2009].
It has been demonstrated that PDE5-Is can prevent fibrosis and apoptosis in animal models, but these results have not been confirmed in humans. Thus their role in the penile rehabilitation program remains controversial [Hatzimouratidis et al. 2009].
Mirodenafil, one of the recently developed PDE5-Is, has been reported to have an excellent profile of efficacy for ED. Kim and colleagues demonstrated that after the administration of mirodenafil in bilateral nerve-injured rats that erectile function and the expression of NOS and cGMP were improved [Kim et al. 2010].
A multicenter, randomized, double-blind, placebo-controlled parallel-group fixed-dose study was conducted with 223 subjects who were randomized to placebo or mirodenafil at fixed doses of 50 or 100 mg for 12 weeks on an ‘as-needed’ basis. Mirodenafil, in doses of 50 or 100 mg, significantly improved erectile function and was well tolerated in a representative population of Korean men with broad-spectrum ED of various etiologies and severities [Paick et al. 2008]. A randomized, double-blind mirodenafil–sildenafil trial to assess which of the two drugs has more efficacy to treat ED will be of great interest.
It is important to underline that PDE5-Is have limited contraindications (retinitis pigmentosa or diseases predisposing to priapism, such as leukaemia or multiple myeloma) and that their cardiovascular safety is well known [Hatzimouratidis and Hatzichristou, 2007]. Previous studies have not demonstrated an increased risk for cardiovascular diseases (CVD), when a PDE5-I was compared with placebo [Padma-Nathan et al. 2002; Hatzichristou et al. 2004; Jackson et al. 2004].
By contrast, other studies demonstrated that PDE5-Is may have cardiovascular benefits, preventing ventricular hypertrophy and pathological remodeling, which frequently lead to heart failure. [Takimoto et al. 2005; Borlaug et al. 2005]. However, there is public awareness regarding PDE5-Is safety in patients affected by CVD before surgery. Actually CVD has great prevalence in the age group of men characterized by increased incidence of PCa.
The clinical success of PDE5-Is in ED treatment led to focus research on their potential use to treat other medical conditions. Previous studies have explored the beneficial effects of PDE5-Is in patients with cardiovascular risk factors or disease. Such research becomes even more important because CVD and ED share common risk factors and pathophysiological mechanisms [Barrett-Connor, 2004; De Berardis et al. 2003; Franklin et al. 2004]. Preclinical and clinical data demonstrated the importance of PDE5-Is in improving endothelial function and in decreasing arterial stiffness. These data suggest that PDE5-Is could also be useful for patients with metabolic syndrome and diabetes mellitus.
As discussed previously, the prevalence of ED in patients with CVD is high and the conditions may have common risk factors. A rational way to treat these patients would include a multimodal approach, aimed at improving endothelial function through different classes of drugs [Katz et al. 2000; Halcox et al. 2002; Desouza et al. 2002; Kimura et al. 2003; Vlachopoulos et al. 2004; Rosano et al. 2005; Caretta et al. 2005; Gori et al. 2005].
Since CVD and PCa are common pathologies in older people, and ED is commonly associated with both CVD- and PCa-related treatments, it would be of great interest to develop new therapeutical approaches aimed at improving ED, while reducing cardiovascular risk. Furthermore, recovery of erectile function following radical prostatectomy is largely dependent on preoperative erectile status, which is highly influenced by CVD. Therefore, any pharmacological target which aims at reducing CVD and ED will be of great benefit in a large population of older men. Other works suggest a potential therapeutic role for PDE5-Is in continence recovery after bilateral nerve-sparing prostatectomy [Gacci et al. 2010] and diabetic neuropathy [Wang et al. 2011]. Inhibition of PDE5 in adipose tissue affects adipose differentiation and aromatase function but its clinical efficacy in obesity and metabolic syndrome has not been clarified yet [Armani et al. 2011]. A new study suggests that the use of PDE5-Is may provide a protective therapeutic route for noise-induced hearing loss, caused by damage to auditory hair cells in mice [Jaumann et al. 2012].
Intracorporeal injection therapy
Intracorporeal injections (ICIs) with alprostadil, a synthetic PGE1 derivative, either alone or in combination with papaverine or phentolamine, are effective treatments for ED [Burnett, 2005]. In the series by Claro and colleagues it was demonstrated that patients who failed oral or intraurethral treatment had good results with ICIs (alprostadil, papaverine, and phentolamine triple therapy) [Claro et al. 2001]. Success, defined by the ability to engage in sexual intercourse with a hard erection, was achieved in 94.6% of patients. With respect to the role of ICIs in penile rehabilitation, beyond the initial experience of Montorsi and colleagues in 1997, an early combination of ICI alprostadil or triple therapy with sildenafil started at the time of hospital discharge following RP was assessed [Montorsi et al. 1997; Nandipati et al. 2006]. It was shown to facilitate early sexual intercourse, improve satisfaction, and possibly promote earlier return of spontaneous erections in 22 men. Sildenafil was taken daily, and the ICIs were carried out two to three times per week until natural erections occurred. The combination also allowed for a lower dose of ICIs, which minimized penile discomfort.
ICIs with PGE1, papaverine, phentolamine, or combinations thereof at doses based on patient response in a monitored setting are quite successful at achieving erections for men with post-RP ED, especially in men for whom cavernosal nerve-sparing surgery could not be achieved. This strategy is effective for men who have tried oral agents and their condition has failed to respond. Some evidence exists of the benefit of ICIs in a rehabilitative setting; however, the studies were small and uncontrolled, which prevents any definitive conclusions [Burnett, 2005].
Intraurethral alprostadil suppositories
Intraurethral alprostadil suppositories (IUAs) have been shown to be an effective treatment for organic ED [Padma-Nathan et al. 2008]. A preliminary study by Raina and colleagues showed that initiating IUA shortly after RP is safe and tolerable, and appears to shorten the recovery time to regain erectile function [Raina et al. 2007]. Patients were asked to first use 125 μg. After 4 weeks of treatment patients returned to the clinic to titrate to a dose of 250 μg of IUA. If the patients tolerated the higher dose they were instructed to remain on 250 μg of IUA at least three times. At the end of 6 months, 74% of men on the three times weekly dose reported successful intercourse compared with 37% on once-daily treatment. The Sexual Health Inventory for Men score was 18.9 in the treated group and 15.8 in the on-demand group. The study was largely observational but showed the tolerability of frequent IUAs in the postoperative period [Raina et al. 2007; Briganti et al. 2010]. The question of whether suberectile IUA would provide adequate cavernous oxygenation was addressed in penile oximetry studies. In one series comparing the effects of IUA, a vacuum erection device (VED), and ICI, the group noted that 250 μg IUA was equivalent to an erectogenic ICI dose [McCullough et al. 2010; Yuan et al. 2010]. They also noted that a nightly dose of 250 μg IUA resulted in improved cavernous oximetry the next day [McCullough et al. 2010]. The study shows the importance of the biological effect of IUA (i.e. increased oxygenation) that is much longer than the local half life of alprostadil, which is on the order of minutes.
McCullough and colleagues performed a controlled clinical trial to evaluate whether early treatment with IUA or the oral PDE5-I sildenafil citrate after bilateral NSRP hastens healing and decreases the time required for the return of spontaneous or erectogenic-aided erection. IUA appeared to provide improved erectile function, as did oral PDE5-I, despite different mechanisms of action. IUA did not require an intact nerve supply, but the oral agents rely on an intact nerve supply for a beneficial effect on sexual function. However, neither IUA nor PDE5-I offers a total solution to successful penile rehabilitation after RP. Subtherapeutic IUA has results comparable with those of oral PDE5-I [McCullough et al. 2010]. It is unclear if there is a benefit in the administration of IUAs in a penile rehabilitation capacity. The success in a salvage context for ED therapy when patients fail oral therapy is suggested but not proved. These studies are limited by their small number of subjects enrolled as well as the fact that there is not one rehabilitation regimen that has been proven superior. As such, although IUAs seemingly can be used to treat ED post RP, further studies are required to clarify their place as rehabilitation therapy
Vacuum erection devices
Vacuum therapy (VT) utilizes negative pressure to distend the corporal sinusoids and to increase the blood inflow to the penis. Depending on its purpose, VT could be used as a vacuum constriction device (VCD), with the aid of an external constricting ring which is placed at the base of penis to prevent blood outflow, maintaining the erection for sexual intercourse. Also, a vacuum erectile device (VED), without the application of a constriction ring, just increases blood oxygenation to the corpora cavernosa and for other purposes [Yuan et al. 2010].
Few studies have examined the use of VEDs specifically after RP. The use of VCDs to treat ED is well established; one of the first studies by Cookson and Nadig, conducted in a large cohort of patients with ED of various causes, demonstrated long-term efficacy and patient satisfaction rates greater than 80% [Cookson and Nadig, 1993].
VCD use following RP has several goals. Similar to concepts for pharmacological treatment after RP, a VCD, if used at fixed intervals, might prevent the long-term effects of postoperative ED by reducing the extent of physiological changes that occur as a result of surgery, such as impaired cavernous oxygenation, smooth muscle apoptosis, and fibrotic changes. In patients whose condition fails to respond to pharmacological treatment or who do not tolerate the medication, VCDs can be used in addition to or instead of drug treatments. VCDs can also be used to prevent postoperative penile shortening [Magheli and Burnett, 2009].
The first reports on the use of VCDs after RP indicated the feasibility of its use in a distinct patient cohort, and the early incorporation of VCD into the concept of penile rehabilitation was encouraged [Hall, 1995; Zippe et al. 2001; Kohler et al. 2007]. Since then, only a few studies have examined the use of VCDs in treating men with ED after RP. In a pilot study assessing the advantages of the early use of the vacuum erection device after radical prostatectomy, Kohler and colleagues enrolled 28 men who were randomized to early intervention with a VCD compared with a control group with no early postoperative intervention. They found IIEF scores to be significantly higher in the treatment group compared with the control cohort [Kohler et al. 2007]. Furthermore, they observed that, compared with the preoperative status, stretched penile length was significantly decreased in the control cohort and preserved in the treatment group. Raina and colleagues conducted a prospective randomized trial on early penile rehabilitation in 109 men after bilateral NSRP with the daily use of a VCD versus observation without any erectogenic treatment [Raina et al. 2006]. In the treatment group, 80% of patients were reported to have erections sufficient for intercourse with the use of the VCD. Spontaneous nocturnal erections returned in 32% of these men at 9 months, and 17% had spontaneous erections sufficient for intercourse without any additional aids. In the control cohort, 37% of patients had spontaneous erections at 9 months, of which 29% were sufficient for vaginal intercourse. The remaining 71% sought additional treatment after the study was closed. The proportion of patients complaining of a decrease in penile length and circumference was significantly greater in controls compared with the treatment group (63% versus 23%). The authors concluded that the early use of a VCD facilitates sexual intercourse, spousal satisfaction, and earlier return of natural erections after RP. It is interesting to note that the dropout rate from the study was not insignificant (18% at 3 months into the treatment). The final success rates might therefore have been influenced by the lack of an intention-to-treat analysis. Raina and colleagues reported on the use of a combination treatment consisting of sildenafil and VCD after RP [Raina et al. 2005]. They investigated a subgroup of patients from the former study [Raina et al. 2004] (n = 31) who were not satisfied with the use of VCD alone for the treatment of ED after RP. The addition of sildenafil to the use of a VCD led to significant improvements in each domain of the IIEF-5 score in 77% of patients. The authors concluded that combined therapy is suitable for patients who are not satisfied with a VCD alone [Raina et al. 2005]. It appears that patients who have undergone non-nerve sparing surgery, in particular, can be aided with VEDs, and a combination of a VED and sildenafil may be better than a VED alone in those who do not respond to VED alone.
Future perspectives
Gene therapy
Several gene transfer attempts have been employed to manipulate the three major types of cells involved in ED (nerve, endothelial cells, and SMCs). Target genes in endothelial cells are eNOS, vascular endothelial growth factor (VEGF), heme oxygenase-1, and superoxide dismutase. Neural ones are brain-derived neurotrophic factor (BDNF), glial cell derived neurotrophic factor, and particulate nitrous oxide synthase. Smooth muscle genes are RhoA, calcitonin gene-related peptide, hSLO, vasoinhibitory peptide, PDE5 antisense oligonucleotide, inducible nitric oxide synthase, and the potassium adenosine triphosphate channel. They have used several vectors (adenoviruses, herpes viruses, plasmids) with the same endpoint: to increase NO levels and cGMP bioavailability [Burnett et al. 2010]. It is worthwhile citing a paper published in 2006 by George Christ and colleagues. It is a trial that enrolled 11 patients with moderate to severe ED who were administered a single-dose injection in the corpus cavernosum of naked DNA plasmid containing the hSlo gene. This gene encodes the hMaxi-K channel, which while it is open allows an efflux of potassium. This electrical phenomenon causes hyperpolarization of the cell and closure of all Ca2+ channels. In the corpora cavernosa, this process means smooth muscle relaxation and vasodilatation [Shieh et al. 2000]. Patients were followed for 18 months after the treatment. No adverse effect and no change in physical examination or in blood and sperm examinations were reported for 2 years after the treatment. No conclusion on its efficacy could be made. This treatment option for ED has passed a phase 1 safety test and now is a candidate for phase 2 [Melman et al. 2006]. However, a nonspecific mode of administration and no cell-specific vectors were used.
Growth factors
Growth factors can be classified in two groups: neuromodulating agents and angiogenic cytokines. Neural regeneration is the mechanism by which erectile function improves over time following RP. Although the degree of neural trauma that occurs intraoperatively is a determinant of long-term recovery of neural function, biological factors involved in neural regeneration are likely important determinants of the completeness of neural recovery. Furthermore, these biological factors are likely a major reason for the interindividual variation in recovery of erectile function after this operation. Neurotrophic factors are molecular signals that promote nerve cell survival and maintain target organ function by facilitating axon regeneration [Burnett, 2003]. Animal studies have implicated a variety of nerve growth factors in ED [Raina et al. 2006]. The development of rat models of cavernous nerve injury has facilitated the study of neuroprotective and neuroregenerative agents [Mulhall, 2009].
To protect neurons from death and to stimulate neuroregeneration, several attempts to develop neuromodulatory drugs have been made. Neurotrophic molecules of particular interest in neuromodulatory applications for the penis include both classic neurotrophins as well as atypical neurotrophic factors. More interesting typical molecules are NGF, FGF, BDNF, neurturin, persephin, and artemin, and they have been tested on rats with positive results on erection recovery [Burnett et al. 2010].
Pentoxifylline (PTX) is a nonselective phosphodiesterase inhibitor that is further known for its broad-spectrum cytokine inhibitory properties [Wei et al. 2009; Lin et al. 2010]. It has been used clinically in a wide variety of conditions. PTX interferes with multiple cytokine pathways, such as those involved in tumor necrosis factor α and TGFβ signaling [Wei et al. 2009; Lin et al. 2010; Zabel et al. 1993; Petrovich et al. 1997; Shindel et al. 2010; Abdel-Salam et al. 2003]. These pathways are involved in both the primary nerve degeneration following cavernous nerve (CN) injury and the secondary development of penile fibrosis and SMC apoptosis [Petrovich et al. 1997; Abdel-Salam et al. 2003; Kiefer et al. 1995; Taskinen et al. 2004; Nath et al. 1998; Atkins et al. 2006]. In a recent study, Albersen and colleagues demonstrated that daily oral PTX treatment following CN crush injury resulted in a restoration of erectile function [Albersen et al. 2011]. The underlying mechanisms of recovery appear to involve enhanced nerve regeneration as well as a preservation of the microarchitecture of the erectile tissue in the corpus cavernosum. The clinical availability of PTX merits application in the near future in penile rehabilitation studies following RP.
Atypical molecules such as VEGF, insulin-like growth factor (IGF) 1, IGF binding protein 3, sonic hedgehog homolog, and growth differentiation factor 5 have shown interesting results as well [Burnett et al. 2010]. Angiogenic cytokines are represented by VEGF and angiopoietin 1. They both incremented EF in rats [Lee et al. 2002].
Erythropoietin
In a rat model, Allaf and colleagues showed that administration of erythropoietin (EPO) promoted the recovery of erectile function following CN injury [Allaf et al. 2005]. The only clinical study in humans was conducted by Burnett and colleagues. It was a retrospective small-scale trial for men who were candidates for NSRP and had normal erectile function preoperatively. In the treatment group they administered 40,000 IU EPO on the preoperative day. The control group did not receive EPO injection; both groups could employ PDE5-I on demand postoperatively. EPO administration on the preoperative day conferred improved erectile function recovery postoperatively [Burnett et al. 2008].
Stem cells
Several studies have researched the potential use of stem cells (SCs) for ED therapy. Different types of stem cells have been tested (embryonic tissue, skeletal muscle, bone marrow, and adipose tissue), but not every source has given satisfactory results. However, penile injection of nonautologous mesenchymal stem cells (MSCs) with and without concomitant adenovirus-mediated eNOS gene transfer revealed marked and significant improvements at 7 and 21 days after surgery [Bivalacqua et al. 2007]. In a pilot experiment, adipose-derived SCs were shown to improve erectile function after bilateral cavernous crush injury in a rat model of ED (unpublished work by Tom Lue and colleagues). This year a paper by Qiu and colleagues reported data about intracavernous injection of VEGF164 adenovirus-transfected MSCs on rats with diabetes-associated ED. Although rats showed an improvement in their erectile function, caution is recommended for this novelty. Actually no safety system has been inserted in the MSCs to eliminate them when excessively proliferating, no selective genetic insertion has been reported, thus increasing oncogenic risk. Moreover, no solution has been added to overcome problems like virus spread and reversion to its original form [Qiu et al. 2012].
Conclusions
RP is performed increasingly in patients with PCa and a life expectancy greater than 10 years. Because of the decrease in the mean age of this patient subgroup after prostate-specific antigen testing the quest for optimal postoperative quality of life has become more important. Data show that erectile function recovery after RP is the principal determinant of postoperative quality of life. ED depends on several preoperative, intraoperative, and postoperative factors that have to be considered adequately in each case for consequent stratification and counseling. At this time we are not able to assess whether robot-assisted RP is better or not than open or laparoscopic RP. However, several studies are focusing on ameliorating RP techniques to achieve better postoperative results. Indeed, when patients are selected properly and managed adequately after surgery, the expected rate of recovery of optimal erectile function is high. At present, PDE-5-I, ICI, and IUA do not offer a total solution to successful penile rehabilitation after RP. New trials are needed to help us understand their best clinical uses and which patients will benefit the most from them. In patients undergoing non–nerve-sparing procedures, it is suggested to use VEDs. If they are not working adequately, PDE5-I therapy could be added to increase the postoperative recovery of erectile function. Penile implant surgery is the treatment for ED associated with the highest success rate. However, it requires great surgical skills and experience and adherence to patient selection criteria. New therapeutic approaches are being studied in an attempt to improve post-RP EF that target different pathophysiological mechanisms.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.