
Abstract
Background:
Combined first-line therapies have been frequently adopted for patients with anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis. Plasma exchange (PE) or immunoadsorption (IA) was used as an add-on option following initial immunotherapies, including high-dose steroids and intravenous immunoglobulin (IVIG). However, whether a shorter delay of PE or IA can improve the early recovery prognosis of patients with anti-NMDAR encephalitis remains largely unknown.
Objective:
To compare short-term clinical improvement between patients with early and late initiation of PE or IA in anti-NMDAR encephalitis.
Design:
A retrospective study was conducted for patients admitted with anti-NMDAR encephalitis between January 2015 and December 2023 (n = 29), including 21 patients who received PE or IA as synergistic therapies.
Methods:
The clinical prognosis was compared between the early PE/IA group and the late PE/IA group in the research. Primary outcome included changes in the Clinical Assessment Scale for Autoimmune Encephalitis (∆CASE) at 90 and 120 days after encephalitis onset. Secondary outcomes included changes in the modified Rankin scale (∆mRS) after 90 and 120 days from encephalitis onset, and the length of intensive care unit (ICU) stay for patients with severe anti-NMDAR encephalitis.
Results:
The ∆CASE scores after 90 and 120 days from encephalitis onset revealed a significant difference between patients with early and late initiation of PE or IA (p ⩽ 0.05). A significant difference in the ∆mRS was also found between patients with early and late initiation of PE or IA in severe encephalitis (p ⩽ 0.05). No significant difference was found in the length of ICU admission (p = 0.101).
Conclusion:
Our findings emphasize the importance of considering PE or IA as early as feasible for patients with anti-NMDAR encephalitis, even when steroids and IVIG are in use.
Introduction
Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis is the most common autoimmune encephalitis (AE). 1 It is characterized by pathogenic autoantibodies targeting the GluN1 subunit of NMDAR. 2 Despite being a treatable condition, anti-NMDAR encephalitis incurs heavy healthcare costs. 75% of patients experience severe symptoms and require admission to an intensive care unit (ICU). Due to the severity of their condition, most of these patients need combined first-line immunotherapies during the acute phase of the disease. 3
In clinical practice, combined first-line therapies are a prominent treatment strategy, particularly when the initial clinical presentation of anti-NMDAR encephalitis is severe. 4 High-dose steroids and intravenous immunoglobulin (IVIG) are often used due to their accessibility. 5 Plasma exchange (PE) and immunoadsorption (IA) are frequently employed as synergistic therapies for the direct removal of autoantibodies in circulation because steroids and IVIG are usually insufficient to resolve AE.5,6 However, the improvement usually can be experienced by half of the patients within 4 weeks after initiating immunotherapies. 3 Besides, because IgG has an approximate 21-day half-life, PE or IA can remove therapeutic IgG and reduce the efficacy of IVIG. 7 Therefore, waiting for the initially immunotherapeutic response or concerns about removing therapeutic IgG often delay initiation of PE or IA.
Previous studies have pointed out that earlier aggressive immunotherapies were associated with better prognosis, 8 as well as the equal efficacy and safety of PE and IA. 9 However, the timing of PE or IA as synergistic immunotherapies remains largely unknown. In the present study, we analyzed the delay of PE or IA in the acute phase of anti-NMDAR encephalitis and assessed improvements with respect to the timing of PE or IA initiation. Our study also provides important implications for identifying patients who would benefit from early apheresis interventions.
Methods
Participants
All patients admitted with anti-NMDAR encephalitis between January 2015 and December 2023 at the First Affiliated Hospital of Sun Yat-sen University were included. The diagnostic criteria for anti-NMDAR encephalitis were as follows: (1) positive anti-NMDAR antibodies in cerebrospinal fluid; (2) at least one or more of the six major groups of anti-NMDAR encephalitis symptoms, including abnormal (psychiatric) behavior or cognitive dysfunction, speech dysfunction, seizure, dyskinesia, autonomic dysfunction or central hypoventilation, and decreased level of consciousness. 10 All patients met the following inclusion criteria: (1) early initiation of intravenous high-dose methylprednisolone (IVMP) or IVIG within 4 weeks after encephalitis onset; (2) received both IVMP and IVIG in the acute phase (⩽3 months after encephalitis onset); (3) (i) achieved a favorable outcome (modified Rankin scale (mRS) ⩽ 2) after 90 days from encephalitis onset with only one course of IVMP and one course of IVIG; or (ii) accepted PE or IA as synergistic therapy. Participants with other neurological diseases or severe non-neurological diseases were excluded from this study. One patient with only low-titer serum-positive anti-NMDAR antibodies was more likely to be misdiagnosed 11 and was excluded.
Severity assessments
The clinical severity at three key time points was measured with mRS and Clinical Assessment Scale for Autoimmune Encephalitis (CASE) as parts of the clinical baseline characteristics: (1) the mRS and CASE at the initial immunotherapy were completed right before the initiation of the first immunotherapy; (2) the mRS and CASE at the decision point were finished at the time of discharge for those that did not require PE or IA, or right before starting PE or IA for those who did; and (3) the worst mRS and CASE scores were finished at the clinical nadir for all patients in our research. The decision point was when clinicians determined whether to initiate apheresis. The disease severity of patients was assessed at the first three time points to ascertain their baseline functional status before apheresis.
Outcome assessments
Clinical statuses in the acute phase of anti-NMDAR encephalitis were assessed using the CASE and the mRS. CASE and mRS were conducted by two independent neurologists (MS and ZW).
Clinical improvement was defined by: ∆CASE 1 = (the CASE score after 90 days from onset) − (the worst CASE score), ∆CASE 2 = (the CASE score after 90 days from onset) − (the CASE score before PE/IA), ∆CASE 3 = (the CASE score after 120 days from onset) − (the worst CASE score), ∆CASE 4 = (the CASE score after 120 days from onset) − (the CASE score before PE/IA), ∆mRS 1 = (the mRS score after 90 days from onset) − (the worst mRS score), and ∆mRS 2 = (the mRS score after 120 days from onset) − (the worst mRS score). The primary outcome was clinical improvement identified by a reduction of CASE scores after 90 and 120 days from onset. The secondary outcome encompassed scores reduction of mRS after 90 and 120 days from onset and the length of ICU stay.
Treatments
All patients received IVMP (500–1000 mg/day × 3–5 days) or IVIG (0.4 g/kg/day × 5 days) with a very short delay, and they received both immunotherapies in the encephalitis’ acute phase. PE or IA was selected as a rescue therapy after initial therapies, including IVMP or IVIG. PE was performed on a continuous flow filtration device with a central line. One volume of plasma was exchanged against the 5% human albumin solution for a median (Q1, Q3) of 4 (3, 5) sessions. IA was performed for a median of 10 (10, 10) sessions.
Patient groups
In the non-apheresis group, patients achieved good outcomes (mRS ⩽ 2) after 90 days from disease onset with only one course of IVMP and one course of IVIG. In the apheresis group, patients received PE or IA as synergistic therapy of IVMP and IVIG in the acute phase of encephalitis. Patients in the apheresis group were divided into two groups according to the timing of apheresis: delay ⩽4 weeks versus delay >4 weeks after disease onset. Patients with severe anti-NMDAR encephalitis are defined as patients who required ICU care due to status epilepticus, disturbance of consciousness, or respiratory failure, and had a worst mRS score of 4 or 5. 12
Statistical analysis
Data was shown as n (%), median (Q1, Q3), or mean [95% CIs]. Shapiro–Wilk test was performed for continuous variables, and F-test was performed for homogeneity of variances. Comparisons of continuous variables, such as clinical characteristics and scores, were analyzed using the t tests for data with normal distribution, and Mann–Whitney U test for non-normally distributed data. Categorical variables of clinical characteristics were compared by Fisher’s exact test. The correlations between outcomes and the delay of PE or IA were evaluated by Spearman’s rank correlation coefficient. All statistical analyses were conducted using IBM SPSS Statistics version 24 (IBM Corporation, Armonk, New York, USA). p-Value ⩽0.05 was considered statistically significant.
Results
Baseline clinical features of patients with anti-NMDAR encephalitis in this study
In this study, 31 patients who met the inclusion criteria diagnosed with anti-NMDAR encephalitis between January 2015 and December 2023 were enrolled initially. At that point, one patient with comorbid multiple system atrophy and one patient with comorbid massive hemorrhage of the gastrointestinal tract were excluded from the study (Figure 1). Thus, we included 29 participants who initiated immunotherapies in 4 weeks from encephalitis onset and received both IVMP and IVIG in the acute phase of encephalitis. There were eight patients in the non-apheresis group who rated an mRS score between 0 and 2 after one course of IVIG and one course of IVMP without PE or IA therapies. Twenty-one other patients in the apheresis group received not only IVMP and IVIG but also PE or IA in the acute phase of encephalitis. In the apheresis group, there were 10 patients in the early PE/IA group with PE/IA delay ⩽4 weeks after onset, and 11 patients in the late PE/IA group with PE/IA delay >4 weeks.

The enrollment workflow and the group assignment of patients with anti-NMDAR encephalitis in the present study.
The median age of all patients was 23 years and 69% (20/29) were female. Compared with the non-apheresis group, the apheresis group had higher rates of fever, psychiatric symptoms, disturbance of consciousness, autonomic dysfunction, respiratory failure, and teratoma (p < 0.05) (Table 1). Significant differences were also found in the types of anti-seizure drugs, the delay from onset to nadir, the mRS scores at the decision point and the clinical nadir, and the CASE scores at three key time points between the non-apheresis group and the apheresis group (Table 1), of which the cut-off points were defined by receiver operating characteristic curve analysis (Supplemental Table S1). The apheresis group showed higher mRS scores with a cut-off point of 3.5, higher CASE scores with 12, and more types of anti-seizure drugs with 2.5 at the clinical nadir.
The baseline characteristics of patients with anti-NMDAR encephalitis.

One patient with CSF pleocytosis in the apheresis group was excluded from the CSF profiles analysis due to the data dearth.
The number of types of anti-seizure drugs refers to how many different types of drugs are administered within the first 120 days after onset, including sodium valproate, levetiracetam, lamotrigine, oxcarbazepine, midazolam, clonazepam, perampanel, phenobarbital, topiramate, diazepam, and propofol.
The mRS was measured at the time of discharge for those who did not require PE or IA, or right before starting PE or IA for those who did.
Abnormality in EEG included slow-wave activity and epileptic discharge.
All the patients with teratoma underwent a surgical operation and no patient presented with a second tumor in our study.
p ⩽ 0.05, **p < 0.01, ***p < 0.001, boldfaced values: statistically significant difference.
CASE, Clinical Assessment Scale for Autoimmune Encephalitis; CSF, cerebrospinal fluid; EEG, electroencephalogram; IA, immunoadsorption; IVIG, intravenous immunoglobulin; IVMP, intravenous high-dose methylprednisolone; MRI, magnetic resonance imaging; mRS, modified Rankin scale; NMDAR, N-methyl-D-aspartate receptor; PE, plasma exchange.
All clinical aspects were balanced between the early PE/IA group and the late PE/IA group except leucocytes in CSF (22 (13.75, 111.25) vs 5 (0.75, 47), p = 0.031) and the delay from onset to nadir (12 (10.25, 18) vs 38 (21, 69), p = 0.002) (Table 2). No significant difference was found in the symptom profiles between two groups (p > 0.05). The cerebral magnetic resonance imaging (MRI) was abnormal in 6/10 (60%) patients of early PE/IA group and in 6/11 (54.5%) of the other group (p > 0.05). Abnormal hyperintensities of brain MRI included cortex (2/10 vs 3/11), medial temporal cortex (3/10 vs 3/11), subcortex/white matter (1/10 vs 2/11), corpus callosum (1/10 vs 2/11), basal ganglia (0/10 vs 3/11), thalamus (1/10 vs 1/11), infra-tentorium (0/10 vs 1/11), and meninges (1/10 vs 2/11). The disease severity assessed by the CASE during the nadir was 20 (17.75, 24.25) for the early PE/IA group and 21 (19, 24) for the late PE/IA group, and by the worst mRS score was 5 (5, 5) for both groups (p > 0.05). Treatments included the types of anti-epilepsy drugs 3 [1.99, 4.01], the total courses of IVMP 1 (1, 1.25) and IVIG 1 (1, 2) in the acute phase of encephalitis for the early PE/IA group, whereas anti-epilepsy drugs 3 [2.06, 4.94], the total courses of IVMP 2 (1, 2) and IVIG 2 (1, 2) for the late PE/IA group (p > 0.05). All tumors in 10 patients (6/10 vs 4/11) were ovarian teratomas and were completely removed by surgery (p > 0.05). Rituximab (3/10 vs 1/11), tocilizumab (2/10 vs 0/11), ofatumumab (1/10 vs 0/11), and cyclophosphamide (0/10 vs 2/11) were used as second-line therapies (p > 0.05).
The baseline characteristics of patients with anti-NMDAR encephalitis in the apheresis group.

One patient with CSF pleocytosis in group with delay >4 weeks was excluded from the CSF profiles analysis due to the data dearth.
p ⩽ 0.05, **p < 0.01, boldfaced values: statistically significant difference.
CASE, Clinical Assessment Scale for Autoimmune Encephalitis; CSF, cerebrospinal fluid; EEG, electroencephalogram; IVIG, intravenous immunoglobulin; IVMP, intravenous high-dose methylprednisolone; MRI, magnetic resonance imaging; mRS, modified Rankin scale; NMDAR, N-methyl-D-aspartate receptor.
Clinical outcome between PE group and IA group
In the apheresis group, 15/21 patients received PE, and 6/21 patients received IA as rescue therapies. Furthermore, no significant difference between ∆CASE 1 scores and ∆CASE 2 scores had been observed between PE group and IA group after 90 days from onset (p = 0.724 and p = 0.666) (Figure 2(a) and (b)). There was also no significant difference between ∆CASE 3 scores and ∆CASE 4 scores in two groups after 120 days from onset (p = 0.584 and p = 0.639) (Figure 2(c) and (d)).

(a, b) The PE group and the IA group did not differ in their decline of CASE scores after 90 days from disease onset (∆CASE 1, p = 0.724 and ∆CASE 2, p = 0.666). (c, d) The PE group and the IA group did not differ in their decline of CASE scores after 120 days from disease onset (∆CASE 3, p = 0.584 and ∆CASE 4, p = 0.639).
Clinical outcome associated with PE/IA delays
No significant difference was found in the CASE scores and the mRS scores at three key time points between the early PE/IA group and the late PE/IA group (p > 0.05) (Table 2). After 90 days from onset, ∆CASE 1 was 8 (6, 14) for the early PE/IA group and 4 (2, 5) for the late PE/IA group (p = 0.005). The ∆CASE 2 scores were 7.5 (5.75, 11.25) for the early PE/IA group and 2 (1, 5) for the late PE/IA (p = 0.003). After 120 days from onset, the ∆CASE 3 and the∆CASE 4 were 11 (6, 16.25) and 10.5 (6, 15.25) for the early PE/IA group, and 4 (2, 8) and 3 (2, 8) for the other group (p = 0.015 and p = 0.007). Although the median of ∆mRS 1 scores in the early PE/IA group was higher than the other group (0.5 (0, 2) vs 0 (0, 0)), the difference was not statistically significant (p = 0.119) (Table 3). The ∆mRS 2, which represented the clinical improvement after 120 days from encephalitis onset, had a significant difference between two groups (1 (0, 3) vs 0 (0, 0), p = 0.047). Although all patients underwent early initiation of immunotherapy (IVIG or IVMP) in 4 weeks from onset and received both IVMP and IVIG in the acute phase, some patients received PE or IA after IVMP and IVIG, and the other received PE or IA after IVMP but before IVIG. The time gap between IVIG and PE or IA was presented in Supplemental Table S2.
Clinical efficacy of IA or PE as synergistic therapy in the acute phase of autoimmune encephalitis.
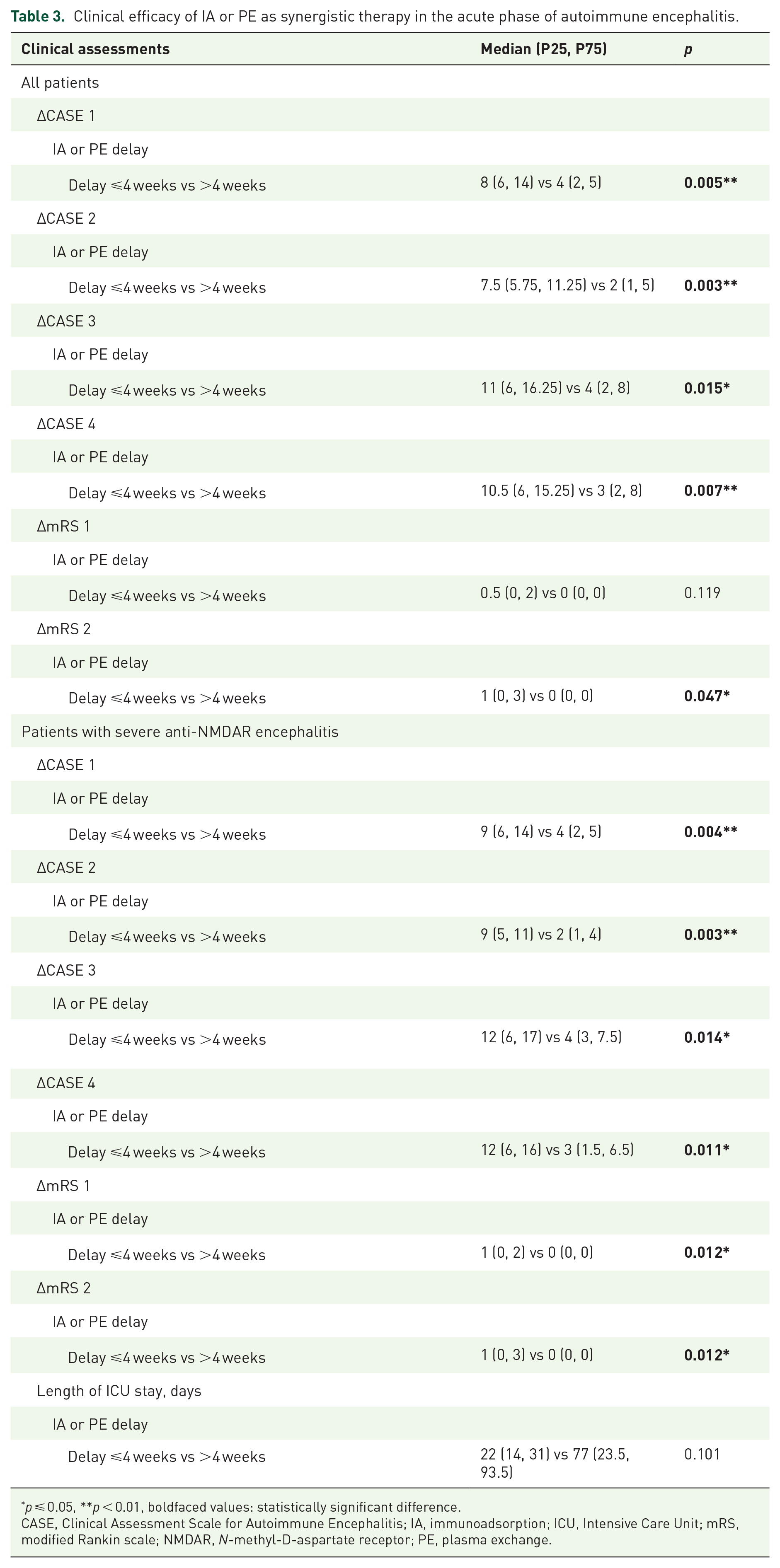
p ⩽ 0.05, **p < 0.01, boldfaced values: statistically significant difference.
CASE, Clinical Assessment Scale for Autoimmune Encephalitis; IA, immunoadsorption; ICU, Intensive Care Unit; mRS, modified Rankin scale; NMDAR, N-methyl-D-aspartate receptor; PE, plasma exchange.
In patients with severe anti-NMDAR encephalitis, there were significant differences in ∆CASE 1, ∆CASE 2, ∆mRS 1, and ∆mRS 2 between the early PE/IA group (N = 7) and the late PE/IA group (N = 9; p < 0.05). However, length of ICU admission showed no significant differences (22 (14, 31) vs 77 (23.5, 93.5), p = 0.101) (Table 3). The changes in CASE scores and the time gap between the disease onset and the initiation of PE or IA in patients with non-severe encephalitis were presented in Supplemental Figures S1 and S2.
The ∆CASE scores, which represented clinical improvement, declined along with longer PE/IA delay (∆CASE 1, ρ = −0.493, p = 0.023; ∆CASE 2, ρ = −0.582, p = 0.006, ∆CASE 3, ρ = −0.421, p = 0.057, and ρ = −0.527, p = 0.014, median of PE/IA delay = 30 days) (Figure 3). A downward trend was seen in ∆mRS scores without significant difference (∆mRS 1 ρ = −0.242, p = 0.29 and ∆mRS 2 ρ = −0.341, p = 0.13).

(a, b, d) A decline of
Discussions
The underlying mechanisms for different subtypes of AE remain largely unknown. However, current evidence supports the hypothesis that anti-NMDAR encephalitis is a B cell-dependent autoimmune disease that is mainly caused by antibodies targeting neuronal cell-surface receptors. 13 B cells, plasma cells, and IgG deposits were found in the central nervous system. 14 In vitro, antibodies were found to decrease the level of NMDARs in postsynaptic dendrites reversibly. 2 According to previous studies, anti-NMDAR antibodies are the pathogenic antibodies of anti-NMDAR encephalitis, and as a result, apheresis might have therapeutic benefits by removing the autoantibodies. 14
The therapeutic options for AE mainly include treatment strategies from other neurological autoimmune disorders. 5 A noteworthy proportion of patients with anti-NMDAR AE necessitate combinations of both first-line and second-line therapies and in some cases, further therapeutic interventions. 3 To explore the clinical efficacy of the apheresis’ timing in the combined first-line therapies, we conducted an exploratory analysis about the timing of immunotherapies here.
In a retrospective study of 577 patients with anti-NMDAR encephalitis, clinical improvement assessed by mRS scores was observed in 53% of patients within 4 weeks after immunotherapy and tumor resection. 3 One of the independent factors for good outcomes in patients who required intensive care was early aggressive immunotherapy, such as combined first-line immunotherapy, 15 or early initiation of second-line immunotherapy with rituximab. 16 While most studies have focused on long-term outcomes after combined treatment, such as recovery time, 17 the precise effectiveness, and the timing of treatment responsiveness may not be well-defined due to the overlapping use of immunotherapeutic agents. 4 In our study, we attempted to assess the shorter-term response after PE or IA through changes in clinical scores after 90 and 120 days from the onset of encephalitis and ICU duration. Additionally, many studies based the outcome assessments on mRS,18–20 which was designed to assess neurological function recovery of patients after stroke with scores from 0 to 6. It is crucial to recognize that mRS may not be as sensitive as CASE to measure clinical improvement in patients with AE. Our study emphasizes the importance of adopting a shorter-term therapeutic reaction and a more suitable clinical score for evaluating the specific effects of PE or IA in anti-NMDAR encephalitis.
The accessibility and convenience of steroids and IVIG often make them the first tools deployed in the therapeutic regimen. 5 PE and IA are recommended as late add-on treatments if the efficacy is insufficient with a delay resulting from waiting time for therapeutic response and concerns about removal of IgG from IVIG. 5 The efficacy of PE or IA, which aimed at removing antibodies, was investigated in a prospective observational case-control study conducted by Heine et al., involving 21 patients with AE. Notably, both PE and IA yielded a significant clinical improvement, with a 67% reduction in mRS scores in PE group (N = 11) and a 60% reduction in IA group (N = 10). 9 The equal efficacy of PE and IA was proven in anti-NMDAR encephalitis in our study. However, the influence of the starting time of PE or IA had not been analyzed in AE previously, although some studies have been performed in other neurological autoimmune disorders. Previous studies have shown that minimizing the delay of PE (⩽5 days) was associated with maximal improvement in patients with attacks of neuromyelitis optical spectrum disorder. Conversely, a longer delay in PE, even when applied as a rescue therapy after steroids, decreased clinical improvement. 21 Consistent with those previous studies, our study found that patients treated with PE or IA within 4 weeks after the onset of anti-NMDAR encephalitis exhibited greater reductions in CASE scores in the overall patient cohort. Although there was more mRS score reduction in the group with a shorter delay, the difference between the two groups in the overall patient cohort did not reach statistical significance. The longer delay from onset to clinical nadir in the late PE/IA group suggested the disease progressed without adequate treatment. On the other hand, we observed a significant difference in mRS score reduction between the group with a delay ⩽4 weeks and the group with a delay >4 weeks in patients with severe anti-NMDAR encephalitis. This suggested that the changes in mRS may not be sensitive enough to measure meaningful clinical responses of patients in AE. Additionally, the timing of apheresis may be more crucial for patients with severe anti-NMDAR encephalitis.
A multivariate logistic regression model has predicted 1-year prognosis after anti-NMDAR encephalitis. ICU admission, abnormal MRI, lymphocytic pleocytosis, treatment delay, and lack of immunotherapy response at 4 weeks were associated with poor outcomes in the model. 22 However, the factors related to apheresis initiation had not been analyzed. Based on our study, we advocate the consideration of PE or IA as soon as practically possible in patients with anti-NMDAR AE, particularly those presenting severe symptoms or with teratoma. Severe symptoms encompassed fever, psychiatric symptoms, disturbance of consciousness, autonomic dysfunction, and respiratory failure, indicating that disruptions might occur in the diencephalon and brainstem. IVIG can be used after PE or IA as a supplementary therapy to avoid potential wastage caused by antibody-removing interventions, given its efficacy through a long-term immunomodulatory mechanism. Moreover, our results suggested that the early initiation of therapeutic apheresis (⩽4 weeks) still made a beneficial impact on patients who received combinational treatment of IVMP and IVIG. In patients who received early immunotherapies including IVMP and IVIG, the delayed time longer than 4 weeks may still hamper the benefit of PE or IA. It is viable to decrease the observing time of initial immunotherapeutic response to less than 4 weeks after disease onset, while more precise observing time requires a much larger sample size with subgroup analysis.
The calculation and justification of the sample size were not conducted because anti-NMDAR AE is a rare disease (about 1.5 per million per year), 23 and we could only gather a small sample at our center. To reduce the sample size requirements, continuous outcome variables and a composite endpoint were used in the current study.24,25 It is still important to note that the evidence generated from the small-sample research has limitations in its application because of the sampling error. Although it is difficult to compare the effects of different immunotherapy combinations in patients with anti-NMDAR AE, our study suggests that comparing the short-term response of specific immunotherapy in patients may be a significant step to optimize the management of combined immunotherapies.
Conclusion
Our study underscores the importance of optimizing the therapeutic timeline. The effectiveness of apheresis was associated with their early integration into the treatment regimen. Minimizing the delay in PE or IA in patients with severe conditions may enhance the overall efficacy of the combined therapeutic approach. These findings provide future perspectives on optimizing therapy regimens for anti-NMDAR encephalitis patients.
Supplemental Material
sj-docx-1-tan-10.1177_17562864241276208 – Supplemental material for Short delay to initiate plasma exchange or immunoadsorption as synergistic therapies for patients in the acute phase of anti-NMDAR encephalitis
Supplemental material, sj-docx-1-tan-10.1177_17562864241276208 for Short delay to initiate plasma exchange or immunoadsorption as synergistic therapies for patients in the acute phase of anti-NMDAR encephalitis by Miao Su, Zichao Wu, Qiuyan Luo, Huiyu Feng and Hongyan Zhou in Therapeutic Advances in Neurological Disorders
Footnotes
Acknowledgements
We thank the patients who contributed the clinical data to this study. We thank Dr. David Westover for his valuable suggestions and English proofreading on this manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.