
Abstract
Background:
Previous studies have suggested that the Pro-Kin visual feedback balance system can promote the recovery of balance function in stroke patients.
Objectives:
However, this system has not been used effectively in the early stages of stroke rehabilitation. This study aimed to investigate the effect of Pro-Kin system combined with weight loss system for the early recovery of balance and walking ability following a stroke.
Methods:
A total of 62 patients who underwent radiological diagnosis of stroke were randomly divided into two groups: a control group (n = 31) and a treatment group (n = 31). Both groups received conventional balance training. The treatment group also received training on the Pro-Kin system in conjunction with a weight loss system. Balance was measured using the Berg Balance Scale (BBS), Timed ‘Up & Go’ (TUG) test and Pro-Kin system. Walking ability was assessed using the Functional Ambulation Classification (FAC). The tests were performed before the start of treatment and on the 4th week following the training. There was no statistically significant difference between the groups before training.
Results:
After 4 weeks of training in both groups, there were significant improvements in balance and walking ability. BBS values and FAC were significantly higher (p < 0.01), TUG times, ellipse area and motion trajectory length were significantly reduced (p < 0.01, p < 0.05) after training. The treatment group outperformed the control group (p < 0.05). In addition, there was a positive correlation between balance function and walking ability (p < 0.01).
Conclusion:
The Pro-Kin system combined with weight loss system is a viable method that promotes early reconstruction of balance and walking ability following a stroke.
Trial registration:
Clinical trial number ChiCTR1900026370. https://www.chictr.org.cn/showprojEN.html?proj=43736
Keywords
Introduction
The incidence of stroke in China is increasing annually and the country now has the highest number of stroke victims in the world.1,2 Abnormal changes in muscle tone and reduced active control of the affected side after a stroke can lead to reduced balance and difficulty walking, as well as an increased risk of falls.3–5 This not only affects physical function for the patients but also places a significant burden on their families and society as a whole; thus, improving balance and preventing falls are important treatment goals for people who have experienced a stroke.6,7
The use of the Pro-Kin visual feedback balance system (Figure 1(a)) for the treatment of post-stroke balance dysfunction has increased in recent years.8–10 Previous studies have shown that the Pro-Kin visual feedback balance system can increase the motivation of patients to participate in post-stroke rehabilitation training by making it more lively and interesting than conventional rehabilitation. Moreover, the real-time feedback of the Pro-Kin visual feedback balance system can improve balance and walking ability following a stroke by promoting symmetrical weight distribution, reducing postural sway, improving walking stability, enhancing muscle strength and reducing muscle atrophy.8,11

(a) Pro-Kin system. (b) Weight loss system.
In addition, previous studies have shown that early rehabilitation following a stroke is important for improved balance, as starting functional training in the acute phase improves balance more than in the sub-acute or post-acute phase.12,13 However, as the Pro-Kin visual feedback balance system can be used effectively in clinical practice in the standing position, training should only be initiated once the patient has regained dynamic standing balance. In this study, the Pro-Kin visual feedback balance system was combined with weight loss system (Figure 1(b)) to promote early balance and walking reconstruction in the early stages of stroke rehabilitation, when the lower limbs can be partially weight-bearing and standing balance has not yet become static. The findings provide insight into new ways of improving balance and walking ability in the early stages of stroke rehabilitation.
Methods
Study participants
The study group consisted of 62 subjects (the minimum sample size which can satisfy the test efficiency is determined by using the sample size calculation formula of the superiority test) who underwent radiological diagnosis of stroke at Gansu Provincial Hospital between April 2020 and September 2023. All subjects were between the ages of 50–80 years and had no history of leg injuries or other conditions associated with balance disturbances. In addition, all participants scored <56 on the Berg Balance Scale (BBS) and >24 on the Mini Mental State Examination (MMSE). As judged by the senior physiotherapist, if the individual had experienced a stroke within the past month, was able to stand with assistance for at least 1 min and required balance training, a referral should be made. Patients were excluded if they (i) had recurrent stroke; (ii) have bilateral hemispheric, cerebellar or brainstem lesions; (iii) experienced severe spasticity or cognitive deficits; (iv) have orthopaedic problems; (iv) experienced peripheral neuropathy, significant visual field or hemineglect; (v) have a cardiovascular or respiratory impairment or (vi) presented with other concomitant conditions. Individuals who changed their treatment plan during the prescribed exercise programme and those who were not in a position to undergo follow-up testing were also excluded from the final analysis.
A total of 62 patients were assigned in the treatment group (n = 31) and control group (n = 31) according to the random number table method.
Patient and public involvement
Patients and/or the public were not involved in the design or conduct or reporting or dissemination plans of this study.
Randomization scheme
The randomization scheme was in accordance with CONSORT declaration, and the random concealment mechanism was established by using completely random design, and the grouping scheme was composed of two parallel sample groups: the treatment group and control group. SPSS version 27.0 (IBM Corp., NewYork, America) was used to generate a random digital allocation table with a sample size of 62 and a grouping number of 2, which was saved to an independent third party (individuals who did not participate in the experiment), kept confidential before the end of the experiment and hidden random distribution scheme. Random numbers and packet names encoded in the same order are saved with envelopes encoded only in the label sequence. Whenever the subjects are selected, the third party of the hidden random scheme is asked to open the corresponding envelopes to reveal the allocation into the group, and the subjects are randomly divided into the treatment group or the control group.
Data collection
Balance function was calculated using the BBS 14 and Timed ‘Up & Go’ (TUG) tests. 15 The BBS is a clinical functional measure of balance disorder, consisting of 14 items of increasing difficulty, rated on a 5-point ordinal scale (0–4). The maximum possible score is 56, with higher scores indicating better balance. In this study, a TUG test was also administered to assess the subjects’ balance; this test records the time (in seconds) it takes for the subject to stand up from a chair, walk 3 m, turn around, return to the chair and sit down again. The shorter the time, the better the balance. Functional Ambulation Classification (FAC) 16 was used to assess walking ability. This scale is divided into five levels, with higher levels indicating improved walking ability. The three tests were repeated twice and the average score was recorded.
The Pro-Kin visual feedback balance system (PK254; TecnoBody S.R.L., Bergamo, Italy) was used in this study. The Pro-Kin system utilizes a force-sensitive platform to assess centre of pressure (CoP) movement-induced postural sway. Users stand comfortably in a standardized position on the platform and are instructed to look at the screen surface directly in front of them and to keep their arms at their sides and their eyes focused on a stationary target when standing in a normal forward-facing position.
The weight loss system (YK-7000A2; Yikang Medical Equipment Industry Corp., Guangzhou, China) was used in conjunction with the Pro-Kin system. It is controlled by a sling and uses the principle of individualized minimal weight loss according to the patient’s ability, typically 20% of the patient’s body weight, while maintaining constant traction to ensure the patient can stand properly.
Procedures
The control group received regular balance training for a total four practice sessions of 20 min per session, 10 times a week. The exercises were as follows: (i) muscle strengthening and postural transfer exercises; (ii) sitting in front of a mirror and being pushed from different directions by the therapist; (iii) moving someone’s weight forwards, backwards and sideways; (iv) passing the ball to the therapist who had arranged it in a circle and throwing and catching it.
All subjects in the treatment group performed balance training (20 min each) using the Pro-Kin system with the support of a weight loss training system on top of their regular training; subjects used the Pro-Kin system with the support of a weight loss system for 10 min each time, 10 times a week for 4 weeks: One test with open eyes (OE) and one with closed eyes (CE). Using visual feedback sensitive to CoP displacement, patients were asked to move the CoP over a designated area in various directions (including forwards, backwards, sideward and circular movements) (Figure 2) with the support of the weight loss training system. Patients also played two games of their choice, selecting from three options: a ping-pong game, a light display and a ski simulator (Figure 3). In each of these conditions, the motion trajectory length (in mm) and ellipse area (in mm2) were measured, for a total of four different outcome variables. The test was performed twice, and the mean score was recorded.

Modes of training using the Pro-Kin system. (a) Forwards and backwards. (b) Sideward. (c) Circular motion.

Game training. (a) Ping pong. (b) Light. (c) Skiing.
Statistical analysis
All statistical tests were performed using SPSS version 27.0 (IBM Corp.). Independent t tests were used to compare the means of the control and treatment groups. Paired t tests were used to compare the means before and after treatment. Differences in categorical variables were analysed using Mann–Whitney’s U test. Correlation analysis between balance function and walking ability was carried out using Pearson’s correlation coefficient. For all tests, p < 0.05 was considered to indicate statistical significance.
Results
Table 1 describes the general characteristics of the subjects, including sex, age, time since stroke and MMSE scores. The differences between the groups were not statistically significant (p > 0.05). Tables 2–4 shows the BBS, TUG, FAC scores, ellipse area and motion trajectory length before and after training and the changes. No significant differences were found between the groups before training (p > 0.05). However, the results before and after training for each group showed that BBS and FAC values were significantly higher following training (p < 0.01), TUG values and ellipse area and motion trajectory length were significantly lower after training (p < 0.01, p < 0.05), especially in the treatment group. Compared with the control group, BBS, TUG, FAC, ellipse area and motion trajectory length were significantly improved in the treatment group following (all p < 0.05).
Characteristics of the participants.

MMSE, Mini-Mental State Examination.
Comparison of BBS, TUG, FAC before and after training between the two groups.

BBS, Berg Balance Scale; FAC, Functional Ambulation Classification; TUG, Timed ‘Up & Go’.
Comparison of ellipse area before and after training between the two groups.
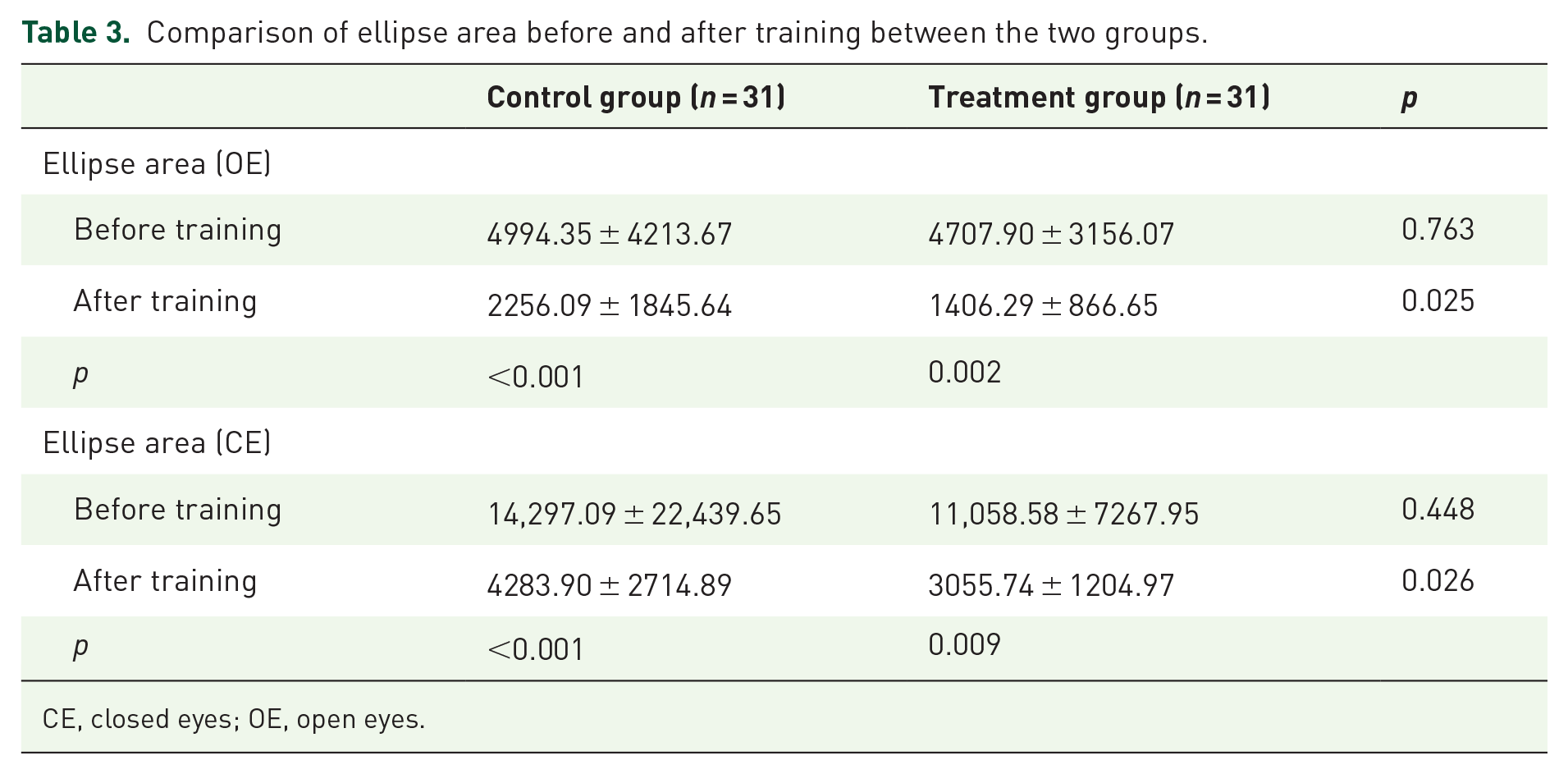
CE, closed eyes; OE, open eyes.
Comparison of motion trajectory length before and after training between the two groups.
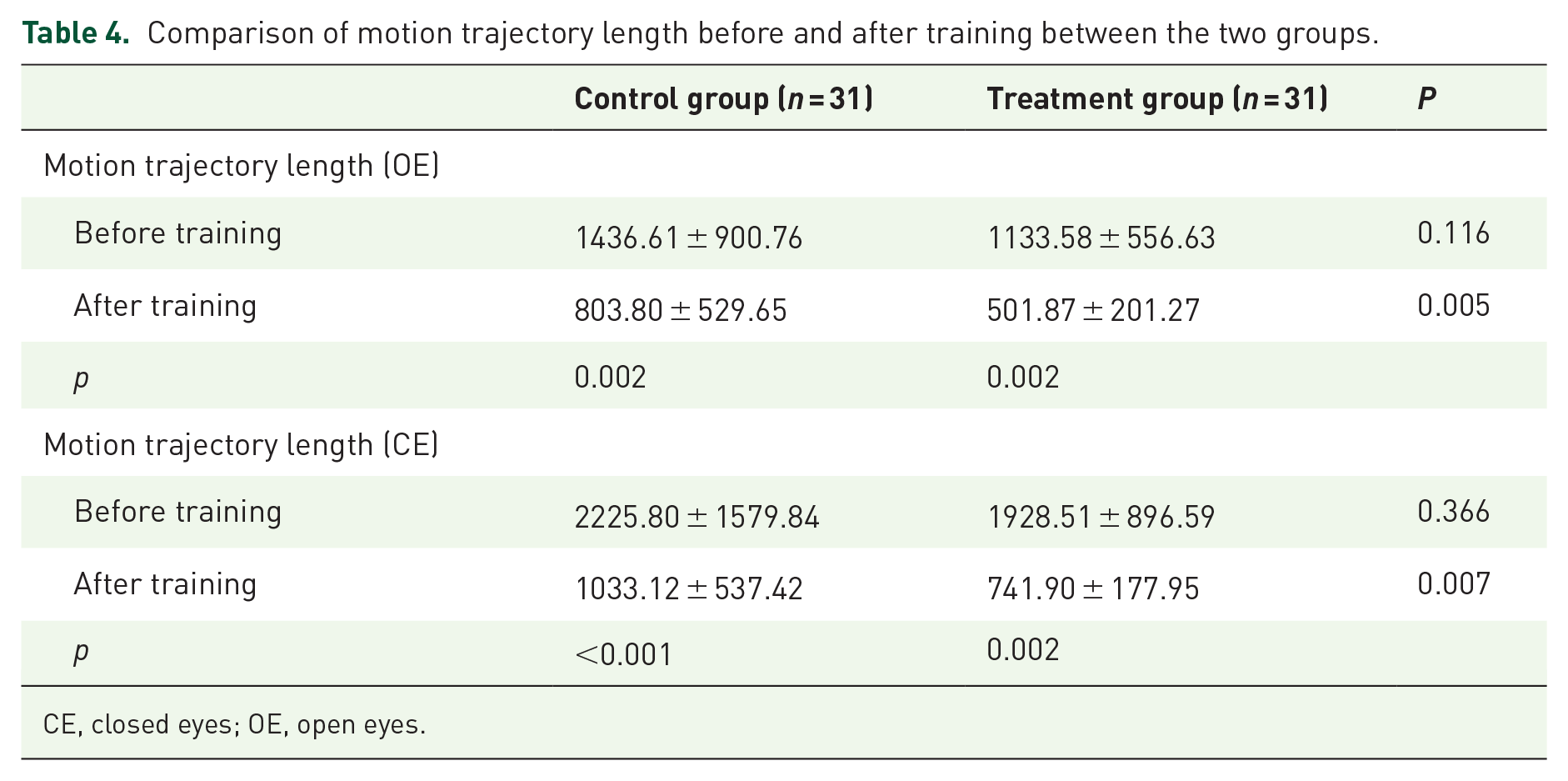
CE, closed eyes; OE, open eyes.
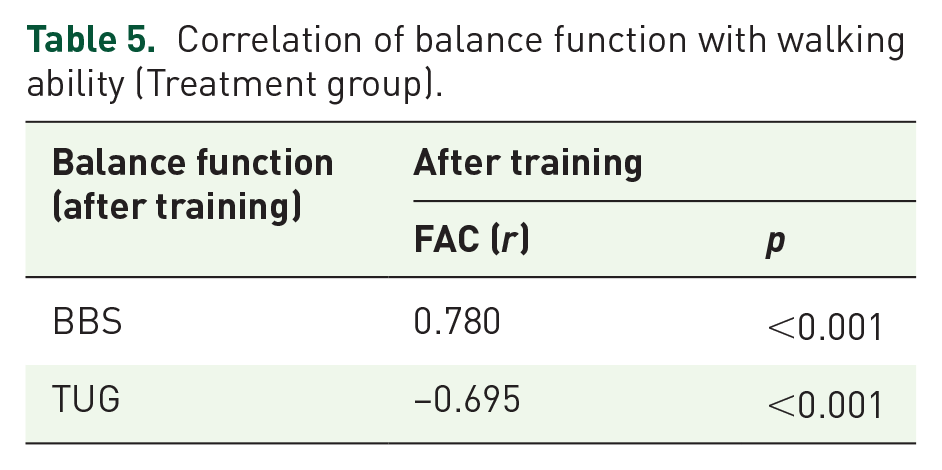
Correlations between balance function and walking ability in the treatment groups are presented in Table 5. Post-training BBS and TUG values significantly correlated with FAC (r = 0.780, p < 0.01 and r = −0.695, p < 0.01 for BBS and TUG, respectively). To further assess the outcomes in both groups, changes from baseline to post-training were calculated for all outcomes; this analysis showed a significant change in all outcomes in the treatment group.
Correlation of balance function with walking ability (Treatment group).
Discussion
Among the functional impairments left after a stroke, balance impairment is an important factor affecting motor function in patients who have experienced a stroke; thus, early restoration of balance function is an important rehabilitation goal for stroke patients.6,7,17 Previous studies have shown that restoration of sitting and standing balance occurs in the early stages following a stroke, and the earlier the rehabilitation mediator, the better the functional recovery and overall outcome of the patient. 4 The Bobath technique and the Brunnstrom method have long been used as the primary treatment to restore balance in patients who develop hemiplegia following a stroke, with a focus on standing balance and lower limb motor control training,18,19 although most of the training is initiated at a late stage.12,20–24 The development of methods that could improve the balance in the early stages following a stroke has become an important objective in neurorehabilitation research.
The aim of this study was to compare the effects of two different treatment modalities, conventional balance training and visual feedback balance training combined with a weight loss system, on the balance and walking ability of patients in the early stages of stroke rehabilitation. The results demonstrated that compared with the control group, patients who used the Pro-Kin visual feedback balance system combined with the weight loss system experienced significant improvements, both in balance and walking ability. The reasons underlying the differences between the two groups may be explained as follows.
The first reason is that motor balance and coordination depend on the vestibular, proprioceptive and visual systems to receive and transmit information regarding the position of the body.17,25,26 In recent years, training using the Pro-Kin visual feedback balance system has become an important therapeutic approach.8–10,27–30 With the Pro-Kin system’s visual dynamic feedback, patients are able to effectively control their own body weight movements and correct abnormal body positions in a timely manner, thereby improving their ability to move their weight within a stable range and improving balance control.8,27,28 Our results are consistent with previous studies using the Pro-Kin system in stroke survivors, providing supportive evidence that visual feedback from a force-sensitive platform is effective in reducing balance dysfunction after a stroke.8,31,32
Second, the weight loss system can reduce the weight load on the lower limbs to varying degrees through the suspension device, facilitating early training for patients with inadequate support.33–36 Balance training with the weight loss system improves the patient’s sense of security, eliminates stress and fear during treatment and enables early balance training for patients whose standing balance has not yet reached a static level.33,34 After 4 weeks of training, the patients in this study showed improvement in balance and walking ability, and post-training BBS and TUG values significantly correlated with FAC. These results further confirm that balance is closely associated with the recovery of walking ability and a reduction in the probability of falling.8,37–39 Thus, we propose that the use of the Pro-Kin visual feedback balance system supported by training with a weight reduction system facilitates the organic integration of weight-bearing and balance factors when walking, thus promoting the early re-establishment of normal walking patterns.
Although these findings demonstrated the effectiveness of the Pro-Kin visual feedback balance system in combination with a weight loss system, this study design has its limitations, such as short training period (only 4 weeks). In addition, the lack of imaging examinations, such as functional MRI, failed to explain the central mechanisms of efficacy; therefore, further improvements to the design are needed in subsequent studies.
Conclusion
In summary, the combined application of the Pro-Kin visual feedback balance and the weight loss systems is beneficial to the recovery of motor function in the early rehabilitation phase and is an effective treatment that promotes early reconstruction of balance and walking ability following a stroke.
Supplemental Material
sj-doc-2-tan-10.1177_17562864241266512 – Supplemental material for Effects of visual feedback balance system combined with weight loss training system on balance and walking ability in the early rehabilitation stage of stroke: a randomized controlled exploratory study
Supplemental material, sj-doc-2-tan-10.1177_17562864241266512 for Effects of visual feedback balance system combined with weight loss training system on balance and walking ability in the early rehabilitation stage of stroke: a randomized controlled exploratory study by Wei Lu, Mingming Wen, Yinxia Li, Feng Liu, Yongping Li, Hengchun Zhang and Min Zhang in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-1-tan-10.1177_17562864241266512 – Supplemental material for Effects of visual feedback balance system combined with weight loss training system on balance and walking ability in the early rehabilitation stage of stroke: a randomized controlled exploratory study
Supplemental material, sj-docx-1-tan-10.1177_17562864241266512 for Effects of visual feedback balance system combined with weight loss training system on balance and walking ability in the early rehabilitation stage of stroke: a randomized controlled exploratory study by Wei Lu, Mingming Wen, Yinxia Li, Feng Liu, Yongping Li, Hengchun Zhang and Min Zhang in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.