
Abstract
Background:
Thrombotic microangiopathy (TMA) is a rare side effect of interferon-beta (IFN-β) therapy. The clinical characteristics of IFN-β-induced TMA are unknown.
Objectives:
To explore the clinical characteristics of IFN-β-induced TMA and provide reference for the prevention of TMA.
Design:
Articles on IFN-β-induced TMA were collected by searching the literature in relevant Chinese and English databases from inception to 31 July 2023.
Methods:
Data in the articles were extracted and analyzed retrospectively.
Results:
Forty-seven patients, with a median age of 41 years (range 22, 66), were included in the analysis. The median time to the diagnosis of IFN-β-induced TMA was 8 years (range 0.1–30) after administration. The main clinical symptoms were neurological symptoms (51.1%), hypertension (78.7%), dyspnea (19.1%), edema (19.1%), asthenia/fatigue (19.1%), and digestive symptoms (17.0%). Most patients presented with hemolytic anemia (76.6%), thrombocytopenia (63.8%), and acute kidney injury (70.2%). All patients stopped IFN-β and received plasma exchange therapy (53.2%), systemic steroids (46.8%), antihypertensive therapy (46.8%), eculizumab (12.8%), and rituximab (12.8%). Kidney damage was not completely reversible; 40.4% of patients achieved renal function and hematology remission, 27.7% developed chronic kidney disease, 25.5% developed end-stage renal disease, and 2.1% died.
Conclusion:
IFN-β-induced TMA is a rare but serious complication that can be life-threatening. It may occur after many years of IFN-β therapy, and patients taking IFN-β should be monitored for symptoms such as headache and hypertension.
Keywords
Introduction
Thrombotic microangiopathy (TMA) is a clinicopathological syndrome caused by microvascular thrombosis and characterized by thrombocytopenia, microangiopathy, hemolytic anemia, and organ dysfunction. Primary TMA includes thrombotic thrombocytopenic purpura (TTP) and atypical hemolytic uremic syndrome (aHUS). 1 TTP is caused by a severe deficiency of the acquired or congenital von Willebrand factor-cutting protease a disintegrin and metalloproteinase with a thrombospondin type 1 motif 13 (ADAMTS13), usually <5%, and aHUS is characterized by an inability to regulate alternative complement pathways. 2 Secondary thrombotic microvascular disease is secondary to infection, autoimmune diseases, malignant tumors, pregnancy, drugs, transplantation, and malignant hypertension. 3 Drug-induced TMA accounts for 10%–13% of all TMA cases and approximately 26% of secondary TMA cases, with drugs representing the third most frequent cause of TMA after pregnancy and infection. 3
Interferon-beta (IFN-β) is a cytokine produced by fibroblasts, leukocytes, etc., that has antiviral, anti-proliferative, and immunomodulatory activity. 4 IFN-β can be used as a first-line treatment for multiple sclerosis (MS). 5 Flu-like symptoms, injection site reactions, asthenia, hypertonia, and menstrual disorder are common adverse reactions to IFN-β. 6 TMA was first reported as a rare adverse reaction to INF-β in 1998. 6 What is known about IFN-β-induced TMA has been learned from case reports, and the specific clinical features are unclear. We investigated the clinical characteristics of IFN-β-induced TMA through a retrospective analysis, and here, we provide recommendations for the prevention and treatment of TMA.
Methods
Data sources
Case reports, case series, and clinical studies of IFN-β-induced TMA were collected by searching both Chinese and English databases, including the PubMed, Embase, Web of Science, Cochrane Library, Scopus, China National Knowledge Infrastructure, WanFang, and VIP databases, until 31 July 2023. Medical subject terms included TMA, MS, hemolytic uremic syndrome, TTP, interferon, and IFN-β.
Inclusion and exclusion criteria
Case reports, case series, and clinical studies of IFN-β-induced TMA were included. Duplicate publications, reviews, and animal studies were excluded.
Data collection
The following clinical information of patients was recorded in a self-designed data extraction table: sex; age; medical history; concomitant drugs; indication; IFN-β administration information (type, dose, frequency, and time); clinical symptoms and signs; laboratory indicators, including serum creatinine, lactate dehydrogenase (LDH), platelet count (PLT), hemoglobin (Hb), and presence of schistocytes; ADAMTS13 activity and complement mutation; kidney histopathological findings; brain imaging findings; and the treatments and outcomes of TMA.
Definitions
Hematological remission of TMA was defined as the normalization of the platelet count and LDH levels in two consecutive measurements over a 4-week period. Renal remission was defined as an improvement in the serum creatinine level of more than 25% compared to the worst value. Complete remission of TMA was defined as hematological and renal remission.
Statistical analysis
SPSS 20.0 software (IBM Corp., Armonk, NY) was used for descriptive statistical analysis of the collected data. Continuous data are expressed as the median (range, minimum, maximum), and count data are expressed as n (%).
Results
Basic information
A total of 32 studies with 47 patients meeting the inclusion criteria were retrieved. The basic information of the 47 patients is shown in Table 1. The median age of the 47 patients was 41 years (range 22, 66), and there were 11 males (23.4%), 24 females (51.1%), and 12 (25.5%) individuals for whom sex was not reported. IFN-β was used primarily for the treatment of MS in 46 patients (97.9%) and chronic hepatitis C in 1 patient (2.1%). Of the 14.9% who were concomitantly treated with other drugs, as listed in Table 1, it should be noted that none of these agents are known to be associated with a TMA.
Characteristics of the 47 patients with interferon-beta-induced thrombotic microangiopathy.
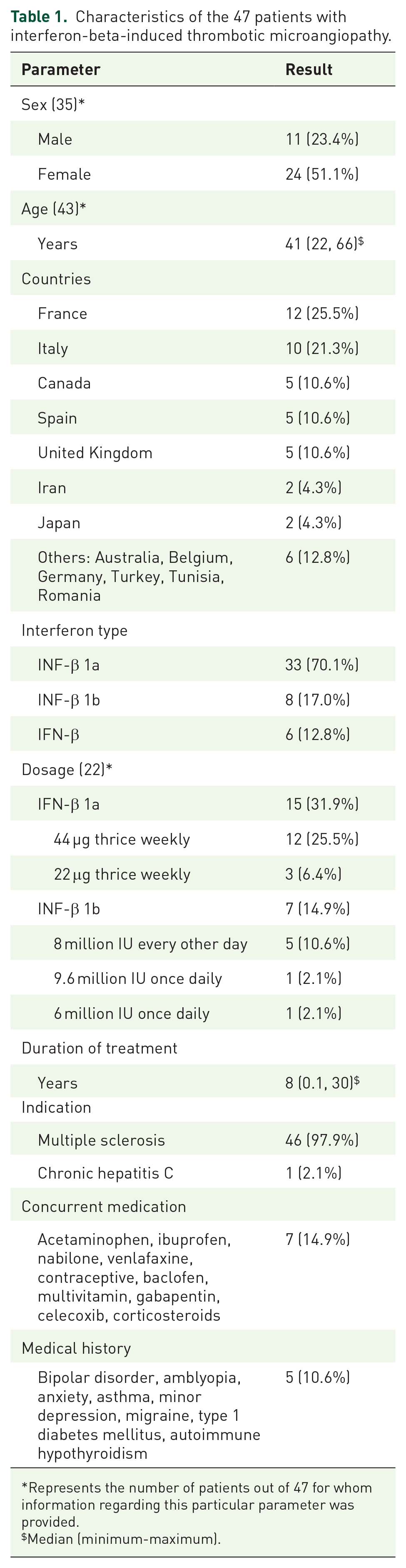
Represents the number of patients out of 47 for whom information regarding this particular parameter was provided.
Median (minimum-maximum).
IFN-β administration
IFN-β-1a was used in 33 patients (70.1%), IFN-β-1b in 8 patients (17.0%), and no type was described for 6 patients (12.8%). The dose of IFN-β-1a was described for 15 patients (31.9%), including 12 patients (25.5%) with 44 µg thrice weekly and 3 patients (6.4%) with 22 µg thrice weekly. IFN-β-1b dosages were described in 7 patients (14.9%), including 5 patients (10.6%) at 8 million IU every other day and 1 patient each at 9.6 million IU once daily and 6 million IU once daily. The median time for TMA to develop was 8 years (range 0.1, 30) after IFN-β administration.
Clinical symptoms
The clinical symptoms of IFN-β-induced TMA are detailed in Table 2. Hypertension occurred in 37 patients (78.7%), of whom 25 (53.2%) had malignant hypertension. The median systolic and diastolic blood pressure values were 200.5 mmHg (range 170, 250) and 120 mmHg (range 80, 150), respectively. Nine (19.1%) patients showed asthenia/fatigue, and eight (17.0%) patients showed dyspnea. Nine patients (19.1%) had edema, including facial edema, pulmonary edema, papillary edema, lower limb edema, and peripheral edema. Digestive tract symptoms, including nausea, vomiting, anorexia, and abdominal pain, were observed in eight patients (17.0%). The other symptoms could be characterized as fever, purpura, epistaxis, and gingival hemorrhage.
Clinical symptoms and imaging examination findings of the 47 patients with interferon-beta-induced thrombotic microangiopathy.

Represents the number of patients out of 47 for whom information regarding this particular parameter was provided.
Median (minimum, maximum).
ADAMTS13, a disintegrin and metalloproteinase with thrombospondinmotifs13; CFHR, complement H-related proteins; CT, computed tomography; MCP, membrane cofactor protein; MHT, malignant hypertension; MRI, magnetic resonance imaging; PRES, posterior reversible encephalopathy syndrome.
Neurological signs occurred in 24 (51.1%) patients, mainly headache (14 cases, 29.8%) and seizures (8 cases, 17.0%), visual disturbance (4 cases, 8.5%), confusion (4 cases, 8.5%), and syncopal attack (3 cases, 6.4%).
Laboratory examination
The renal and hematological manifestations of IFN-β-induced TMA are shown in Table 3. Thirty-six (76.6%) patients developed hemolytic anemia, with a median hemoglobin value of 7.7 g/dL (range 4.4, 11.4). Thrombocytopenia was present in 30 of 35 patients, and the median platelet count was 62 × 109/L (range 4, 122). The results of peripheral blood smears were reported for 25 patients, all of whom showed the presence of schistocytes. LDH levels were reported for 33 patients (70.2%), 32 of whom had elevated LDH, with a median value of 1160 IU/L (range 315, 1929 U/L). Of the 47 patients evaluated, 33 (70.2%) developed acute kidney injury (AKI), and the median serum creatinine was 3.0 µ/dL (range 1.7, 13.8). Urine analysis of 21 patients showed proteinuria in 21 patients and hematuria in 12 patients (25.5%).
Laboratory examination findings of the 47 patients with interferon-beta-induced thrombotic microangiopathy.

Represents the number of patients out of 47 for whom information regarding this particular parameter was provided.
Median (minimum, maximum).
AKI, acute kidney injury.
ADAMTS13 activity was measured in 20 patients, and no activity was detected in three patients (6.4%). Complement gene mutation analysis in 13 patients revealed heterozygous membrane cofactor protein (MCP) mutations in one patient (2.1%) and heterozygous complement H-related protein (CFHR1-R3) deletions in three patients (6.4%).
Histopathology
Renal biopsy was performed in 23 patients. Glomeruli showed ischemic changes (six cases, 12.8%), mesangial cell proliferation (three cases, 6.4%), mesangiolysis (three cases, 6.4%), glomerular basement membrane reduplication (four cases, 8.5%), and capillary occlusion and stenosis (three cases, 6.4%). Renal arterioles showed vessel narrowing with thrombi (six cases, 12.8%), luminal obliteration (five cases, 10.6%), and arteriolar wall thickening and intimal onion skin-like swelling (eight cases, 17.0%). Renal tubules showed tubular atrophy, microvacuolization and protein cylinders (four cases, 8.5%). The renal interstitium showed lymphomonocytic infiltration (four cases, 8.5%). Immunofluorescence showed IgM, C1q, and fibrinogen deposits.
Brain imaging
Cerebral magnetic resonance imaging (MRI) was performed in 13 patients (27.7%), of whom 9 (19.1%) showed posterior reversible encephalopathy syndrome (PRES). Among four patients (8.5%) who underwent computed tomography, PRES was found in one patient.
Treatments and outcomes
The treatments and outcomes of IFN-β-induced TMA are detailed in Table 4. All patients discontinued IFN-β, and 22 patients (46.8%) received antihypertensive therapy. Twenty-five patients (53.2%) underwent plasma exchange (PE), 22 patients (46.8%) received systemic steroids, and 6 patients (12.8%) received eculizumab and rituximab. Other treatments included fresh frozen plasma infusion, red blood cell transfusion, platelet mass transfusion, vincristine, and cyclophosphamide. Nine patients (19.1%) achieved TMA remission by directly discontinuing IFN-β and did not require additional treatment. Nineteen patients (40.4%) achieved renal function and hematological remission, 13 patients (27.7%) developed chronic kidney disease, 12 patients (25.5%) developed end-stage renal disease (ESRD), and 1 patient (2.1%) died. Preexisting hypertension was reported in only 19 patients (40.4%) after TMA resolution.
Treatments of interferon-beta-induced thrombotic microangiopathy and patient outcomes.

Represents the number of patients out of 47 for whom information regarding this particular parameter was provided.
ESRD, end-stage renal disease; FFP, fresh frozen plasma; PE, plasma exchange; PMT, platelet mass transfusion.
Discussion
Drug-induced TMA may be an acute, immune-mediated disease or may be the result of progressive, dose-dependent toxicity. 7 The immunomodulatory activity of interferon therapy has been described to induce autoimmune diseases. The presence of drug-dependent antibodies against ADAMTS-13 together with decreased anti-ADAMTS-13 activity are reported for interferon. 8 Type I interferon-induced TMA in experimental models has a dose-dependent toxic effect on the microvasculature. 9 Interferon alpha (IFN-α) has been repeatedly described in relation to the development of TMA.10,11 IFN-β-induced TMA was independent of IFN-β type. IFN-β-1a differs from β-1b in the presence of glycosylation. 12 This suggests that glycosylation may not be related to IFN-β-induced TMA. At least half of IFN-β-induced TMA patients are female, which may be related to the fact that MS primarily affects women. 13 However, female sex cannot be ruled out as a risk factor for IFN-β-induced TMA. TMA appeared at a median time of 8 years after IFN-β treatment. This suggests that the late onset of TMA is the result of the cumulative effects of IFN-β on the kidneys and systemic micro vessels. Low body mass index may be another risk factor for IFN-β-induced TMA. IFN therapy may lead to dose-dependent TMA at high dosages for weight. 9 Although IFN-β is used in conjunction with other drugs, there is currently no literature describing concomitant drug-induced TMA.
Patients with TTP have very low platelet counts (usually <20 × 109) and relatively mild renal impairment. Compared with TTP, patients with aHUS have less thrombocytopenia (usually >30 × 109) and more severe renal impairment. 14 Patients with IFN-β-induced TMA were more likely to have aHUS than TTP. Among TMA types, neurological involvement is most frequent in IFN-β-induced TMA. The most common symptom is severe headache, followed by seizures, confusion, and visual disturbance. MRI reveals brain lesions compatible with PRES. MHT is found in 25% of patients presenting with hypertension among IFN-β-induced TMA cases. In individual cases, hypertension is also associated with Raynaud’s phenomenon. 15 Hypertension often requires control with multiple antihypertensive medications and persists after the resolution of TMA. Given that half of the patients did not have schistocytes, it is recommended to use kidney or normal skin biopsy to detect C5b-9 complement complex deposition in the diagnosis of TMA and as an adjunct examination to determine whether TMA may be responsive to eculizumab.16,17
The underlying mechanism of IFN-β-induced TMA is not fully understood. The different forms of TMA share a common feature of endothelial cell injury of diverse origins. Mutations of complement proteins such as CFH, C3, CFI, CFB, or MCP are clearly associated with the development of primary TMA with deregulated activity of the complement system. 18 Drug-induced TMA could be linked to direct endothelial toxicity. The association between complement activation and endothelial damage has not been demonstrated for drug-induced TMA. It is currently believed that the development of TMA involves a ‘two-hit’ mechanism, with a combination of genetic background and triggers. 7 Variants in complement genes play an important role in the pathogenesis of primary TMA. 19 Genetic variants in complement genes are found in less than 10% of drug-induced TMA patients, 20 and only a small number of patients with drug-induced TMA have been reported to have potential causative complement variants. 21 Approximately one-third of patients with malignant hypertension may present with TMA, of which complement abnormalities are found in 35–65%. 22 Therefore, complement abnormalities should be suspected in patients with TMA in the setting of malignant hypertension.
The ADAMTS13 viability test is helpful in TMA diagnosis, the formulation of treatment regimens, and the monitoring of disease progression and prognosis. 23 Plasma ADAMTS13 activity is zero (or almost undetectable) in patients with familial TTP as a result of homozygous (or double heterozygous) mutations in two 9q34 genes encoding ADAMTS.24,25 During an episode of acquired idiopathic TTP, patients usually have undetectable or barely detectable plasma levels of ADAMTS. 26 Immunoglobulin G (IgG) antibodies (possibly autoantibodies) that inhibit plasma enzyme activity are present in 48–80% of patients, which may be associated with transient (or intermittent) deficits in immune regulation.24,27 In the patients we studied, ADAMTS 13 deficiency may be due to autoantibodies against various epitopes of this protease during IFN-β treatment.
Standardized treatment options for TMA are not available. The cessation of IFN-β therapy is critical. IFN-β-induced TMA in some patients is dose-dependent and usually resolves after discontinuation without the need for other treatment. According to the patient’s condition, PE and/or steroids are given along with symptomatic treatment, such as antihypertensive therapy, blood transfusion, and treatment for anemia. 1 Conventional approaches to managing this entity, such as PE or steroids, obtained limited improvement, with high rates of renal failure. Monoclonal antibodies such as rituximab and eculizumab may be an option for refractory secondary TMA. According to a review of the literature, rituximab and eculizumab have been used with marked effectiveness for TMA secondary to therapy with clopidogrel, quinine, gemcitabine, and cisplatin and calcineurin inhibitors.28–31 aHUS patients can benefit from treatment with eculizumab, an inhibitor of terminal complement activation, due to uncontrolled complement activation, whereas TTP patients can benefit from immune therapy with rituximab, an anti-CD20 monoclonal antibody used in autoantibody-mediated diseases. Treatment with PE or eculizumab remains a controversial issue. Additionally, the optimal timing of monoclonal antibody treatment is still unknown. Based on existing experience, patients can be given eculizumab immediately after a course of unsuccessful PE therapy. 32 It should be noted that patients with IFN-β-induced TMA have a poor prognosis despite treatment with PE, steroids, and monoclonal antibodies. Nephrotoxicity can be a serious and irreversible complication, with some patients progressing to advanced chronic kidney disease (CKD) and ESRD. In addition, hypertension usually persists after the resolution of TMA.
Limitations
There are limitations to the study. First, the data are based on case reports and case series, which contain more unknowns than controlled studies. Second, complete clinical data were not available for all patients; for example, less than half of the patients had schistocyte presence, renal biopsy findings, and ADAMTS13 activity documented. Third, the number of patients in this sample is small, and more clinical studies are needed to demonstrate the efficacy of monoclonal antibodies in drug-induced TMA.
Conclusion
Clinicians should be wary of IFN-β-induced TMA as a rare complication. Symptoms such as headache and hypertension should be carefully monitored in patients receiving interferon beta therapy. The clinical presentation of IFN-associated TMA is often severe, and the renal prognosis is often poor. Early identification of TMA can prevent its further development, and the interruption of IFN treatment is warranted.