
Abstract
Background and Aims:
In multiple sclerosis (MS), non-adherence/non-persistence is related to suboptimal response to treatment, including disease relapses and the need for more expensive healthcare. The aim of this study was to identify predictors related to adherence to disease modifying therapies (DMTs) in a cohort of Argentinian MS patients.
Methods:
We conducted a cross-sectional study at the National Medical Care Program from Argentina. MS patients with at least one claim for a DMT from 1 January 2017 to 1 October 2017 were identified. A telephone survey was performed to assess clinical and demographic factors. The medication possession ratio (MPR) was used to estimate adherence; MPR <80% defined non-adherence. Associations were studied using a logistic regression model.
Results:
Our database included 648 MS patients. A total of 360 patients (60% females, mean age 55.3 years) accepted to participate. Of these, 308 (85.5%) patients were receiving DMT at the time of the survey. Some 198 (63.7%) were receiving injectable therapies. Optimal adherence was 47.7%. Adherence was associated with oral medication [odds ratio (OR) 1.83 95% confidence interval (CI) 1.13–3.00, p = 0.014]. A factor related to oral drugs was higher educational level (OR 2.86 95%CI 1.41–5.81, p = 0.004).
Conclusion:
This real-world study showed better adherence and persistence on treatment with oral therapies in MS patients in Argentina.
Introduction
Multiple sclerosis (MS) is a chronic, immune mediated, and neurodegenerative disease that generates physical, cognitive, and emotional disabilities. It affects young people with a female predominance.1,2 Progression in MS varies from person to person. Furthermore, the various types of MS disease also progress in different ways. Most people with MS experience an increase in physical disability at some point and it worsens (progression) when disease activity causes neurodegeneration. 3 Several disease-modifying therapies (DMTs) have shown efficacy in reducing relapse frequency and progression of disability, and improving quality of life in patients with MS (PwMS).
In general, only half of patients with chronic diseases have optimal adherence to treatment. 4 Adherence to treatment (also referred to taking medication according to the dosage of the prescribed program) and persistence to treatment (i.e., continuation of treatment by the patient from the beginning to the interruption of treatment for any reason) of DMTs are both critical for the achievement of optimal outcomes in PwMS. Different studies on DMT have shown that multiple factors may affect adherence and persistence, including patients who are tired of chronic treatment, perceived loss of efficacy, adverse reactions, injection device problems, and dosing frequency. 5
Adherence and persistence rates to DMTs in MS range from 49% to 88%. 1 Identification of these factors might contribute to the planning of disease management programs, improving the prognosis and quality of life of patients. 3 Few previous studies have evaluated adherence to treatment in MS in Latin America. The aim of the present study is to identify predictors related to adherence and persistence to DMTs in a cohort of Argentinian MS patients.
Methods
A cross-sectional study was conducted in a cohort of PwMS older than 18 years included in the drug dispensing database from the National Medical Care Program (PAMI) between 1 January 2017 and 1 October 2017, in Argentina. The pharmacy database had only 9 months of follow up available at the time we accessed it. PAMI is a government-funded social insurance program which serves 5 million people older than 65 years, people with disabilities unable to work, pensioners, and war veterans. 6 PwMS receiving DMT were included.
From October 2019 to May 2020, a brief telephone survey (Supplemental Material) was conducted by neurologists and previously trained medical students. Patients were contacted at least twice at different times. The protocol was approved by the Research Ethics Committee of the César Milstein Hospital (Number 14-2019 / 27.06.2019). Oral informed consent was given by telephone by all participants (see supplemental material).
Outcome variables
The medication possession rate (MPR) was used to estimate adherence and was defined as the number of daily doses of drugs dispensed by the pharmacy to each patient divided by expected drug collection during the study period, expressed as a percentage. A MPR ⩾80% was considered adherent and < 80% as non-adherent. Adherence was modeled as a categorical variable.
Predictor variables
Data were collected in the following four groups:
Patient-related
Patient-related factors were age, sex, family environment, educational level, associated comorbidities, including cardiovascular diseases (arrhythmias, congestive heart failure, valvular disease, myocardial infarction), liver disease, chronic lung disease, diabetes, autoimmune diseases (systemic lupus erythematosus, rheumatoid arthritis, Hashimoto’s disease, myasthenia gravis), and cancerous tumor. 7 Cognitive complaint was also included (using a 5-point Likert scale).
Disease-related
We collected data on disease duration (<10 years / >10 years), presence of relapse, steroid treatment and hospitalizations in the previous year, fatigue quantified with the Fatigue Impact Scale of Daily Use (D-FIS), 8 depression assessed using the PHQ-2 scale, 9 and disability measured with the Patient Determined Disease Scale (PDDS). 10
Drug-related
Information on drug selection (chosen only by treating doctor / shared with patient), DMT forgotten (by 5-point Likert scale), presence of adverse effects, polypharmacy (defined as ⩾5 drugs per day), and route of administration (injectable: subcutaneous/intramuscular/intravenous versus oral) were collected.
Health-system-related
Information on neurological appointments per year, delay in the delivery of DMT, administrative requirements per year, and person in charge of carrying out the administrative paperwork were noted.
Statistical analyses
Based on the results, descriptive statistics of categorical variables were reported as absolute frequency and percentages. Continuous variables were described as mean and standard deviation (SD) or median values and interquartile range (IQR) according to the data distribution. The Shapiro–Wilk test was applied to evaluate normal distribution of variables. A bivariate model and three logistic regression models were constructed to estimate odd ratios (ORs) to identify possible factors independently associated with adherence to DMT.
The first model included age, sex, educational level, memory disorders, family environment, and comorbidities as demographic predictors. The second model included the predictors of the disease: duration time, relapses, hospitalizations, use of steroids, fatigue, depression, and current disability. The third model included predictors of the drug used: drug choice, forgetting medication, medication supervision, adverse effects, polypharmacy, and route of administration. The fourth model included predictors of the health system: neurological appointments, person in charge of administrative burden, administrative requirements, and delay in delivery of DMT.
Adherence as an event of interest was coded as 1. The Kruskal–Wallis nonparametric analysis test was used to estimate differences in the relevant subgroups of drugs used. The sample size was calculated based on an event rate of 35.5% according to our previous study11 with the intention of including at least 8 predictor variables in the model. Taking into account the rule of thumb, 10 events are needed for each variable included in the model. 12 According to this calculation, a minimum of 240 participants needs to be included. We allowed for 20% of possible missing data or data errors and increased the sample to a minimum of 288 participants. Data analysis was conducted using the STATA 13, Stata Statistical Software: Release 13. StataCorp LP, College Station, TX, USA. For all analyses, p values < 0.05 were considered statistically significant.
Results
Of the 648 patients registered in our database, only 360 were contacted by phone, with a survey response rate of 55.5% (Figure 1). Clinical and demographical data of the population included are shown in Table 1. The mean age was 55.3 years (SD 12) with a female predominance (60%). At the time of the survey, 308 (85.5%) patients were receiving DMT. The remaining 52 (14.5%) had non-persistence to treatment: 30 patients (57.7%) due to a lack of authorization from their health insurance provider and 22 (42.3%) because of medical decisions.
Demographic characteristics among non-adherent and adherent: bivariate model.
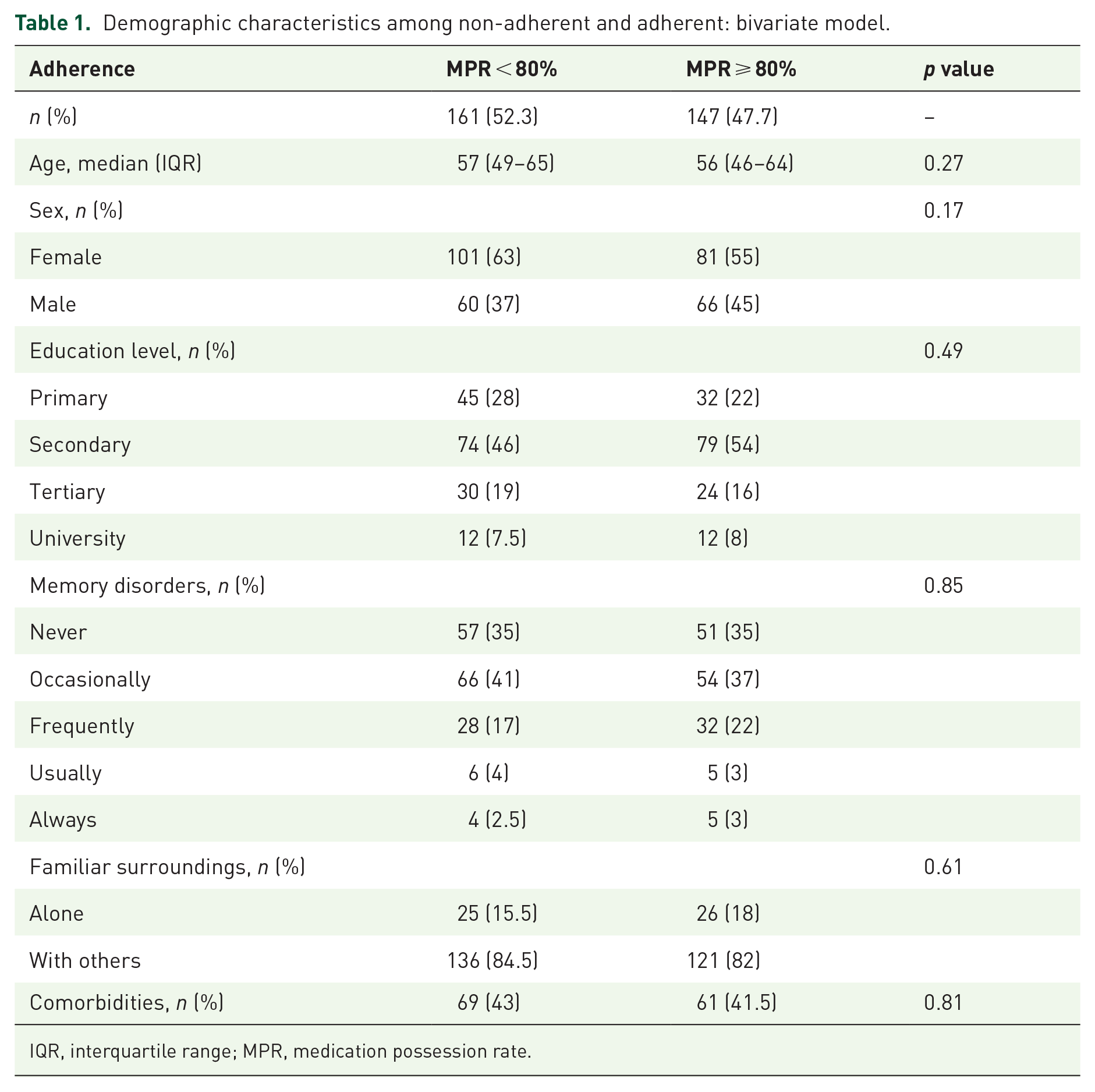
IQR, interquartile range; MPR, medication possession rate.

Flow chart.
As shown in Table 2, 156 (43%) patients had comorbidities. A total of 103 PwMS reported depression, resulting in a prevalence of depression of 33.4%, and 201 (55.5%) had limitations in gait and mobility (Figure 2).
Comorbidities in MS patients.
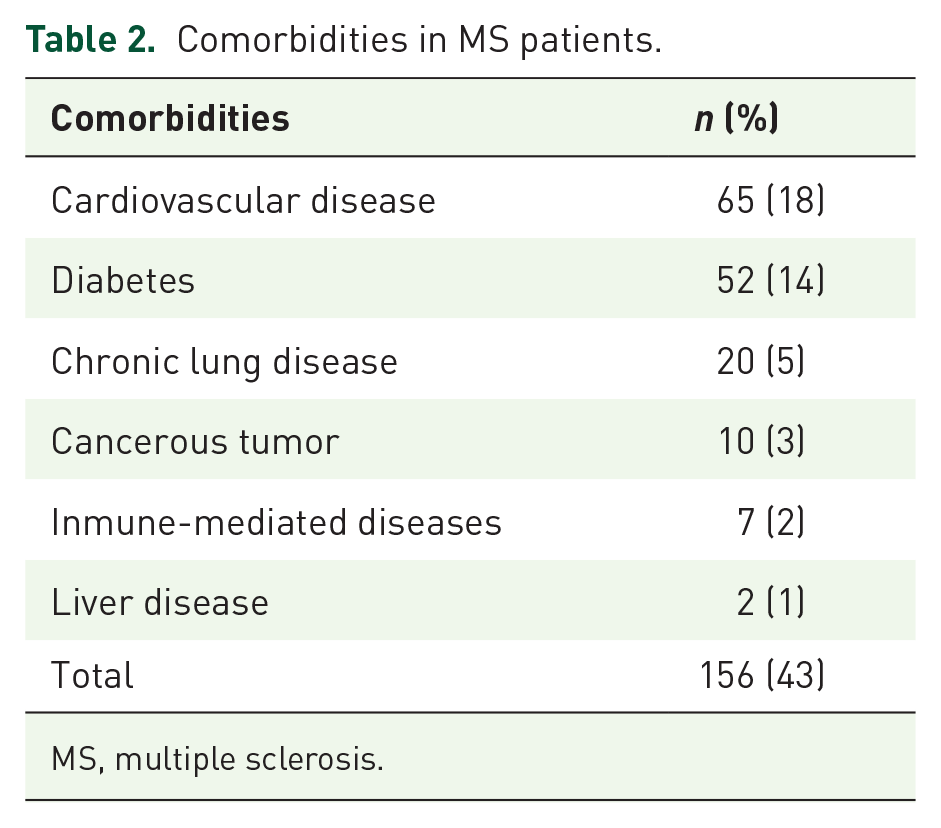
MS, multiple sclerosis.

PDDS Score.
Of the PwMS under treatment, 147 (47.7%) were adherent to their DMT. Median adherence was 78% (IQR 56–100). As shown in Figure 3, the median distribution of adherence was greater among oral drugs compared with injectables. The parenteral route of administration was the most used in 197 (64%) PwMS, as shown in Table 3. We detected that 86 (27%) patients had adverse effects that could affect the persistence of treatment, among them: 36 (11%) were intolerant to injectables, 26 (8.2%) experienced digestive intolerance, 12 (3.8%) had lymphopenia, 9 (2.8%) showed infections, 2 (0.63%) suffered uncontrolled hypertension, and 1 (0.31%) suffered thrombocytopenia.
DMTs used.

DMT, disease-modifying therapy.

Median adherence to injectable versus oral therapies. Expressed CI 5–95% and IQR 25–75%. Self-injectables: IFN, AG. Injectables: NTZ, ALZ. Oral: DMF, FG, TF, CLD.
In the multivariate model, we found an association between the oral route of administration and adherence (OR 2.02, 95% CI 1.24–3.29, p = 0.005). Figure 4 shows the median adherence of each drug. In a secondary post hoc analysis, we found that the main demographic predictor for those who received oral treatment was tertiary or universitary educational level (OR 2.86, 95% CI 1.41–5.81, p = 0.004).
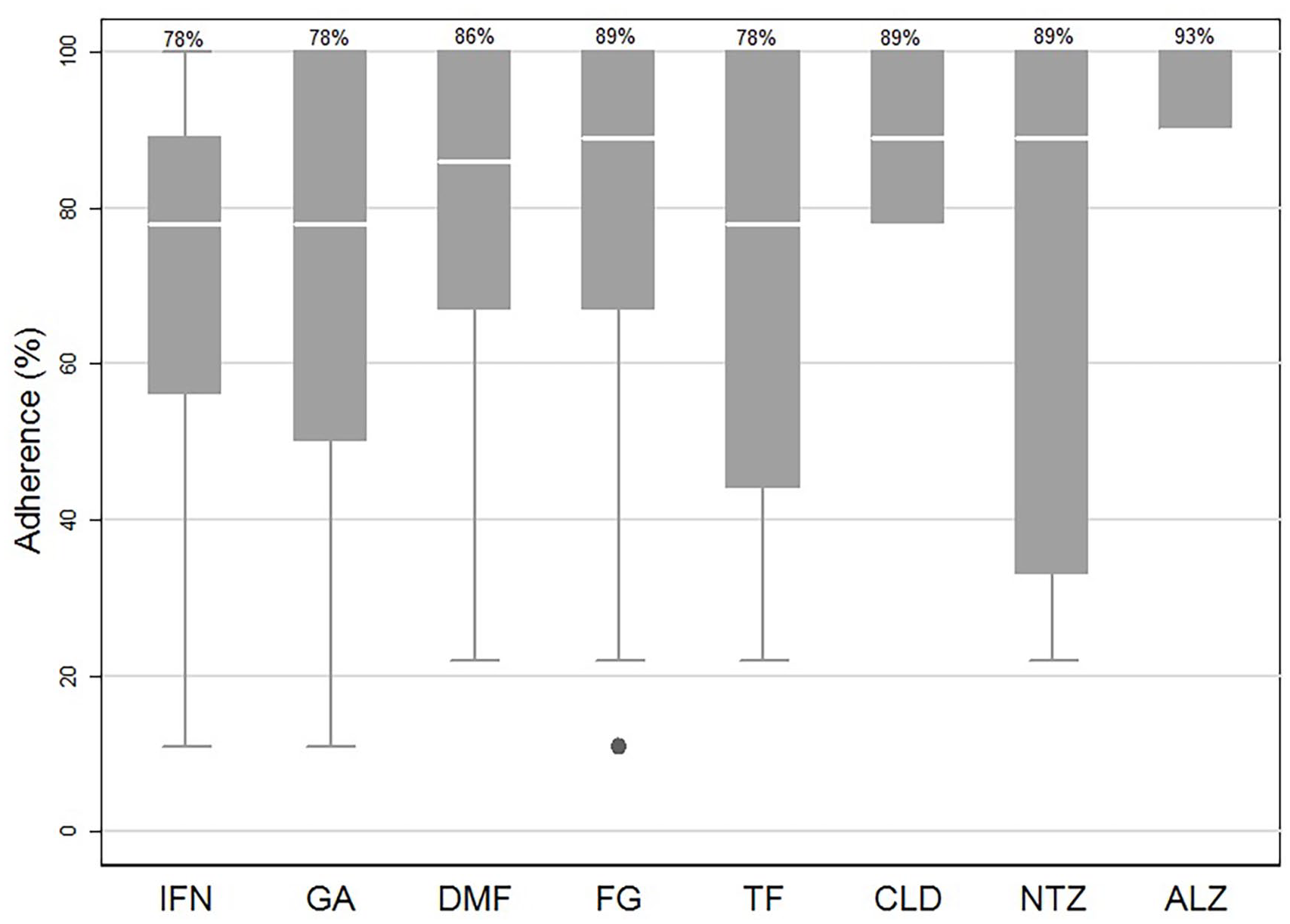
Median of adherence according to DMTs. Expressed confidence interval 5-95% and interquartile range 25-75%
Different variables that could affect adherence to treatment were evaluated, as summarized in Table 4.
Characteristics of the disease, drug used, and health system associated with adherence and persistence to DMTs: logistic regression model.

P <0.05, statistically significant.
DMTs, Disease-modifying therapies; OR, Odds Ratio; CI, confidence interval; IQR, interquartile range; D-FIS, Fatigue Impact Scale for Daily Use; PDDS, Patient Determined Disease Scale.
No statistically significant association in demographic, disease, or health system variables was found. We detected a decrease in adherence, which did not reach statistical significance, among the number of neurological appointments per year and the person in charge of carrying out the administrative burden.
Discussion
The results of this cross-sectional study showed that approximately 5 out of 10 PwMS were non-adherent/non-persistence to treatment. Adherence has been defined by the World Health Organization (WHO) as “the degree to which the person’s behavior corresponds with the agreed recommendations from a health care provider” (WHO, 2003), 13 while persistency refers to the amount of time that a patient remains on chronic drug therapy. 14 Adherence to treatment in MS varies according to the quantification method used. 15 Our results were superior to those described by Hansen et al., who showed an adherence of 30–40%, although lower than those reported by other researchers, which varied between 59.6% and 76.4% in different studies.16 –19
Of the 21 variables analyzed, only the route of drug administration had significant implications for non-adherence/non-persistence. We identified that patients who used the injectable route were more likely to be non-adherent. Several previous studies obtained similar findings to the present study.20 –22 Better adherence to oral drugs is probably due to an easier administration and the absence of injection-related issues. 20 Nonetheless, other studies have not found differences between oral and injectable DMTs.3,23 –25 Patients with comorbid diseases have shown difficulties in adhering to the proposed medication. 26
One third of our PwMS reported symptoms suggestive of depression. The prevalence data ranges from 19 to 54% in PwMS. 27 Depression showed an association with non-adherence in several studies.3,28 Tarrants et al. showed that patients with depression were half as likely to be adherent to their treatment. 32 Memory disorders also negatively affect adherence. 28 About 68.5% of the PwMS reported worsening memory symptoms. Similar results were obtained by Tremlett et al. 27 In our study, we did not find cognitive disorders are a predictor of adherence. However, our study did not use any specific test to evaluate this variable.
Only 27.5% of the PwMS expressed shared decisions between doctor and patient regarding drug election. A previous study from our country revealed that the frequency of shared decisions ranges between 76% and 79%. 30 The disparity of values is probably due to differences in the population included. Ben-Zacharia et al. 1 described that patients obtained better levels of adherence when the therapeutic decision was shared.
More than one-third of the patients reported having forgotten to take the medication. Between 16% and 51% missed at least 1 dose of their medication in the short and long term. Unlike other authors, we did not find an association with adherence.24,27,31, Besides that, between 45% to 62% of patients discontinued the treatment due to adverse events.30,32–34 A quarter of our PwMS presented adverse events that justified discontinuation of treatment. Previous studies have investigated polypharmacy and its consequences in lower adherence patients.26,30 We obtained a polypharmacy prevalence rate of 35.5%, while, in a recent review, the reported rate varies between 15% and 59%. 32
Several studies showed that short disease duration and the absence of clinical relapses determined better adherence.26,31,35 A minority of patients reported hospitalizations for MS in the previous months. Two studies showed that adherent patients were less likely to have MS-related hospitalizations in the previous 6 months and in the subsequent 12 months. This suggests a 50% decrease in the hospitalization rate in adherent patients.17,25
The patients who reported symptoms of fatigue did not show an impact on therapeutic adherence, similar to that reported by Van Gaudecker. 36 In contrast, other authors showed a relationship between fatigue and non-adherence.33,37 The assessment of disability with adherence showed mixed results.21,35 More than half of our PwMS required assistance to walk. Unlike Pengxiang et al., we did not find an association between current disability and adherence. 25
Our patients had 3.8 neurological visits on average per year. This association was previously studied and it evidenced a greater number of outpatient medical visits (mean 5.6/year) in adherent patients. 23 Missing more than 20% of scheduled appointments was identified as the most important factor associated with suboptimal adherence. 18
In our country, 32.3% of the PwMS expressed problems obtaining the medication from the medical insurance provider. 37 Those with a state-run health insurance reported a longer waiting time (4.5–6 weeks) for first prescription and maintenance of therapies and inappropriate delivery of DMT compared with other types of medical insurance. 38 As a requirement of health insurance policy, medication for MS is requested through chronic medication forms, which must be updated every 6 months. Our PwMS reported a waiting time of 2 weeks for administrative procedures, which could delay the start and/or continuity of treatment.
Given the heterogeneity in the data currently available, we consider it essential to continue this line of research to establish more predictor variables, facilitating the correct selection of treatment, and taking into account the possible barriers that could affect adequate adherence when starting a new therapy.
Several limitations in this study should be noted. Firstly, this was a cross-sectional study and it is not possible to assess changes over time to explore causality. Secondly, our response rate was 55%, as is the case in most telephone surveys,39,40 which could introduce selection bias because the characteristics of the participants who respond and those who do not can differ. Third, this cohort is limited to patients with PAMI medical insurance. This population has distinctive characteristics, such as advanced age, long duration of disease, and high use of injectable therapies. Since only this particular health system was evaluated, we suggest being cautious when drawing conclusions and extrapolating the findings to other populations.
Fourthly, we do not have direct clinical data related to adherence provided by physicians (e.g., medical reasons, therapeutic failure, progressive forms, adverse effects). This study cannot distinguish between non-persistent patients (who could restart a new treatment in the future) from those who definitively discontinued treatment. 14 Finally, there is no data on PwMS medicated with peginterferon beta 1a and Ocrelizumab, both recently approved in our country at the time of the study. Despite these limitations, this study provides an initial approach to the potential variables that could affect adherence to treatment in PwMS not previously evaluated in Argentina and this warrants further study.
In conclusion, adherence is a key factor when optimizing management of PwMS. In this real-world study, we showed better adherence and persistence to oral therapies in MS patients in Argentina. This result should be considered by the healthcare professional when evaluating the risk of non-adherence/non-persistence with therapies. It is essential to implement efforts to improve treatment adherence, disease care, and patients’ quality of life and to reduce public health costs for MS patients.
Supplemental Material
sj-docx-1-tan-10.1177_17562864211031099 – Supplemental material for Predictors of adherence and persistence to disease-modifying therapies in Multiple Sclerosis
Supplemental material, sj-docx-1-tan-10.1177_17562864211031099 for Predictors of adherence and persistence to disease-modifying therapies in Multiple Sclerosis by Gisela Zanga, Estefania Drzewiscki, Paula Tagliani, Maximiliano Smietniansky, Maria M. Esnaola y Rojas and Diego Caruso in Therapeutic Advances in Neurological Disorders
Footnotes
Acknowledgements
We would like to thank Maria Celica Ysrraelit for her valuable recommendations on the manuscript, as well as the following people who have put the time and effort in collecting the data presented in this work: Gabriela Costa, Federico Ramos, Gonzalo Lage, Carlos Turzio, Florencia Tucillo, and Martin Arnedillo.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GZ disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this study was supported by a research grant awarded by the Florencio Fiorini Foundation. The article processing charges was funded by Roche.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.