
Abstract
Primary central nervous system lymphoma (PCNSL) is a rare and aggressive extranodal non-Hodgkin lymphoma (NHL), confined to the brain, eyes, spinal cord or leptomeninges without systemic involvement. Overall prognosis, diagnosis and management of PCNSL differ from other types of NHL. Prompt diagnosis and initiation of treatment are vital to improving clinical outcomes. PCNSL is responsive to radiation therapy, however whole-brain radiotherapy (WBRT) inadequately controls the disease when used alone and its delayed neurotoxicity causes neurocognitive impairment, especially in elderly patients. High-dose methotrexate (HD-MTX)-based induction chemotherapy with or without autologous stem cell transplantation (ASCT) or reduced-dose WBRT leads to durable disease control and less neurotoxicity. The optimal treatment has yet to be defined, however HD-MTX-based induction chemotherapy is considered standard for newly diagnosed PCNSL. Ongoing randomized trials address the role of rituximab, and of consolidative treatment using ASCT or reduced-dose WBRT. Despite high tumor response rates to initial treatment, many patients have relapsing disease with very poor prognosis. The optimal treatment for refractory or relapsed PCNSL is poorly defined. The choice of salvage treatment depends on age, previous treatment and response, performance status and comorbidities at the time of relapse. Novel therapeutics targeting underlying tumor biology include small molecule inhibitors of B-cell receptor, cereblon, and mammalian target of rapamycin signaling, and immunotherapy programmed cell death 1 receptor inhibitors and chimeric antigen receptor T cells.
Keywords
Epidemiology
With an incidence of 0.44 per 100,000, primary central nervous system lymphoma (PCNSL) accounts for approximately 2% of all primary central nervous system tumors. 1 PCNSL is a rare but aggressive form of extranodal non-Hodgkin lymphoma (NHL) limited to the brain, spinal cord, leptomeninges or eyes. 2 The median age at diagnosis is 65 years. Since 2000, there has been an increase in the overall incidence of PCNSL, especially in the elderly. The 5- and 10-year survival rates for PCNSL are 29.9% and 22.2%, respectively. 1
Molecular pathogenesis
Approximately 90% of PCNSL cases are diffuse large B-cell lymphomas (DLBCLs), with the remainder consisting of T-cell (2%), Burkitt’s, lymphoblastic and low-grade lymphomas. 3 PCNS DLBCL is recognized as a distinct subtype of DLBCL in the World Health Organization Classification 4 and expresses pan B-cell antigens (CD19, CD20 and CD79a).5–7 Melanoma associated antigen (mutated) 1 (MUM1)/interferon regulatory factor 4 (IRF4) is nearly always positive; B-cell chronic lymphocytic leukemia (CLL)/lymphoma 6 (BCL-6) is expressed in about 50% of cases; B-cell CLL/lymphoma 2 (BCL-2) is variably expressed; and CD10 is expressed in only a small minority of cases (about 10%).5–7 This means the majority of PCNS DLBCL most closely resemble a post-germinal center or an activated B-cell (ABC) immunophenotype (CD10–, BCL-6+, MUM1/IRF4+). BCL-6, CD10, BCL-2, MUM1/IRF4 and ki-67 may have prognostic importance. For example, BCL-6 expression was associated with inferior survival outcomes in a recent study of B-cell differentiation markers and their prognostic impact in a cohort of 119 patients from a prospective trial (G-PCNSL-SG1). 8 The incidence of Epstein Barr virus (EBV) infection is high in immunocompromised hosts, such as in patients with acquired immunodeficiency syndrome; in contrast, virtually all tumor samples from immunocompetent hosts are EBV negative. 9 Copy number alterations of 9p24.1 and infrequent translocations of 9p24.1 are also observed in PCNSL, leading to overexpression of the programmed cell death 1 receptor (PD-1) ligands, PD-L1 and PD-L2. 10 Inactivation of CDKN2A is also commonly observed in PCNSL and systemic DLBCL. 11 PCNS DLBCL more often have loss of human leukocyte antigen (HLA) class I or HLA class II expression compared with primary nodal DLBCL. This could result in the evasion of neoplastic B cells from immune surveillance by T cells which, in turn, may explain the poorer prognosis of PCNS DLBCL. 6 The extent of somatic hypermutation of proto-oncogenes has also been shown to be greater in PCNS DLBCL compared with DLBCL arising outside the central nervous system (CNS). 12 In a genomic analysis of 19 PCNSL samples from immunocompetent patients, recurrent abnormalities in PRKCD and TOX genes were observed. 13 PRKCD, a proapoptotic protein kinase, has been implicated in cellular processes such as growth, differentiation, secretion, apoptosis and tumor development. TOX plays a key role in T-cell development and has some effect on B-cell development as well. Mutations leading to activation of the nuclear factor κB (NF-κB) signaling pathway, such as activating mutations of MYD88, CARD11 and CD79 and deletions of TNFAIP3 and TBL1XR1, are observed in almost all PCNSL cases, suggesting that NF-κB activation may play a role in the pathogenesis of PCNS DLBCL and may represent a potential therapeutic target.11,13,14 Gene expression profiles also demonstrate that PCNSL is characterized by differential expression of genes related to adhesion and extracellular matrix pathways, including MUM1, CXCL13 and CHI3L1. Alterations in TP53, CDKN2A/p16, BCL-6, MYC and PAX5 genes are also commonly observed in PCNSL. 14
Diagnostic evaluation
The most common clinical presentation of patients with PCNSL is with nonspecific neurocognitive deficits, and less frequently focal neurological signs or symptoms. The International PCNSL Collaborative Group (IPCG) has developed guidelines to determine the extent of disease in this patient population. 15 Most immunocompetent patients with PCNSL present with a single brain mass. Multiple brain masses are only reported in 20–40% of immunocompetent patients. Supratentorial and periventricular location is common in PCNSL (Figure 1). 16 Due to its hypercellularity, lesions are mainly iso- or hyperdense on unenhanced computed tomography (CT) scan. 16 Magnetic resonance imaging (MRI) with gadolinium contrast is the most sensitive imaging modality in the diagnosis of PCNSL. PCNSL is characterized by homogenous contrast enhancement with well defined borders 17 (Figure 1). Nonenhanced lesions are rare. Perilesional vasogenic edema is common. Low signal on T2-weighted MRI and restricted diffusion on diffusion-weighted imaging (DWI) are other characteristics of PCNSL, which may be explained by its high cellularity with tightly compacted cells and the high nuclear to cytoplasmic ratio. 18 These radiographic features may help to differentiate PCNSL from other conditions, such as infections, tumefactive demyelinating lesions or gliomas. 19 Radiographic response to corticosteroids is common, but this does not secure the diagnosis of PCNSL as inflammatory or demyelinating conditions do so as well. Rarely, PCNSL may present with subtle focal abnormalities of cranial or radicular nerves or focal meningeal enhancement.
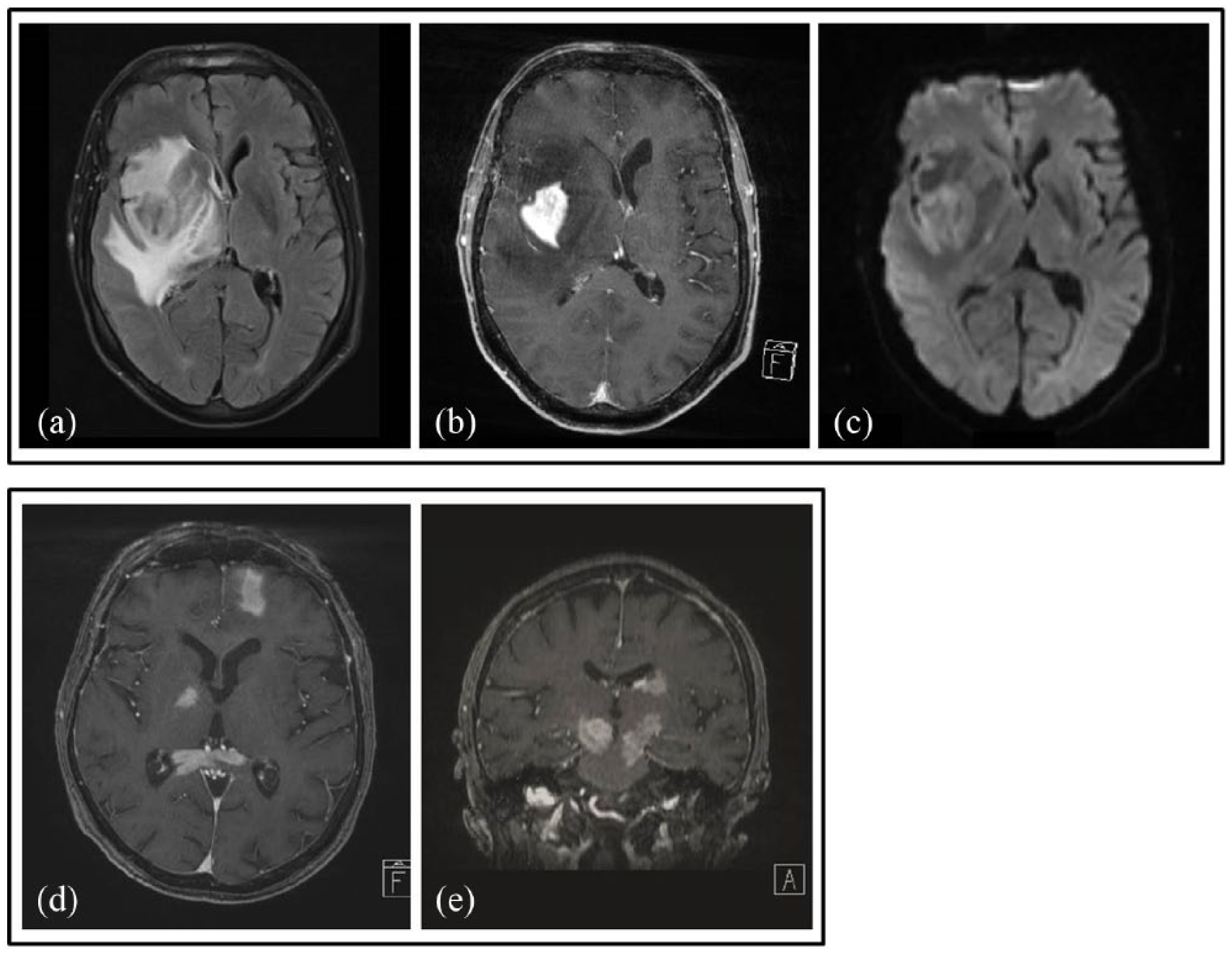
Brain magnetic resonance imaging (MRI) of two patients (a–c, d and e) with primary central nervous system lymphoma (PCNSL): (a) axial fluid-attenuated inversion recovery (FLAIR) sequence demonstrating a hypointense lesion surrounded by hyperintense edema; (b) axial, T1-weighted, contrast-enhanced sequence with intense homogeneous contrast enhancement; (c) diffusion-weighted axial sequence showing bright signal in the lesion, indicating restricted diffusion. (d, e) Axial and coronal T1-weighted, contrast-enhanced sequences revealing multifocal contrast-enhanced PCNSL lesions. (Courtesy of Martin Bendszus, M.D., Division of Neuroradiology, University of Heidelberg.)
Recent studies of advanced imaging techniques have demonstrated the usefulness of these metrics in diagnosis and prognostication of PCNSL. 18 For example, fractional anisotropy (FA) of diffusion tensor imaging (DTI) correlates with microstructural integrity of myelinated fiber tracts and it is significantly lower in PCNSL compared with Glioblastoma (GBM). 20 Similarly, on magnetic resonance spectroscopy PCNSL differs from other glial tumors, including GBM, by massively increased lipid resonances and markedly higher choline/creatine and choline/N-acetyl-aspartate ratios. 21 These imaging techniques, therefore, could facilitate differentiating PCNSL from other brain pathologies. DWI-derived apparent diffusion coefficient (ADC) measurements inversely correlate with PCNSL tumor cellular density and it has been shown that low pretherapeutic ADC values may be predictive of earlier disease progression and shorter overall survival (OS) in patients with PCNSL compared with higher ADC values despite the same chemotherapy treatment. 22 Metabolic imaging by 18 F-fluorodeoxyglucose (FDG) or 11C-methionine positron emission tomography (PET) has been suggested to be able to predict therapy response at a very early time point and also to detect early disease recurrence during post-treatment surveillance, before changes are seen on MRI.23,24 These newer imaging techniques may ultimately provide noninvasive imaging biomarkers that might identify high-risk patients with PCNSL for poor outcome, and may facilitate individualized treatment plans in the future.
Concurrent involvement by DLBCL of the cerebrospinal fluid (CSF) and the eye occurs in approximately 15–20% and 5–20%, respectively. Isolated involvement of the CSF, primary leptomeningeal lymphoma, or isolated involvement of the eye, primary vitreoretinal lymphoma, is rare. Presenting symptoms of ocular involvement include eye pain, blurred vision and floaters. 25 If not contraindicated, a lumbar puncture should be performed for CSF analysis. If biopsy of the brain lesion is not possible, a diagnostic vitrectomy can be performed if ocular involvement is suspected on a split-lamp examination. CSF and vitreous specimens should be assessed by flow cytometry, cytology and immunoglobulin heavy-chain gene rearrangement. CSF cytology is positive in approximately 18% of newly diagnosed PCNSL cases; 26 flow cytometry appears to be more sensitive than cytology in hematologic malignancies of the CNS. 27 Nevertheless, prompt stereotactic biopsy is advised in almost all PCNSL cases that are surgically accessible in the brain, given the possible delay in diagnosis and treatment with the two methods mentioned above. If possible, corticosteroids should be avoided prior to biopsy as histopathological diagnosis can be difficult because of their lymphotoxic effects. However, preoperative treatment with corticosteroids did not prevent the diagnosis of PCNSL by stereotactic biopsy in one study. 28 If corticosteroids have been administered prior to surgery, a new brain MRI should be performed shortly before biopsy to assess the residual lesion.
‘B symptoms’ such as weight loss, fevers and night sweats are rare in PCNSL. For the diagnosis of primary CNS lymphoma, the exclusion of extraneural disease by additional diagnostic testing is required. Evidence of systemic disease has been reported in up to 8% of patients initially thought to have PCNSL. 15 Staging FDG body PET/CT may be more sensitive than a conventional CT of the chest, abdomen and pelvis for detecting systemic disease, as illustrated by a retrospective study in which 7% of patients were found to have systemic NHL by FDG-PET imaging when staging CT scan and bone marrow biopsies were negative. 29 Bone marrow biopsy and aspirate can also reveal subclinical systemic, sometimes lower-grade, lymphoma not detectable by other staging procedures. 30 Approximately 3% of patients with testicular lymphoma have brain metastases at diagnosis mimicking PCNSL and body CT or PET scans may rarely miss an abnormality in the testis, therefore testicular ultrasound for men should be considered.29,31 Blood tests including serum lactate dehydrogenase (LDH), hepatitis and human immunodeficiency virus serologies should be performed. 15
Prognostic models
For PCNSL, two prognostic scoring models have been established.32,33 The Memorial Sloan-Kettering Cancer Center prognostic model described three groups based on age and Karnofsky performance status (KPS). Patients less than 50 years old had the best prognosis with a median survival of 8.5 years, and were classified as group 1. In group 2 (patients ⩾50 years and KPS ⩾ 70), median survival was reduced to 3.2 years. Patients at least 50 years old with a KPS less than 70 had the worst prognosis with a median survival of 1.1 years. 32 The International Extranodal Lymphoma Study Group (IELSG) described five prognostic variables as independent predictors of poor prognosis with low OS: Eastern Cooperative Oncology Group performance status higher than 1; age over 60 years; elevated serum LDH level; elevated CSF protein concentration; and involvement of deep regions of the brain. The 2-year survival with 0–1, 2–3 or 4–5 of these unfavorable factors was 80%, 48% and 15%, respectively. 33 In recent data, patients with lymphopenia at diagnosis of PCNSL (absolute lymphocyte count ⩽ 875 × 106/liter) had a significantly lower 5-year survival rate than that of patients without lymphopenia (22.3% versus 58.5%). This study suggests that lymphopenia is a significant prognostic factor for progression-free survival (PFS) and poor OS. 34 Further validation of these data is needed.
Neurotoxicity
Long-term survival for patients with PCNSL is improving and, thus, the potential for late complications such as treatment-related neurotoxicity is increased and requires significant attention. The exact incidence of delayed neurotoxicity remains unclear, as most studies have not systemically assessed neurocognitive function with serial neuropsychological test batteries. The application of whole-brain radiotherapy (WBRT) alone or in combination with systemic chemotherapy has been identified as a significant risk factor for developing late neurotoxicity, with patients over 60 years old at highest risk. In patients receiving early WBRT after a high-dose methotrexate (HD-MTX)-based chemotherapy regimen, global cognition as determined by the Mini-Mental Status Examination (MMSE) in year 2 after randomization was worse compared with no early WBRT. 35 As the MMSE is insensitive for certain neurocognitive domains, the IPCG has developed an instrument for monitoring neurocognitive function. This assessment is composed of quality of life questionnaires and a focused neuropsychological test battery, including assessment of executive function, attention, memory and psychomotor speed. 36 Treatment-induced leukoencephalopathy with periventricular white matter changes, ventricular enlargement and cortical atrophy are frequent radiographic findings. Demyelination, hippocampal neuronal loss and large-vessel atherosclerosis are common features in pathological studies. 37 The pathophysiology is unknown but is likely multifactorial. Damage to neural progenitor cells has been implicated to play an important role in radiation-related neurotoxicity. 38
Treatment
Response assessment
The IPCG has established response criteria that assess all involved sites (brain, CSF and eye) and corticosteroid dosage. Gadolinium-enhanced MRI scans are the standard for assessing tumor lesions in the brain or spinal cord. CSF and ophthalmological evaluation is needed when the leptomeninges and eye, respectively, are involved at diagnosis or as clinically indicated. 15 Lumbar punctures should only be performed in patients at no risk of brain herniation. Responses are defined by the IPCG criteria as indicated in Table 1.
Response assessment of PCNSL from the International PCNSL Collaborative Group.

CR, complete response; CRu, unconfirmed complete response; CSF, cerebrospinal fluid; PCNSL, primary central nervous system lymphoma; PD, progressive disease; PR, partial response; RPE, retinal pigment epithelium; SD, stable disease.
Corticosteroids
Corticosteroids lead to decreased tumor-associated edema and may result in partial radiographic regression (PR) due to their lymphotoxic effects. An initial response to corticosteroids appears to be a prognostic factor in PCNSL with favorable outcome. 39 After an initial response to corticosteroids, most patients quickly have relapsing disease. As already described, corticosteroids should generally be avoided preoperatively due to the risk of a nondiagnostic biopsy.
Surgery
Surgical resection is not considered the standard of care in treating PCNSL given the multifocal nature of this tumor. 40 There might be a small percentage of patients with large lesions and acute symptoms and signs of brain herniation who will benefit from tumor debulking. To date, however, the extent of resection has not been established as a prognostic factor in PCNSL. Although in one report a possible benefit of gross total resection in patients with PCNSL was observed, this was a retrospective, subset analysis likely confounded by selection bias. 13 Other reports demonstrate no clear benefit. In patients with uncharacteristic MRI lesions, frozen section analysis is a useful tool in brain tumor surgery to determine whether further resection would be beneficial (e.g. in a glioma). Today, diagnosis of PCNSL via stereotactic biopsy of the intracranial mass is the most accepted diagnostic procedure in PCNSL.
Radiotherapy
Optimal standard treatment for PCNSL has not been established. As PCNSL is a microscopically diffuse, multifocal disease, focal radiation or radiosurgery is not recommended. Historically, WBRT at doses ranging from 36 to 45 Gy was performed as first-line therapy, resulting in a high proportion of radiographic responses, but early relapse was typical. In a multicenter, phase II trial conducted by the Radiation Therapy Oncology Group (RTOG), 41 patients were treated with WBRT (40 Gy) plus a tumor boost of 20 Gy, achieving a median OS of 12 months. 41 Given the lack of durable responses to WBRT and the increased risk of neurotoxicity with this modality of therapy, WBRT is no longer a routinely recommended treatment for patients with newly diagnosed PCNSL. However, WBRT might be an option in patients with contraindications to chemotherapy and as a salvage therapy for patients with refractory or relapsed disease. In a series of 48 patients with refractory or relapsed PCNSL, 58% achieved a complete response (CR) after WBRT, with a survival of 28 months compared with 4–5 months for patients with a partial response (PR) or less. However, 29% developed neurotoxicity after WBRT, with a considerable decline of functional status as measured by the KPS. 42
Chemotherapy for newly diagnosed PCNSL
HD-MTX (3–8 mg/m2) in combination with other chemotherapeutic agents or WBRT is the most effective treatment for newly diagnosed PCNSL. However, there is no consensus on the optimal dose or on the role of WBRT in combination with MTX in the management of newly diagnosed PCNSL. Randomized trials have been conducted or are still ongoing to address these issues (Table 2). Doses of MTX of at least 3 mg/m2 achieve sufficient therapeutic concentrations in the brain parenchyma and CSF, and when combined with WBRT lead to more durable treatment responses.43–45 In a randomized, multicenter, phase II trial in patients with PCNSL less than 75 years old, the effect of adding high-dose cytarabine to induction therapy with HD-MTX versus HD-MTX alone was assessed. All patients underwent consolidative WBRT after induction therapy. Radiation dose was chosen according to response and age after chemotherapy: patients in CR and up to 60 years old received 36 Gy; for patients over 60 years old and in CR radiation was chosen at the discretion of the participating center. Patients in PR received 36 Gy plus a boost of the tumor bed of 9 Gy; patients with stable disease (SD) or progressive disease (PD) were irradiated with 40 Gy plus a boost of 9 Gy. Forty-six percent of patients receiving HD-MTX plus cytarabine achieved a CR compared with 18% in the HD-MTX arm. 46 Moreover, the patients treated with the combination had a superior 3-year OS. However, the incidence of neurotoxicity with combined modality treatment that includes standard dose WBRT is significant, especially in elderly patients. 36 Therefore reduced-dose WBRT has been investigated in several trials. Fifty-two patients were enrolled in a multicenter phase II trial assessing the efficacy of reduced-dose consolidation WBRT (23.4 Gy) plus cytarabine in patients achieving CR to induction chemotherapy with rituximab, HD-MTX, procarbazine and vincristine (R-MPV). There was no significant decline of neurocognitive function observed at early follow up. 47 Due to the delayed risk of neurotoxicity, 48 longer neuropsychological evaluation of these patients is necessary to definitively assess the safety of this regimen. In several phase II studies, the safety, efficacy and modest neurotoxicity of HD-MTX chemotherapy (every 10–21 days with doses ⩾3 g/m2) could be demonstrated.49,50 Longer duration of induction chemotherapy with HD-MTX results in higher CR rates. In the IELSG32 randomized trial, the MATRix induction regimen (arm C: MTX + cytarabine + thiotepa and rituximab) in patients with PCNSL and aged up to 70 years provided superiority in terms of CR and overall response rates compared with arm A (MTX + cytarabine) and arm B (MTX + cytarabine + rituximab). At a median follow up of 30 months, patients in arm C had a CR rate of 49% compared with 23% in arm A and 30% in arm B. There was no difference in infectious complications in the three groups. 51 In a multicenter, phase II trial of induction MTX, temozolomide and rituximab (MTR), all drugs with demonstrated single-agent efficacy in PCNSL, followed by a consolidative etoposide/cytarabine combination without WBRT, the CR rate after induction therapy was 66% and the median PFS was 29 months. 49 Median OS was not reached with a median follow up of 5 years. These results are comparable to those seen with consolidative WBRT. An ongoing randomized phase II trial, RTOG 1114, is comparing R-MPV with or without reduced-dose WBRT (23.4 Gy), followed by cytarabine [ClinicalTrials.gov identifier: NCT01399372].
Overview of trials in primary central nervous system lymphoma.

DA-TEDDI-R, dose-adjusted temozolomide, etoposide, doxil, dexamethasone, ibrutinib, rituximab; HD-MTX, high-dose methotrexate; HDT/ASCT, high-dose therapy/autologous stem cell transplantation; MTX, methotrexate; WBRT, whole-brain radiotherapy; BCNU, Bis-chlorethylnitrosourea; R-MBVP, rituximab, MTX, BCNU, teniposide, prednisolone.
An ongoing randomized trial is also investigating the role of induction rituximab in newly diagnosed PCNS DLBCL randomized to rituximab, MTX, teniposide, Bis-chlorethylnitrosourea (BCNU), prednisolone rituximab, MTX, BCNU, teniposide, prednisolone (R-MBVP) or MBVP alone. 58
Intrathecal chemotherapy
Several nonrandomized studies have investigated combination chemotherapies, including intrathecal MTX. However, there was no improvement of outcome in regimens incorporating intrathecal chemotherapy versus those that did not.59,60 Thus, intrathecal chemotherapy with MTX is not currently considered a part of standard induction chemotherapy for patients with newly diagnosed PCNSL. However, this question should be addressed in a future randomized trial.
Rituximab
Rituximab is a chimeric monoclonal antibody targeting the CD20 antigen. It is incorporated into various treatment regimens at doses of 375–800 mg/m2. CSF penetration is low, with CSF levels from 0.1% to 4.4% of serum levels. However, radiographic responses haven been observed in patients with relapsed PCNSL treated with rituximab monotherapy. 61 CR rates are higher in induction regimens that include rituximab compared with chemotherapy regimens without rituximab. 62 As noted above, a randomized trial addressing the utility of induction rituximab is ongoing. Intrathecal administration of rituximab alone or in combination with systemic chemotherapy is well tolerated and should be investigated in future trials of patients with PCNSL and leptomeningeal involvement.63,64
Consolidation therapy
The optimal consolidative chemotherapy for PCNSL is not yet defined. As noted, WBRT has a risk of neurotoxicity and several trials have assessed whether WBRT can be eliminated in the treatment of patients with newly diagnosed PCNSL. In a multicenter, phase III trial, HD-MTX-based chemotherapy with or without consolidative WBRT was investigated. Patients randomized to chemotherapy plus WBRT achieved longer PFS but no improvement in OS compared with those treated with chemotherapy alone (32.4 months versus 37.1 months). 52 As noted previously, there are also initiatives to reduce the dose of consolidative WBRT in an effort to reduce the risk of neurotoxicity. 47 Other studies have investigated chemotherapy without WBRT as induction and consolidation for newly diagnosed PCNSL. In a multicenter phase II trial, dose-intensive consolidation chemotherapy with etoposide and cytarabine was administered to patients who achieved CR with induction chemotherapy using HD-MTX, rituximab and temozolomide (CR rate was 66%). The median PFS of 2.4 years observed in this study without WBRT was comparable to those regimens that included WBRT. 49
Another consolidative approach omitting WBRT is high-dose chemotherapy followed by autologous stem cell transplantation (HDT/ASCT). This involves leukapheresis and peripheral blood stem cell harvest, followed by conditioning chemotherapy then reinfusion of the stem cells to restore blood cell production. Currently, there is no consensus on the optimal conditioning regimen. However, regimens that contain CNS-penetrant agents such as carmustine, thiotepa and busulfan have demonstrated the most encouraging results. Promising 2-year OS rates were reported in two phase II trials utilizing this approach. In a multicenter phase II study, patients were treated with MATRix induction chemotherapy, followed by high-dose carmustine and thiotepa conditioning with ASCT. 65 The objective response rate was 91% and 2-year OS was 87%. The treatment-related mortality rate was less than 10%. In another phase II study, patients who responded to the induction R-MPV regimen were treated with consolidative high-dose chemotherapy consisting of thiotepa, busulfan and cyclophosphamide (TBC) followed by ASCT. 66 Two-year PFS and OS were almost identical at 79% and 81%, respectively, indicating that nearly all patients alive at 2 years following treatment were free of disease progression. With a median follow up of 45 months, median PFS and OS were not reached. In this study, however, the treatment-related mortality rate among patients who received transplantation was high at 11.5%. Long-term survival data from another phase II trial showed a durable response, with an OS rate of 35% after 10 years of follow up in patients treated with HD-MTX, then high-dose busulfan and thiotepa followed by ASCT. 67 Moreover, seven of the eight patients who were treated with chemotherapy alone had no neurotoxicity and had excellent quality of life and functional status, with KPS of 90–100%.
The results of the second randomization of the IELSG32 phase II trial, in which patients less than 70 years old were treated with either WBRT or carmustine thiotepa conditioned ASCT after MATRix induction therapy, demonstrated that both treatment regimens were effective and feasible, with no significant differences in 2-year PFS (80% and 69%). Two of 59 patients in the ASCT group died because of infection. 54 Overall, high-dose chemotherapy followed by ASCT appears to be highly effective with less delayed neurotoxicity, therefore it is a promising consolidative approach, especially in younger patients with good performance status. Several ongoing randomized trials are comparing the efficacy of different consolidation approaches: high-dose chemotherapy followed by ASCT versus WBRT [ClinicalTrials.gov identifier: NCT00863460, NCT01011920] or ASCT versus chemotherapy [ClinicalTrials.gov identifier: NCT01511562, NCT02531841] (Table 2).
Chemotherapy in the elderly
In elderly patients (>60 years), who account for more than half of all subjects diagnosed with PCNSL, 1 the risk of neurotoxicity is the highest. The majority of elderly patients develop neurotoxicity after treatment with regimens containing WBRT; some of these patients die of treatment-related complications, rather than refractory or relapsed disease. 36 Doses of MTX from 3 to 8 g/m2 are generally well tolerated in elderly patients, with manageable grade 3 or 4 renal and hematological toxicity. 68 In a meta-analysis of 784 elderly patients with PCNSL, treatment regimens with HD-MTX were associated with improved survival. Survival was also improved with WBRT, but there was an increased risk of neurological side effects. 69 In a multicenter single-arm trial of patients with PCNSL aged 65 years or over were treated with rituximab, HD-MTX and procarbazine; lomustine was omitted during the study due to infectious complications. The CR rate was 35.5%, 2-year PFS rate was 37.3% and treatment-related death occurred in 8.4% of enrolled patients. Tolerability was suboptimal, with 81.3% of patients experiencing at least one grade 3 toxicity. 55 In another multicenter phase II trial, 98 elderly patients with PCNSL were randomized to receive either MTX, procarbazine and vincristine (MPV-A) or MTX and temozolomide (MT) with one additional cycle of cytarabine in the MPV arm only. There were no statistical differences between the two groups with respect to CR, PFS and OS. 53 In a retrospective study of 52 elderly patients treated with high-dose thiotepa based chemotherapy followed by ASCT as first-line (28.8%) or as second- or subsequent-line treatment (71.2%), 69% achieved CR and 9% PR with a 2-year PFS and OS of 62% and 70.8%, respectively. Two treatment-related deaths (3.8%) were observed. 70 In summary, there is no standard of care defined for elderly patients with newly diagnosed PCNSL and further studies are needed. WBRT should be avoided because of the higher risk of clinical neurotoxicity. High-dose chemotherapy followed by ASCT appears to be effective and feasible in selected elderly patients with PCNSL.
Refractory and relapsed PCNSL
Despite high response rates with initial HD-MTX-based treatment, more than half of initial responders relapse. Moreover, about a quarter of patients have disease that fails to respond to the initial treatment. Prognosis of refractory or relapsed PCNSL remains poor. In a retrospective study the median OS from the time of progression (OS2) was 2 months in patients with primary refractory disease and 3.7 months in patients with disease that relapsed within the first year of initial therapy. 71 A better prognosis was observed in patients who received high-dose chemotherapy with ASCT at relapse, however these patients tended to be younger with better performance status and more chemosensitive disease. Moreover, about a quarter of them were asymptomatic at relapse, which may explain the better KPS and better survival in this group. This observation supports the need for regular neuroimaging surveillance after initial treatment.
The optimal treatment for refractory or relapsed PCNSL is poorly defined as there are only a limited number of prospective trials in this setting. The choice of salvage treatment depends on age, previous treatment and response, performance status and comorbidities at the time of relapse. HD-MTX rechallenge is an effective approach in patients who had previously achieved a prolonged response to this agent. This approach is supported by retrospective studies which have reported response rates of 85–91% and median OS2 of 41–62 months.72,73 For younger patients with a good performance status who have not previously been treated with high-dose chemotherapy and ASCT, this is also an option at the time of relapse. In a phase II trial of high-dose etoposide and cytarabine followed by high-dose chemotherapy with the TBC regimen and ASCT, 96% of patients with refractory/relapsed PCNSL who proceeded to transplantation achieved a CR. 74 The median PFS and OS in this group was 41.4 months and 58.6 months, respectively. For patients who have not been treated with WBRT as a part of their initial treatment, this modality can be an effective option and is supported by retrospective studies in which response was observed in about 75% of patients.24,49 The median PFS and OS was 10 months and 11–19 months, respectively. These results suggest that the efficacy of deferred WBRT until the time of relapse is comparable to that seen when WBRT is employed as initial therapy. Delayed neurotoxicity of WBRT remains a problem in this approach as it was observed in 15–29% of patients who survived more than 4 months after WBRT.42,75 Age over 60 years and shorter time (<6 months) between the initial HD-MTX-based therapy and the salvage WBRT were associated with increased risk of neurotoxicity. There are reports of some activity with other agents, including temozolomide, topotecan, rituximab, rituximab/temozolomide, bendamustine, ifosfamide/etoposide, and cisplatin/cytarabine, with varying results.
Novel therapeutics
Pemetrexed
Pemetrexed, a folate antimetabolite with a broader spectrum of activity than MTX demonstrated activity in a case series of 17 patients with recurrent PCNSL and an overall radiographic response rate of 58.8% and a median OS of 7.8 months; three patients died of infection. 76 As with MTX, the main side effects include myelosuppression, gastrointestinal reactions and infections; doses up to 900 mg/m2 are relatively well tolerated. 77 In elderly patients, pemetrexed (600 mg/m2) as induction therapy appears to be feasible and well tolerated, with a median OS of 19.5 months in a case series. Patients achieving a CR, PR or SD received maintenance therapy with pemetrexed for a maximum of six cycles. Two patients are still in CR at follow up at 36 and 45 months, respectively. No neurotoxicity or treatment-related deaths were observed in this retrospective study of 12 patients with PCNSL over 65 years old. 78 A combination of pemetrexed (500 mg/m2) with rituximab in patients with recurrent PCNSL after MTX-based first-line treatment shows that the combination is well tolerated, with an overall radiographic response rate of 62.9% and a median OS of 11.2 months. 79
Lenalidomide
Lenalidomide, an oral immunomodulatory agent and derivate of thalidomide with antiproliferative properties, is the subject of several trials in the PCNSL patient population. In one case series, two of six patients with relapsed PCNSL treated with lenalidomide as salvage therapy achieved a CR, with duration of more than 24 months in one patient. 80 In a phase I study of dose-escalating lenalidomide in patients with relapsed or refractory CNS lymphoma, eight of eight evaluable subjects achieved an objective response (four CR, four PR) after 1 month of lenalidomide monotherapy. In a second cohort, 5 of 10 patients with relapsed or refractory CNS lymphoma had a durable response for more than 2 years. Lenalidomide should be further investigated as a potential consolidative or maintenance therapy. 81 In a multicenter phase II trial of relapsed or refractory PCNSL or primary vitreoretinal lymphoma, the combination of rituximab and lenalidomide in an induction phase followed by maintenance therapy with lenalidomide monotherapy was investigated. After the induction phase, 17 of 43 evaluable patients had an objective response rate including 13 CRs. The results for 17 patients who entered the maintenance phase are pending. 56
Ibrutinib
Over 90% of primary CNS DLBCL cases most closely resemble the ABC-like subtype of DLBCL and are highly dependent on B-cell receptor (BCR) signaling. As BCR signaling in these tumors is activated, ibrutinib, a small molecule with promising CNS distribution that binds permanently to the Bruton’s tyrosine kinase, inhibiting B-cell receptor signal transduction, is a promising candidate drug for assessment in PCNSL. In a phase Ib study, 94% of 18 patients with PCNSL had a reduction in tumor size with ibrutinib monotherapy. 57 As patients with ABC DLBCL treated with ibrutinib monotherapy have a median survival of 10.3 months, 82 a combination regimen with dose-adjusted (DA)-TEDDI-R (temozolomide, etoposide, liposomal doxorubicin, dexamethasone, ibrutinib and rituximab) was assessed. DA-TEDDI-R was designed around therapeutic principles for systemic DLBCL and CNS penetration. Due to a potential antagonism with MTX, ibrutinib and MTX combinations are avoided; therefore, MTX was excluded from this regimen. 83 A total of 86% of 14 evaluable patients receiving ibrutinib and DA-TEDDI-R achieved CR, one PR and one PD. Five patients died during the treatment, two secondary to pulmonary/CNS aspergillosis, one of neutropenic sepsis, one patient with ventricular arrhythmia and one with ischemic stroke; three patients died from tumor progression. As in patients with systemic ABC DLBCL, mutations in the BCR subunit CD97B were associated with partial or incomplete response to ibrutinib monotherapy.57,82 Additionally, activating CARD11 mutations leading to activation of the NF-κB signaling pathway were observed in ibrutinib-resistant systemic ABC DLBCL and in one patient with PCNSL.82,84 In a retrospective case study, 14 patients with relapsed or refractory PCNSL were treated with ibrutinib monotherapy. CR was observed in three patients, PR in four patients, and the median PFS was 6 months. 85 Further evaluation of this agent in PCNSL with special attention to Aspergillus infection is needed. Some data suggest that this may be an ‘on target’ effect of this class of agents. A phase I/II study [ClinicalTrials.gov identifier: NCT02315326] is currently recruiting patients with primary or secondary CNS lymphoma investigating the maximum tolerated dose and toxicity of ibrutinib alone and in combination with HD-MTX. Because of drug–drug interactions, both agents will not be administered concurrently. 86
Nivolumab
The monoclonal antibody nivolumab blocks PD-1, thereby preventing T cells from being inactivated. As noted previously, the PD-1 ligands, PD-L1 and PD-L2, are overexpressed in PCNSL, leading to reduced T-cell proliferation and survival. 10 Five heavily pretreated patients with relapsed or refractory PCNSL or primary testicular lymphoma had clinical and radiographic responses to nivolumab treatment and were alive at a median follow up of 17 months. One patient received three doses of rituximab after beginning nivolumab treatment; two other patients received WBRT or focal radiation immediately prior to nivolumab. One grade 4 toxicity of renal insufficiency was observed. Based on these encouraging, preliminary data, a multicenter phase II trial of nivolumab in patients with recurrent and refractory PCNSL and primary testicular lymphoma was initiated and is ongoing. 87
Chimeric antigen receptor T-cell therapy
For chimeric antigen receptor (CAR)-T-cell therapy the T cells of a patient are collected by apheresis and genetically engineered to express the CAR specific to the patient’s particular cancer. After expanding the cells in vitro, they are reinjected into the patient after lymphodepleting chemotherapy. Various trials are ongoing focusing on CAR-T-cell therapy in hematological malignancies. A 68-year old female patient with DLBCL and cerebral involvement refractory to several chemotherapy regimens including an allogenic stem-cell transplantation was enrolled in the TRANSCEND-NHL-001 phase I trial [ClinicalTrials.gov identifier: NCT02631044] and demonstrated activity of the CAR-T-cell therapy in the CNS. The patient received chemotherapy with fludarabine cyclophosphamide, followed by the CD19-directed CAR-T-cell product JCAR017 resulting in CR at 1-month follow up (PET/CT and brain MRI). A subcutaneous lesion at 2-month follow up was resected without further treatment; CR was confirmed at 3 months of follow up with ongoing remission at 12 months. No neurotoxicity, graft versus host disease or cytokine release syndrome were observed. 88 Further evaluation of this new treatment approach in PCNSL is warranted.
Temsirolimus
Mammalian target of rapamycin (mTOR) signaling is often dysregulated in PCNSL and inhibition of the pathway may also effectively reduce PCNSL progression. Temsirolimus, an inhibitor of mTOR, achieved high radiographic response of 54% in a phase II study of 37 patients with relapsed or refractory PCNSL, but median PFS was low (2.1 months). 89 Further validation of this agent is needed.
Monitoring and follow up
The majority of recurrences occur within the CNS and within the first 5 years of treatment completion. However, continued follow up to 10 years is recommended as there are late recurrences. The IPCG’s recommendations for follow-up assessments and monitoring are outlined in Tables 1 and 3. 15
Follow-up schedule of PCNSL from the International PCNSL Collaborative Group.

CSF, cerebrospinal fluid; CT, computed tomography; IPCG, International PCNSL Collaborative Group; MMSE, Mini Mental State Examination; MRI, magnetic resonance imaging; PCNSL, primary central nervous system lymphoma.
Conclusion
Treatment for PCNSL has advanced significantly with improved survival for this rare and aggressive lymphoma of the CNS, however relapse is common and long-term survival remains poor. While the optimal treatment approach has yet to be established, high-dose methotrexate-based chemotherapy is currently considered as the standard induction treatment for newly diagnosed PCNSL. Ongoing randomized trials are evaluating different consolidative approaches using high-dose chemotherapy with ASCT, reduced-dose WBRT or chemotherapy. Treatment of relapsed or refractory PCNSL and elderly patients with PCNSL remain challenging. With better understanding of the molecular pathogenesis of PCNSL, personalized treatments that incorporate targeted agents, hold significant promise.