
Abstract
Background
The cause and clinical significance of the transient decrease in platelet (PLT) count observed in relapsing remitting multiple sclerosis (RRMS) during alemtuzumab administration remain undefined. The aim of this study was to analyse the kinetics and clinical relevance of early onset thrombocytopaenia in alemtuzumab-treated RRMS.
Methods
A total of 26 patients with RRMS were included in a longitudinal study. Blood samples were collected immediately before the first alemtuzumab infusion (D0), and after 3 days (D3), 28 days (D28) and 49 days (D49). PLT, red blood cell (RC), leucocyte and lymphocyte counts, haemoglobin (Hb) concentration and haematocrit (Htc) were measured. Patients with MS were clinically evaluated every day of drug infusion and then at D28 and D49 to verify the presence of signs or symptoms suggestive of thrombocytopaenia.
Results
PLT number significantly decreased at D3 (p < 0.005) and was associated with a decrease in RC count (r: 0.53, p < 0.01), Hb (r: 0.42, p = 0.05) and Htc (r: 0.53, p < 0.01). A progressive reversion of PLT number to normal values was observed at D28 and D49. A mild thrombocytopaenia was observed in 12 patients (46.2%), 8 of which (66.6%) had PLT nadir values at D3, and 4 (33.3%) at D28. No sign or symptom suggestive of thrombocytopaenia was observed. A strong correlation between pretreatment and nadir PTL counts (r: 0.59, p < 0.005) was observed; indeed, mild thrombocytopaenia was observed more frequently in these patients with a baseline PTL count lower than 230 × 109/L (83.3% versus 42.9%, p < 0.05).
Conclusions
The early PLT decrease in alemtuzumab-treated patients is transient, mild, not associated with clinically relevant events and is probably related to the cytokine-released syndrome. Notwithstanding this, our findings suggest the opportunity for PLT monitoring during infusion and in the following 2 months, since a decrease in PLT count may occur.
Introduction
Alemtuzumab, an anti-CD52 monoclonal antibody approved for the treatment of relapsing remitting multiple sclerosis (RRMS), induces a rapid and long-lasting depletion of circulating T cells and B cells. The dynamics of lymphocyte repopulation, which are specific for each lymphocyte subset, may explain both the long-term efficacy and safety profile of alemtuzumab.1,2 Indeed, the CD4+ T helper cell and the regulatory T cell (Treg) subsets show a rapid and almost complete depletion followed by a slow repopulation that follows different kinetics and reaches the lower normal limit in a median time of 35 months.3,4 After therapy, a significant increase in Treg percentage on the CD4+ subset (from 3.4% to 13.7% in CARE MS I 3 and from 3.8% to 12.5% in CARE MS II 4 ) was observed at the end of the first month. It is currently believed that the long-lasting T helper-cell depletion and the early reconstitution of Treg may account for the long-term efficacy of alemtuzumab. 2
On the other hand, the increase in immature B cells (CD19+, CD27-IgD+, CD10+, CD38+) during the first months (approximately +180% at month 3 compared with baseline)3,4 explains the rapid B cell repopulation that reaches baseline values between month 3 and month 6 after therapy. Since B cell-mediated autoimmune disorders (i.e. thyroiditis, 5 thrombocytopaenia 6 and, more rarely, nephropathy 7 ) can be observed in alemtuzumab-treated patients, it has been hypothesized that T cell depletion facilitates the survival of autoreactive naïve B cells. 2 However, it has to be pointed out that antibody-mediated disorders appear later (namely, after 12–18 months) when the reconstituted T helper-cell repertoire may support an ongoing germinal centre reaction.2,8
Recently, two reports have described the appearance of an early and transient thrombocytopaenia during alemtuzumab infusion in 2/22 patients (9.1%) 9 and 34/48 patients (70.8%). 10 Although platelet (PLT) count reverted to basal values during the first month in the majority of patients, three patients (6.5%) 10 presented a delayed PLT count restoration (within 150 days). No evidence of idiopathic thrombocytopaenic purpura or severe adverse event was reported in both studies, thus supporting the hypothesis of an infusion-related phenomenon rather than an autoimmune mechanism.
The pathogenesis and clinical relevance of this potentially harmful phenomenon are still undefined. Here, we report an early time-course analysis of PLT number in alemtuzumab-treated patients with RRMS and show that this adverse event is common, rapidly reverts to normality and is not associated with clinical signs or symptoms.
Materials and methods
Study population
All patients treated with the first course of alemtuzumab in our Multiple Sclerosis Centre, following the approval of the drug by the Italian Agency for Medicines, and having concluded the first 2 months of clinical and laboratory follow up, were consecutively included in the study. Besides the administration of alemtuzumab at the standard dose of 12 mg intravenously diluted with 100 ml of saline solution (infusion speed: 20 ml/h) for 5 consecutive days, the therapeutic protocol included the daily administration of ranitidine 300 mg by mouth, intravenous injection of chlorphenamine maleate 10 mg diluted with 100 ml of saline solution (administrated in 15 min), acyclovir 200 mg by mouth, intra-articular injection methylprednisolone 1 g intravenously diluted with 500 of saline solution (administrated in 60 min), acetaminophen 1 g by mouth, and ondansetron 8 mg intravenously diluted with 100 ml of saline solution (administrated in 15 min). Among these drugs, only methylprednisolone affects the PTL count, usually determining an increase in number.
Prior to the first infusion of alemtuzumab (day 0 [D0]) and after 3 days (D3), 28 days (D28) and 49 days (D49), PLT and red blood cell (RC) counts, haemoglobin (Hb) concentration, haematocrit (Htc), leucocyte and lymphocyte counts were analysed. In order to verify the appearance of any symptoms or signs suggestive of thrombocytopaenia, patients with MS were examined weekly in the first 2 months and then monthly. The study was approved by notification to the Local Ethic Committee (Comitato Etico per la Sperimentazione Clinica, Azienda Ospedaliera, Università degli Studi di Padova; prot. N. 0050576) and all the patients gave their informed consent.
Statistical analysis
Paired t-test or chi-square test were applied in the analysis to compare haematological findings between the time-points, while linear correlation between variables was tested using the Pearson’s single or multiple linear model (all variables were normally distributed). The significance level was set at p < 0.05.
Results
Demography and clinical findings
Enrolment for the study started on February 2015. Of the 26 patients with RRMS enrolled in the study, 16 were women and 10 were men. At alemtuzumab infusion, mean age was 31.7 ± 8.1 (range: 19.0–50.0) years, mean disease duration was 6.8 ± 6.9 years (range: 0.0–26.0), and mean Expanded Disability Status Scale was 2.6 ± 1.4 (range: 1.0–6.0). Seven patients (26.9%) were treatment naïve, while the last treatment was with natalizumab in nine patients, dimethyl-fumarate in three patients, fingolimod in four patients, cyclophosphamide in two patients and teriflunomide in one patient. Of these patients, 13 (50%) had been treated with more than three disease-modifying therapies prior to alemtuzumab. No patient reported a previous history of other autoimmune disorders or other haematological diseases. In addition, no medical history of thrombocytopaenia or other PTL disorders had been documented or could be clinically suspected before alemtuzumab infusion.
Haematological changings during alemtuzumab infusion
At D0, mean PLT number was 229,455 ± 56,801 × 109/L (normal value range: 150,000–450,000). At D3, PLT number and percentage significantly decreased in 22/26 (84.6%) patients (mean ± standard deviation: −50,727 ± 47,780 × 109/L and −20.0 ± 21.1%, respectively; D3 versus D0: p < 0.0005 for both comparisons) (Figure 1a). In 8/26 patients (30.8%) the thrombocytopaenia was mild (PLT 100.000–150.00 × 109/L).

Compared with baseline (D0), platelet (PLT) count (a), red blood cell (RC) count (b), haemoglobin (Hb) concentration (c) and haematocrit (Htc) (d) values significantly decreased (all p < 0.0005) during alemtuzumab infusion (D3). The absolute decrease in PLT count observed at D3 strongly correlated with RC count (e). PLT number increased at D28 and returned to baseline values at D49 (f). PLT count at nadir strongly correlated with PLT count at baseline (r: 0.59, p < 0.005) (g). Median values and 25–75 interquartile ranges are shown in (a), (b), (c), (d) and (g). In (e) and (f), 95% confidence interval is indicated.
A significant decrease in RC count (mean ± standard deviation [SD]: −4,35 × 1012/L and −7.1 ± 5.3%, p < 0.0005 for both comparisons) (Figure 1b), Hb (mean ± SD: −126 ± 11 g/L and −7.1 ± 5.6%, p < 0.0005 for both comparisons) (Figure 1c), and Htc (mean ± SD: −0.036 ± 0,020 and −8.8 ± 4.8%, p < 0.0005 for both comparisons) (Figure 1d) was also found at D3 versus D0. As expected, a marked lymphopaenia was observed at D3 (−2.07 ± 1.3 × 109/L, p < 0.0001).
Leucocyte count increased at D3 as an effect of high-dose steroid infusion (+5.5 ± 4.5 × 109/L, p < 0.001).
Interestingly, the absolute decrease in PLT number correlated with an absolute decrease in RC count (r: 0.53, p < 0.01) (Figure 1e), Hb (r: 0.42, p < 0.05) and Htc (r: 0.53, p < 0.01), but not with leucocyte (r: 0.19, p = 0.36) and lymphocyte (r: −0.06, p = 0.76) decrease. The correlation analysis between percentages further confirmed these correlations (namely, RC and PLT r: 0.44, p < 0.05; Hb and PLT r: 0.38, p = 0.05; Htc and PLT r: 0.46, p < 0.05).
Haematological changes during follow up
On the basis of PTL kinetics, three groups of patients could be identified: (a) 8/26 (30.8%) had a mild thrombocytopaenia at D3 that reverted to normal values at D28 (Figure 2a); (b) 14/26 (53.8%) had a slight reduction in PLT count that remained within the normal range at D3; four of these patients had a further PTL decrease at D28 (two had a mild thrombocytopaenia (Figure 2b); (c) 4/26 (15.4%) had a PTL count stable or increased at D3, but two became mildly thrombocytopaenic at D28 (Figure 2c).
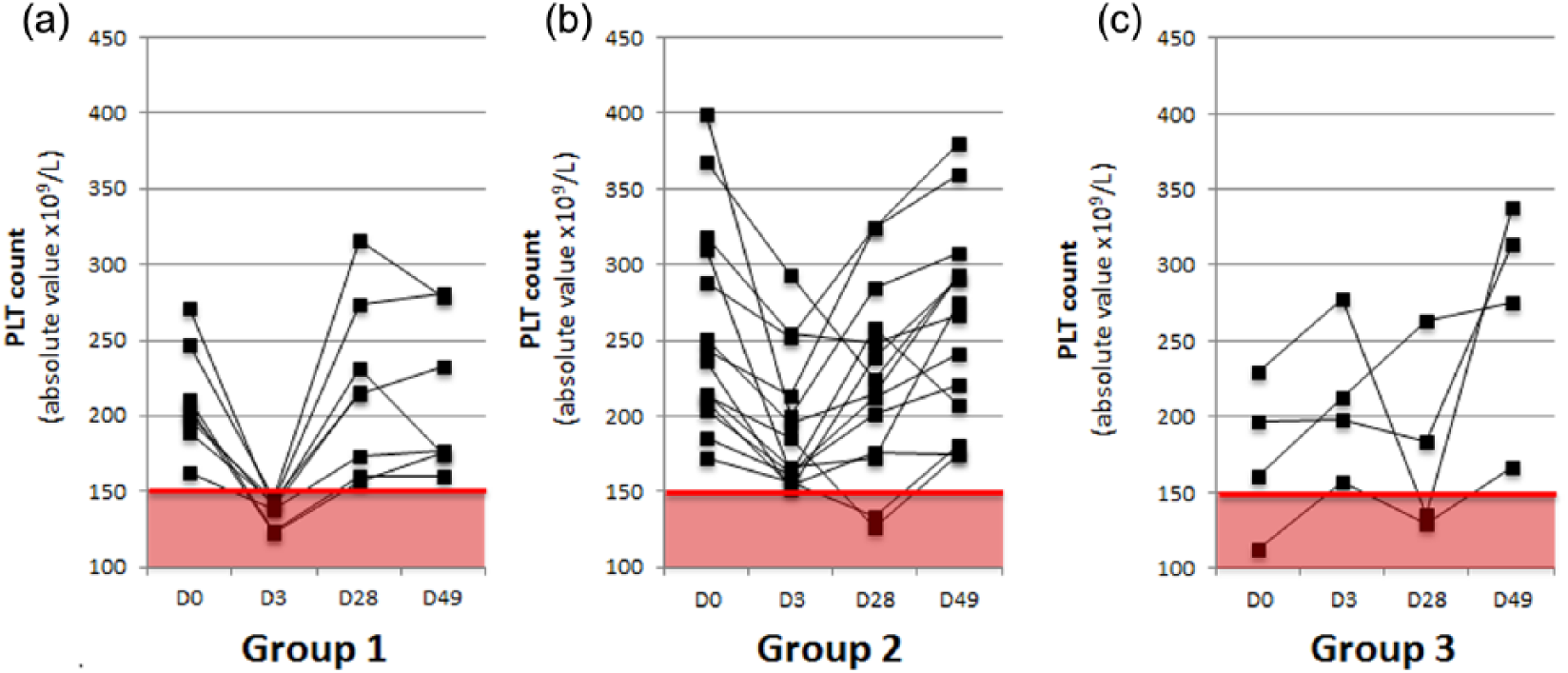
Patients with multiple sclerosis were divided in three groups: (a) group 1, patients with mild thrombocytopaenia at D3 that reverted to normal values at D28 (30.8%); (b) group 2, patients with a slight reduction in platelet (PLT) count that remained within the normal range, at D3 (53.8%); (c) group 3, patients with a PTL count stable or increased at D3 (15.4%). In all patients of group 1, PTL count increased at D28. Two patients in group 2 and two patients in group 3 presented a mild thrombocytopaenia at D28 that reverted within normal values at D48.
In summary, PLT number did not change during follow up in only one patient (3.8%), while 18/26 patients (69.3%) had PLT nadir at D3 and 7/26 (26.9%) at D28. Moreover, 46.2% had a mild thrombocytopaenia during follow up (nadir value at D3 in 30.8% and at D28 in 15.4%). In all cases, PLT count returned within the normal value range at D49 (Figure 1f and Figure 2).
No difference in baseline clinical and haematological variables was observed between groups, but a strong correlation was observed between pretreatment PTL and nadir PTL counts (r: 0.59, p < 0.005) (Figure 1g). Moreover, patients with a baseline PTL count lower than 230 × 109/L more frequently developed mild thrombocytopaenia during follow up (83.3% versus 42.9%, p < 0.05). However, in these patients the increased relative risk, 3.1 (confidence interval 95% 0.9–11.4, p = 0.085) did not reach significance, probably because of the low number of subjects. Finally, no patient developed signs or symptoms suggestive of thrombocytopaenia during the clinical follow up (12.9 ± 7.6 months).
Discussion
Autoimmune thrombocytopaenia, a late adverse event of alemtuzumab therapy, was defined as a PLT count at or below 50,000/μl (without clumping) or between 50,000/μl and 100,000/μl on at least two consecutive measurements, obtained over a 1-month period, associated with normal Hb, neutrophil and eosinophil counts, with no splenomegaly and normal peripheral blood smear (apart from thrombocytopaenia).3,4,11 In all cases, anti-PLT antibodies were demonstrated and antibody-removing therapies (i.e. plasma-exchange or intravenous immunoglobulin) were highly effective.
An early decrease in PLT (during alemtuzumab administration), characterized by a spontaneous restoration of normal PLT count, has also been described during alemtuzumab infusion.9,10
In agreement with these preliminary reports, we found that a significant decrease in PLT count can occur during the first month following alemtuzumab infusion in almost all patients with MS (96.2%), but in 26.9% of patients nadir values were observed at D28. Moreover, a mild thrombocytopaenia was defined in 46.2% patients. An interesting observation of our study is the trend to mild thrombocytopaenia in patients with a PTL count lower than 230 × 109/L at baseline. This finding, which merits investigation in a larger patient series, suggests the possibility of identifying a baseline PTL cut-off value that may help in monitoring and predicting possible PTL-related adverse events.
The rapid onset and spontaneous reversion to normality suggest a drug-induced transient PLT count change, rather than a more complex autoimmune phenomenon. The absence of CD52 on the PLT surface indicates an indirect effect of alemtuzumab.
We observed that PLT decrease was significantly correlated with similar decreases in RC, Hb concentration and Htc. This finding could suggest an increased blood volume following steroid and saline administration (included in the therapeutic protocol). However, since the correlations observed were moderate (explaining less than 30% of PLT decrease) and blood specimens were sampled at 8.00 a.m. (i.e. almost 14 h after previous drug infusion) blood dilution does not explain the phenomenon.
Moreover, the lack of correlation with lymphocyte depletion seems to exclude a complement-mediated alemtuzumab-boosted lysis of circulating PLTs.
We believe that a more likely explanation of PTL decease can be found in the cytokine-release syndrome that peaks 2–6 h after alemtuzumab infusion and continues throughout the infusion course. 12 This syndrome is caused by antibody-mediated cellular cytotoxicity and complement activation that lysate CD52-expressing T and B lymphocytes, with the release of pro-inflammatory cytokines (i.e. tumour necrosis factor alpha [TNF-α], interleukin-6 and interferon-γ) producing a clinical picture characterized by pyrexia, headache, malaise and urticarial rash. 13 Pro-inflammatory cytokines were found to decrease PLT count both directly and indirectly. Indeed, TNF-α was found to (a) induce PLT consumption by acting not on PLT directly, but on the tumour necrosis factor receptor 1 expressed by other cells, presumably increasing the release of factors with agonist activity for PLT 14 , and (b) promote PLT aggregation.15–17
We are aware that a limitation of our study is the relatively low number of patients analysed. However, while confirming previous findings in much lower numbers of patients, the homogeneity of our data suggests that increasing the sample size would further confirm rather than contradict our results.
In summary, we confirmed that the decrease in PLT count observed during alemtuzumab infusion can be demonstrated in almost all patients, being mild in 46.2% of patients and always self-limited. PTL nadir values were not reached during drug infusion, but rather in the following 4 weeks, supporting the importance of performing a haemachrome analysis 1 month after alemtuzumab infusion. Thus, PLT assessment during infusion and monitoring in the following months should be considered good clinical practice in order to prevent a possible unexpected early decrease in PLT count and to detect autoimmune thrombocytopaenia in later therapeutic phases.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.