
Abstract
Multiple sclerosis (MS) is a common and chronic central nervous system (CNS) demyelinating disease and a leading cause of permanent disability. Patients most often present with a relapsing–remitting disease course, typically progressing over time to a phase of relentless advancement in secondary progressive MS (SPMS), for which approved disease-modifying therapies are limited. In this review, we summarize the pathophysiological mechanisms involved in the development of SPMS and the rationale and clinical potential for natalizumab, which is currently approved for the treatment of relapsing forms of MS, to exert beneficial effects in reducing disease progression unrelated to relapses in SPMS. In both forms of MS, active brain-tissue injury is associated with inflammation; but in SPMS, the inflammatory response occurs at least partly behind the blood–brain barrier and is followed by a cascade of events, including persistent microglial activation that may lead to chronic demyelination and neurodegeneration associated with irreversible disability. In patients with relapsing forms of MS, natalizumab therapy is known to significantly reduce intrathecal inflammatory responses which results in reductions in brain lesions and brain atrophy as well as beneficial effects on clinical measures, such as reduced frequency and severity of relapse and reduced accumulation of disability. Natalizumab treatment also reduces levels of cerebrospinal fluid chemokines and other biomarkers of intrathecal inflammation, axonal damage and demyelination, and has demonstrated the ability to reduce innate immune activation and intrathecal immunoglobulin synthesis in patients with MS. The efficacy of natalizumab therapy in SPMS is currently being investigated in a randomized, double-blind, placebo-controlled trial.
Introduction
Multiple sclerosis (MS) is a chronic demyelinating disease of the central nervous system (CNS), affecting an estimated 2.0–2.5 million people worldwide [Milo and Kahana, 2010]. Relapsing–remitting MS (RRMS), the most common form of MS, in which disability accumulates in a stepwise fashion due to incomplete recovery from relapses, typically transitions over time towards a secondary progressive phase, in which relapses become less and less frequent and insidious disability progression begins [Weinshenker, 1998]. Thus, RRMS and secondary progressive MS (SPMS) are generally regarded as different phases of the same disease, each with ‘active’ and ‘not active’ phenotypes that are differentiated by the presence of relapses with or without magnetic resonance imaging (MRI) activity [Lublin et al. 2014]. Despite being on a continuum, RRMS and SPMS appear to have somewhat distinct pathophysiological mechanisms. In RRMS, deterioration results from acute intermittent inflammation, demyelination and axonal injury following the transmigration of inflammatory cells into the CNS [Frischer et al. 2009; Kutzelnigg et al. 2005; Lassmann, 2007a]. Conversely, disability accumulation in SPMS results mostly from chronic persistent demyelination, continued widespread axonal injury, and a compartmentalized inflammatory process behind the blood–brain barrier (BBB) distinguished by chronic meningeal inflammation, ectopic lymphoid tissues and widespread microglial activation that is most notable in the white matter [Frischer et al. 2009; Kutzelnigg et al. 2005]. During the transition from RRMS to SPMS, both peripherally driven and compartmentalized inflammatory processes may coexist [Compston and Coles, 2008].
Natalizumab is a humanized monoclonal antibody that selectively binds to the α4-subunit of α4β1- and α4β7-integrins expressed on the surface of human leukocytes [Rice et al. 2005]. Natalizumab is approved in the United States for relapsing MS [Biogen, 2015a] and in Europe for the treatment of RRMS [Biogen, 2015b], based on the outcomes of two phase III studies [Polman et al. 2006; Rudick et al. 2006]. These studies in patients with relapsing forms of MS demonstrated that natalizumab significantly reduced the annualized relapse rate, the risk of confirmed disability deterioration over 2 years and the accumulation of new brain MRI lesions. In other placebo-controlled studies, natalizumab has been shown to suppress the evolution of new gadolinium-enhanced lesions into T1-hypointense lesions in patients with relapsing MS (70.5% RRMS; 29.5% SPMS) [Dalton et al. 2004]. There is also evidence that natalizumab efficacy in RRMS is accompanied by reductions in the rate of brain volume loss [Miller et al. 2007; Radue et al. 2010; Rinaldi et al. 2012] and enhanced tissue integrity on diffusor tensor imaging [Fox et al. 2011].
In light of these findings, the efficacy of natalizumab in slowing progression of disability independent of relapses is currently being investigated in a phase IIIb trial in patients with SPMS (ASCEND [ClinicalTrials.gov identifier: NCT01416181]). Here, we summarize the relevant pathophysiology of SPMS and present a biological rationale for the treatment of SPMS with natalizumab, including its potential to reduce chronic intrathecal inflammation and disability progression through several potential mechanisms, as illustrated both by pathophysiological data and post hoc analyses of natalizumab studies that included patients with SPMS.
Natalizumab mechanism of action in RRMS
The principal clinical effect of natalizumab in RRMS is thought to be secondary to blockade of the molecular interaction between α4β1-integrin (also known as very late antigen-4 [VLA-4], expressed by mononuclear inflammatory cells) and vascular cell adhesion molecule-1 (expressed by cerebral vascular endothelial cells). The net effect is reduced leukocyte migration into the CNS and consequent reduction of disease activity [Miller et al. 2003; Polman et al. 2006].
Effects on CNS cellular infiltration and intrathecal antibody production
Among untreated RRMS patients, high lymphocyte counts in the cerebrospinal fluid (CSF) and the presence of oligoclonal bands (OCBs) of immunoglobulin types G and M (IgG and IgM) are associated with markers of axonal degeneration and MS disease activity, including higher CSF levels of neurofilament light-chain protein, with higher MS Severity Score (MSSS) and MRI lesion number [Villar et al. 2015]. Similarly, IgG OCB-negative patients exhibit less global and regional brain atrophy than IgG OCB-positive patients [Ferreira et al. 2014].
Several studies have demonstrated the effects of natalizumab therapy on immunological mechanisms involved in inflammatory MS disease activity in the CNS, as summarized in Table 1. In studies of CSF profiles in RRMS patients treated with natalizumab for at least 1 year, reductions were seen in CSF levels of CD4+ T cells, B cells (especially CD5+) and OCBs (IgM, and to a lesser extent, IgG) [Mancuso et al. 2014; Villar et al. 2012; Harrer et al. 2013]; whereas OCBs reappeared in the CSF of patients who discontinued natalizumab [Harrer et al. 2013; von Glehn et al. 2012]. Similarly, a longitudinal study revealed that the CSF CD4+/CD8+ ratio, IgG and IgM levels and IgG-CSF index declined in samples collected during natalizumab treatment compared with pretreatment [Warnke et al. 2015]. A decrease from pretreatment levels in the CD4+/CD8+ ratio in CSF was also observed in a separate longitudinal prospective study of natalizumab-treated patients [Stüve et al. 2006]. Moreover, the proportion of CD19+ B cells in CSF has been shown to be lower in natalizumab-treated MS patients (n = 59) than in those not treated with natalizumab (n = 17) [Warnke et al. 2015]; whereas increases in mature CD19+ B cells and CD19+, CD10+ pre-B cells in peripheral blood of natalizumab-treated patients were greater than increases in the total peripheral lymphocyte population [Krumbholz et al. 2008].
Summary of the CNS effects of natalizumab in patients with RRMS and in patients with SPMS.

Politis et al. [2013] study population included eight RRMS and two SPMS patients.
CNS, central nervous system; CSF, cerebrospinal fluid; IgG, immunoglobulin type G; IgGIF, relative intrathecal IgG fraction; IgM, immunoglobulin type M; IL, interleukin; MRI, magnetic resonance imaging; NR, not reported; OCB, oligoclonal band; RRMS, relapsing–remitting multiple sclerosis; SPMS, secondary progressive multiple sclerosis.
In addition to its effects on CSF cell counts and OCBs, natalizumab affects other markers of inflammation in the CSF and plasma. In a longitudinal study of RRMS, patients starting natalizumab therapy [Mellergård et al. 2010], had baseline levels of some pro-inflammatory cytokines and chemokines that were significantly higher than in patients with other noninflammatory neurological disorders (for CSF comparisons) or healthy blood donors (for plasma comparisons). Over 1 year, natalizumab therapy resulted in marked declines in total CSF cell counts and CSF levels of pro-inflammatory cytokines (interleukin [IL]-1β, IL-6 and IL-8) and chemokines associated with both T helper (Th) type 1 (CXCL9, CXCL10 and CXC11) and Th2 immunity (CCL22), as well as declines in plasma levels of some cytokines [Mellergård et al. 2010]. In a separate longitudinal study, RRMS patients treated with natalizumab for 1 year showed an increase in the percentage of activated CD4+ and CD8+ T cells producing pro-inflammatory cytokines in the peripheral blood that was thought to be due to sequestration of activated cells in the peripheral circulation [Kivisäkk et al. 2009]. Furthermore, most RRMS patients treated with natalizumab have undetectable, presumably normal CSF levels of the B-cell chemokine CXCL13 [Sellebjerg et al. 2009], which is expressed in demyelinating lesions [Krumbholz et al. 2006] and is associated with the formation of ectopic lymphoid tissue. Collectively, these data illustrate the wide-reaching effects of natalizumab on various CSF markers of inflammation known to be associated with disease activity in RRMS.
Other effects of natalizumab in RRMS
Monoclonal antibodies including natalizumab are thought to reach levels in the intrathecal compartment in the range of approximately 0.1–1.0% of their respective serum levels [Deng et al. 2012]. Consistent with this estimate, a recent study of 15 natalizumab-treated patients with MS (tested 1.0–7.4 weeks after the last natalizumab infusion) found that the median natalizumab concentration was 50.9 μg/ml (range 4.3–109.0) in the serum and 0.11 μg/ml (range 0.01–0.42) in the CSF [Harrer et al. 2015]. When present within the intrathecal compartment, natalizumab may have the potential to exert local direct effects on intrathecal CNS inflammation in addition to its known impact on peripheral leukocyte migration. A CSF substudy of ASCEND will provide further information regarding the biological effects of natalizumab in the CNS [ClinicalTrials.gov identifier: NCT01416181].
It has been suggested that natalizumab may inhibit the interaction of α4β1-expressing leukocytes with ligands in the extracellular matrix in the CNS, such as osteopontin and fibronectin, inhibiting further leukocyte recruitment and thereby contributing to the suppression of intrathecal inflammation [Yaldizli and Putzki, 2009]. Osteopontin is present at elevated levels in the plasma of MS patients compared with healthy control subjects [Kivisäkk et al. 2014], and at elevated levels in the CSF of MS patients compared with patients with other neurological diseases [Khademi et al. 2009]. Osteopontin is expressed in the lesions of progressive MS patients and has been found to be elevated in the blood [Hur et al. 2007] and CSF [Szalardy et al. 2013] of MS patients during relapse, decreasing significantly during recovery from relapse [Börnsen et al. 2011]. Natalizumab treatment has been shown to decrease osteopontin levels in the CSF [Khademi et al. 2009] and plasma [Kivisäkk et al. 2014] of RRMS patients. In a study of RRMS patients receiving natalizumab for 2 years, mean plasma osteopontin levels decreased by approximately 31% (p < 0.005), and this decrease correlated with significant (p < 0.005) improvements in mean global cognitive impairment index values [Iaffaldano et al. 2014].
Fibronectin is expressed in chronically demyelinated MS lesions [van Horssen et al. 2006], where it appears to accumulate [Stoffels et al. 2013]. Natalizumab treatment in patients with RRMS significantly reduced the adhesion of ex vivo peripheral blood mononuclear cells to activated transfected human brain microvascular endothelial cells (THBMECs) under flow conditions; fibronectin containing the CS1 region was identified as the ligand of α4-integrin on the THBMECs [Man et al. 2009].
Pathophysiology of SPMS
Demyelination and loss of axons and neurons
SPMS is characterized by chronic white matter and gray matter neuro-axonal degeneration, cortical demyelination and acceleration of CNS tissue loss, resulting in prominent brain volume loss against a background of global innate inflammatory responses in the CNS parenchyma and adaptive immune responses in the meninges [Friese et al. 2014; Mahad et al. 2015; Reynolds et al. 2011]. Thus, a cascade of mechanisms, including cellular and humoral inflammation, oxidative damage, iron accumulation and mitochondrial damage have been hypothesized to collaboratively induce the sustained CNS tissue damage responsible for the progressive accumulation of disability characteristic of SPMS [Friese et al. 2014; Mahad et al. 2015; Reynolds et al. 2011]. Patients with SPMS at autopsy demonstrate slow expansion of pre-existing demyelinating white matter plaques, the borders of which show active demyelination and axonal injury with infiltration by small numbers of diverse inflammatory cells, including T cells, B cells (predominantly in perivascular cuffs), plasma cells, monocytes and activated microglia [Frischer et al. 2009; Kutzelnigg et al. 2005; Reynolds et al. 2011].
Brain volume loss in SPMS affects cortical gray matter much more than white matter [Fisniku et al. 2008; Furby et al. 2010]. Subpial lesions are the most abundant type of cortical lesion in SPMS [Kutzelnigg et al. 2005; Magliozzi et al. 2007; Moll et al. 2008], and appear to be specific to MS, as they are absent in human non-MS inflammatory and noninflammatory brain diseases [Kutzelnigg et al. 2005; Mahad et al. 2015; Moll et al. 2008]. Diffuse injury of normal-appearing white matter (NAWM) is also a hallmark of SPMS [Kutzelnigg et al. 2005], with prominent widespread white matter-microglial activation and perivascular inflammation, accompanied by structural changes at the nodes of Ranvier [Howell et al. 2010] despite a paucity of gadolinium-enhanced and new T2 lesions on brain MRI [Cohen et al. 2002; Kutzelnigg et al. 2005]. The resultant neuro-axonal loss is reflected in increased sodium concentration within lesions, NAWM and cortical and deep gray matter, with higher concentrations seen in SPMS patients and in MS patients with greater levels of disability across the MS spectrum [Paling et al. 2013].
It has been speculated that disability progression in SPMS may result from neurodegeneration, independent of inflammation [Lassmann, 2007a]. Evidence for this includes data from serial MRI studies showing that gadolinium-enhanced lesions are less common in primary progressive MS (PPMS) patients and SPMS patients without superimposed relapses [Kidd et al. 1996]. Similarly, areas of cortical demyelination in patients with chronic forms of MS (SPMS and PPMS) do not demonstrate increased leukocyte infiltration or altered distribution of lymphocyte subsets or microglial activation [Bø et al. 2003]. In contrast, cortical demyelinating lesions in patients with early MS are generally inflammatory, as demonstrated in a study of biopsy specimens, which also revealed that meningeal inflammation was topographically associated with cortical demyelination: in patients who had sufficient meningeal tissue for study [Lucchinetti et al. 2011]. The relatively noninflammatory nature of cortical demyelinating lesions in SPMS is consistent with the observation that despite reducing focal white matter inflammation measured by gadolinium enhancement, immunotherapies have had little effect on brain volume loss and disability progression in progressive forms of MS [Coles et al. 2006]. However, a detailed autopsy study using age-matched control subjects without neurological disease found that neurodegeneration in RRMS and SPMS does not occur above the levels observed in normal aging in the absence of CNS inflammation [Frischer et al. 2009]. This supports the contrary hypothesis that disease progression in SPMS results from chronic CNS-based inflammation trapped behind the BBB, which causes widespread, lower-grade, ongoing diffuse demyelination and axonal injury [Kutzelnigg et al. 2005; Lassmann, 2007b].
CXCL13 and CNS ectopic lymphoid tissue
B cells and plasma cells are found in the CSF and focal lesions of MS patients [Esiri, 1977; Lucchinetti et al. 2000], and are responsible for intrathecal production of OCBs [Colombo et al. 2000; Holmøy, 2009]. In addition, several studies in MS and animal models of autoimmune CNS demyelination, such as experimental autoimmune encephalitis (EAE), have documented prominent intrathecal inflammation [Aloisi et al. 2008; Columba-Cabezas et al. 2003, 2006; Magliozzi et al. 2004, 2007; Serafini et al. 2004, 2006]. A notable finding in SPMS is the presence of mature meningeal ectopic lymphoid follicle (ELF)-like structures in 41% of cases who had autopsy brain tissues available for examination from the UK MS tissue bank [Magliozzi et al. 2007]. Moreover, when the presence of either ELF-like structures or more diffuse lymphocyte infiltrates was assessed in a larger sample of SPMS autopsies, evidence of meningeal lymphocytic infiltration was found in the majority (87%) [Howell et al. 2011].
CXCL13 plays a key role in the accumulation and maintenance of ectopic lymphoid tissues [Aloisi et al. 2008; Gunn et al. 1998; Legler et al. 1998; Magliozzi et al. 2004; Serafini et al. 2004] and is present at elevated levels in the CSF [Krumbholz et al. 2006; Sellebjerg et al. 2009; Edwards et al. 2013] and serum [Festa et al. 2009] of patients with active MS. Although CSF levels of CXCL13 and osteopontin in SPMS patients are similar to or lower than those in stable RRMS patients, they correlate with CSF markers of neuro-axonal damage and demyelination [Edwards et al. 2013; Khademi et al. 2011; Romme Christensen et al. 2013]. Importantly, CSF levels of CXCL13 are greater in OCB-positive than OCB-negative MS patients [Khademi et al. 2011] and are positively correlated with CSF B-cell counts as well as the IgG-CSF index [Khademi et al. 2011; Krumbholz et al. 2006; Ragheb et al. 2011; Sellebjerg et al. 2009].
Microglial activation
Although macrophages recruited into the CNS and resident brain macrophages (microglia) react to any CNS injury, playing a well-established role in clearing myelin debris [Vogel et al. 2013], it is increasingly recognized that these cells may also be pathogenic effector cells in MS [Hickey, 1999]. Positron emission tomography (PET) studies have shown that activated microglia/macrophages are increased in patients with RRMS and SPMS compared with healthy controls [Politis et al. 2012] and that their increased presence was correlated with disability assessed by the Expanded Disability Status Scale (EDSS) [Politis et al. 2012]. This most likely reflects changes occurring in the gray matter of the SPMS patients, since another study found no increase in activated microglia in patients with RRMS relative to healthy controls [Takano et al. 2013]. In a more recent PET study, the presence of activated microglia/macrophages was increased diffusely in NAWM but not in the cortical gray matter of patients with SPMS relative to healthy controls [Rissanen et al. 2014]. The authors hypothesized that the difference between their findings and those of Politis and colleagues [Politis et al. 2012] might have resulted from different data processing and modeling approaches; although they cannot rule out neuropathological differences between the two relatively small study groups [Rissanen et al. 2014].
Regardless of their location within the CNS, the pro-inflammatory and demyelinating activity of activated resident microglia and CNS-infiltrating blood-derived macrophages may be crucial for MS lesion formation [Koning et al. 2007; Trapp and Nave, 2008; Weiner, 2008]. In progressive forms of MS, active demyelination and axonal injury in white matter are associated with microglial activation and oxidative burst in microglia. This in turn leads to gene deletions in neuronal mitochondrial DNA and clonal expansion of defective mitochondria, which may lead to hypoxia and apoptosis in the final pathways of tissue injury in MS lesions [Mahad et al. 2015]. The importance of activated microglia/macrophages in the pathogenesis of SPMS is highlighted by an autopsy study of patients who died after therapeutic chemotherapy followed by bone marrow transplantation, which revealed an absence of meningeal B-cell follicles, B cells and plasma cells in the brain, while there was ongoing axonal injury associated with activated macrophages/microglia [Metz et al. 2007].
Potential impact of natalizumab on pathophysiological mechanisms in SPMS
As mentioned previously, data exist showing that natalizumab reduces CSF levels of chemokines relevant to the formation and maintenance of meningeal lymphocyte aggregates, which may be involved in the pathophysiology of SPMS. In addition to the effects observed with natalizumab treatment in patients with RRMS [Sellebjerg et al. 2009], reductions of CXCL13, osteopontin and neurofilament in the CSF have also been demonstrated in patients with progressive MS (SPMS or PPMS) treated with natalizumab compared with pretreatment levels [Romme Christensen et al. 2014] (Table 1). In contrast, no change was seen in these CSF biomarkers of inflammation, axonal damage or demyelination after 1 year of treatment with placebo or MBP82–98 peptide [Romme Christensen et al. 2013], a synthetic peptide with amino acid sequence corresponding to amino acids 82–98 of myelin basic protein, in patients with SPMS [Freedman et al. 2011]. The fact that natalizumab has effects in SPMS patients on biomarkers that are not affected by other compounds such as MBP82–98 suggests a potential role for natalizumab in this population. However, further exploration of specific biomarkers is needed to better understand their relevance in SPMS. For example, while osteopontin is known to be expressed in MS lesions [Chabas et al. 2001], its expression within the meningeal space has not been demonstrated. Likewise, the relevance of fibronectin expression in chronic MS lesions [van Horssen et al. 2006] is unclear, but it is possible that natalizumab’s effect on the binding of peripheral blood cells to fibronectin [Man et al. 2009] could contribute to reductions in intrathecal inflammation.
Since natalizumab’s target, the VLA-4 integrin, plays a major role in B-cell trafficking across the BBB [Stüve et al. 2009], there are fewer B cells in the CSF of natalizumab-treated patients with MS than in MS patients who are not treated with natalizumab [Stüve, 2008; Stüve et al. 2009]. It is possible that natalizumab’s inhibition of B-cells ingressing through a compromised BBB may have a positive impact in SPMS, given the presence of B cells in lymphoid-like follicles of SPMS. However, once the immune response becomes largely confined to the CNS behind a relatively intact BBB, local expansion of B-cell clones within the lymphoid structures may primarily account for increases in intrathecal B cells [Reynolds et al. 2011].
Natalizumab also appears to modulate microglial function by inhibiting the transmigration of VLA-4-expressing macrophages and dendritic cells into the CNS [de Andres et al. 2012; Khademi et al. 2009; Mindur et al. 2014]. This has been demonstrated in studies using markers of microglial activation with PET imaging. Natalizumab treatment of RRMS patients resulted in decreased cerebral microglial activation [Maoz et al. 2014], and reductions in cortical microglial activation following a year of natalizumab therapy were associated with stabilization of physical disability [Politis et al. 2013]. Finally, inhibition of VLA-4 on dendritic cells may decrease the capacity of these and other cells to efficiently present antigen and activate T cells [Börnsen et al. 2012; de Andres et al. 2012; del Pilar Martin et al. 2008]. These effects on CNS macrophage infiltration, microglial and/or blood-derived macrophage activation and dendritic-cell function may be directly, and more likely indirectly, beneficial in SPMS by decreasing the number of inflammatory cells in the perivascular and subarachnoid spaces.
Clinical experience with natalizumabin SPMS
The efficacy of natalizumab in SPMS patients is currently being evaluated in ASCEND, a multicenter, randomized, double-blind, placebo-controlled phase IIIb study of the efficacy of natalizumab in reducing disability progression independently of relapses [ClinicalTrials.gov identifier: NCT01416181]. Criteria for enrollment in ASCEND are shown in Table 2.
Key eligibility criteria in ASCEND [ClinicalTrials.gov identifier: NCT01416181].
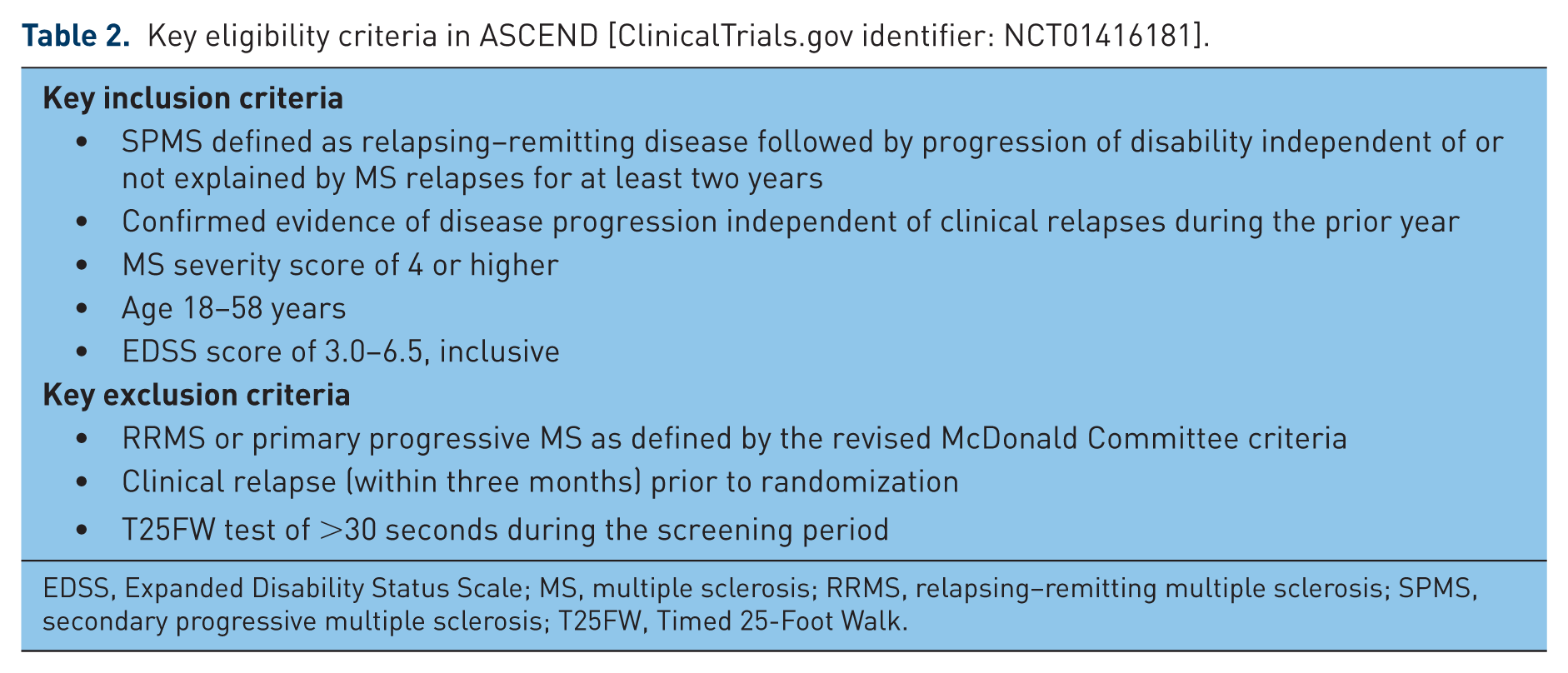
EDSS, Expanded Disability Status Scale; MS, multiple sclerosis; RRMS, relapsing–remitting multiple sclerosis; SPMS, secondary progressive multiple sclerosis; T25FW, Timed 25-Foot Walk.
While no previous trial has assessed the efficacy of natalizumab in an exclusively SPMS population, retrospective analyses [Cadavid et al. 2013] have been conducted with data from natalizumab-treated SPMS patients who participated in the following two studies: (1) a 6-month placebo-controlled phase IIb study (MS231) of RRMS and relapsing SPMS patients, who were monitored for an additional 6 months after the randomized treatment period [Miller et al. 2003] and (2) an 8-month open-label phase Ib study (MS102) of natalizumab in RRMS patients, or SPMS patients with a history of disability progression without superimposed relapses [Woodworth et al. 2013]. A total of 66 patients with SPMS from MS231 and 52 patients with SPMS from MS102 were included in the analyses. Given the relatively short durations of the MS231 and MS102 studies and the observation that EDSS in patients with a baseline score > 5.0 is less responsive to change than T25FW [Cadavid et al. 2010], a post hoc analysis of efficacy on ambulation was conducted using the T25FW. ‘Responders’ were defined as patients who walked faster in two of three post-baseline T25FW assessments than in their best pre-dose walk. In MS231, the percentage of T25FW responders was higher in the natalizumab group (24% [10 of 41]) than in the placebo group (12% [3 of 25]), and in MS102, which lacked a placebo group, a similar proportion of T25FW responders was seen with natalizumab (22% [10 of 45]) [Cadavid et al. 2013]. The potential therapeutic efficacy of natalizumab in SPMS is further supported by the results of a larger post hoc T25FW responder analysis of 548 SPMS patients and a more disabled subset of 358 RRMS patients (baseline EDSS score ⩾ 3.5 and T25FW time > 5 seconds) enrolled in previous clinical studies [Cadavid et al. 2013]. The proportion of responders, using various definitions of improvement in T25FW (e.g. faster walking time over a shorter [6–9 month] or longer [24–30 month] treatment period relative to the best predose walking time), was greater in patients treated for up to 30 months with natalizumab alone, or in combination with intramuscular interferon beta-1a (IFNβ-1a) than among patients given placebo or IFNβ-1a alone. Finally, in a phase IIa study in patients with PPMS and SPMS, EDSS scores improved and T25FW times were stable after 60 weeks of natalizumab therapy [Romme Christensen et al. 2014].
In summary, while the above studies were not designed to assess whether natalizumab is effective in reducing disability progression unrelated to relapses in an SPMS population, the exploratory findings formidably support the prospective evaluation of natalizumab in the ongoing ASCEND SPMS study.
Discussion
As RRMS and SPMS represent a continuum of the same disease [Lublin et al. 2014], mechanisms that predominate in RRMS or SPMS are likely to overlap in individual patients, particularly during the gradual transition from RRMS to SPMS. In practice, diagnosis of SPMS can be challenging given that (1) superimposed relapses during the transition period of RRMS to SPMS may make it difficult for the clinician to identify and differentiate insidious disability progression from stepwise accumulation of disability due to relapses [Lublin et al. 2014] and (2) the manifestations of progression may be more subtle at onset [Rudick et al. 2014], particularly in patients with less severe disease as reflected by MSSS [Roxburgh et al. 2005]. These factors are accounted for in the eligibility criteria of ASCEND (see Table 2, first three bullets of inclusion criteria).
The overlap between RRMS and SPMS suggests treatments that are efficacious in RRMS patients might also benefit SPMS patients. Some treatments approved for RRMS have been studied in SPMS [Ontaneda et al. 2015]. However, anti-inflammatory treatments investigated for treating SPMS should have a plausible biological mechanism to address the CNS-compartmentalized inflammatory process that predominates in SPMS. As natalizumab prevents the transmigration of leukocytes across the BBB [Yednock et al. 1992], clinical benefit might be facilitated not only in RRMS but also in SPMS. The net effect of natalizumab treatment in SPMS may be a reduction in chronic intrathecal (meningeal and CNS parenchymal) inflammation and production of pro-inflammatory cytokines, which in turn may decrease the ongoing CNS demyelination, axonal injury and neuronal loss that are key drivers of progression in SPMS.
In addition to the clinical benefits of natalizumab therapy seen in phase III studies of patients with relapsing forms of MS [Polman et al. 2006; Rudick et al. 2006], other studies have revealed evidence of enhanced tissue integrity and improved axonal metabolism in some natalizumab-treated RRMS patients, suggesting that reducing inflammation may enable endogenous repair mechanisms to take place during natalizumab therapy [Fox et al. 2011; Wiebenga et al. 2015]. While it is unclear whether or to what extent this may be pertinent in SPMS, it is encouraging that natalizumab treatment improved magnetization transfer ratios in the cerebral cortex and normal-appearing white matter of SPMS/PPMS patients [Romme Christensen et al. 2014].
In conclusion, clinical findings from short-term studies with natalizumab in patients with SPMS, combined with evidence indicating its potential to exert beneficial effects on multiple aspects of the pathophysiology associated with the development of SPMS, suggest that natalizumab represents a promising candidate for the treatment of SPMS, a condition for which available therapeutic options are limited. The efficacy of natalizumab for treatment of secondary progression, independent of relapses, is being evaluated in the large, ongoing phase IIIb ASCEND study. There is a high unmet need for effective treatments for SPMS, and data from ASCEND should demonstrate whether preliminary findings with natalizumab in short-term studies and its multiple potentially beneficial mechanisms of action of VLA-4 blockade translate into clinically meaningful efficacy in this serious disease.
Footnotes
Acknowledgements
Mary Goodsell, on behalf of Infusion Communications, wrote the first draft of the paper based on input from authors, and Joshua Safran of Infusion Communications copyedited and styled the manuscript per journal requirements. Biogen reviewed and provided feedback on the manuscript to the authors. The authors had full editorial control of the manuscript, made extensive contributions to follow-up drafts, and provided final approval of all content.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Biogen provided funding for editorial support in the development of this manuscript.
Conflict of Interest Statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.S. has served on scientific advisory boards, been on the steering committees of clinical trials, served as a consultant, received support for congress participation, received speaker honoraria, or received research support for his laboratory from Bayer Schering, Biogen, Genzyme, Lundbeck, Merck Serono, Novo Nordisk, Novartis, Sanofi, Schering Plough and Teva. D.C. and D.S. are full-time employees of Biogen and own stock/stock options in Biogen. D.M. was a full-time employee of Biogen and owned stock/stock options in Biogen when this manuscript was developed. L.M.V. has served as a consultant, received support for congress participation, received speaker honoraria, or received research support for her laboratory from Bayer Schering, Binding Site, Biogen, Genzyme, Merck Serono, Novartis and Teva. R.R. has received speaker honoraria from Biogen and Novartis and research support from EMD Serono.