
Abstract
A superficial siderosis of the central nervous system following a traumatic cervical nerve root avulsion usually leads to gait difficulties and hearing loss, whereas back pain is described only rarely. Here we report on the first case with circadian occurrence of severe back pain as the only symptom of a superficial siderosis. We present a case with the most severe pseudoradicular lumbosacral pain occurring daily at noon for the past 5 weeks. The 48-year-old male white patient did not complain of pain in the morning. A traumatic root avulsion 26 years earlier led to a brachial plexus palsy and Horner’s syndrome in this patient. Superficial hemosiderosis in cranial MRI and examination of the cerebrospinal fluid revealing massive red blood cells as well as xanthochromia and elevated protein levels (742 mg/l) led to the diagnosis of a superficial siderosis. A pseudomeningocele caused by a cervical nerve root avulsion is described as a rare reason for superficial siderosis. Surgery on a pseudomeningocele, diagnosed by MRI, led to an immediate disappearance of complaints in our case. Regular neurological investigation and possibly repeated lumbar puncture to exclude superficial siderosis should be considered in cases with severe back pain and a history of traumatic root avulsion. Modern susceptibility weighted MR imaging (SWI) techniques, sensible to the detection of superficial hemosiderosis, might be helpful in the making of a diagnosis.
Introduction
Superficial siderosis (SS) of the central nervous system several years after a traumatic cervical nerve root avulsion usually leads to gait difficulties and hearing loss, whereas back pain is described only rarely [Aquilina et al. 2005; Urban et al. 1999]. In addition, transient episodes of facial nerve palsy, tinnitus and involvement of other cranial nerves have been reported as early symptoms of SS with spasticity, ataxia, sphincter dysfunction and dementia in the further course of the disease [Aquilina et al. 2005; Bonito et al. 1994; Bracchi et al. 1993; Tapscott et al. 1996]. An early detection and recognition of the initial nonprogressive symptoms coupled with timely surgical management has been recommended in order to minimize the degree of neurological disability [Aquilina et al. 2005].
Subarachnoid bleeding due to a traumatic pseudomeningocele of the brachial plexus has been described as an unusual cause of SS [Bonito et al. 1994; Murata et al. 2012]. Since lumbar puncture results might be normal depending on when the examination takes place, a regular neurological examination is recommended [Aquilina et al. 2005]. No reports so far have described a circadian dependency of SS symptoms.
Case report
Traumatic root avulsion (C6-T1) due to a motorcycle accident 26 years earlier led to a left side brachial plexus palsy and Horner’s syndrome in our patient. Four and 9 years before the current presentation, a lumbosacral pain occurred without it being possible to make a diagnosis. Lumbar MRI revealed no cause for the origin of the pain. Thus, a psychosomatic cause for the symptoms, which improved without therapy, was discussed at that time. A lumbar puncture for examination of the cerebrospinal fluid was not performed. The patient now complained of strongest pseudoradicular lumbosacral pain occurring daily at noon for the past 5 weeks. The patient did not complain of pain in the morning. Cranial MRI showed multiple susceptibility artifacts temporobasal and cerebellar both sides (Figure 1). Thus, an examination of cerebrospinal fluid was performed at the current examination, since it is known that in some patients with an earlier traumatic cervical nerve root avulsion, back pain might be caused by a SS [Urban et al. 1999]. This examination revealed massive red blood cells in the cerebrospinal fluid as well as xanthochromia and elevated protein levels (742 mg/l) whereby the diagnosis of SS was made. Surgery of a pseudomeningocele, diagnosed by cervical MRI (see Figure 2), by laminectomy and by the use of TachoSil [Rickenbacher et al. 2009] led to an immediate disappearance of complaints.

Susceptibility weighted imaging (SWI) showing superficial hemosiderosis.
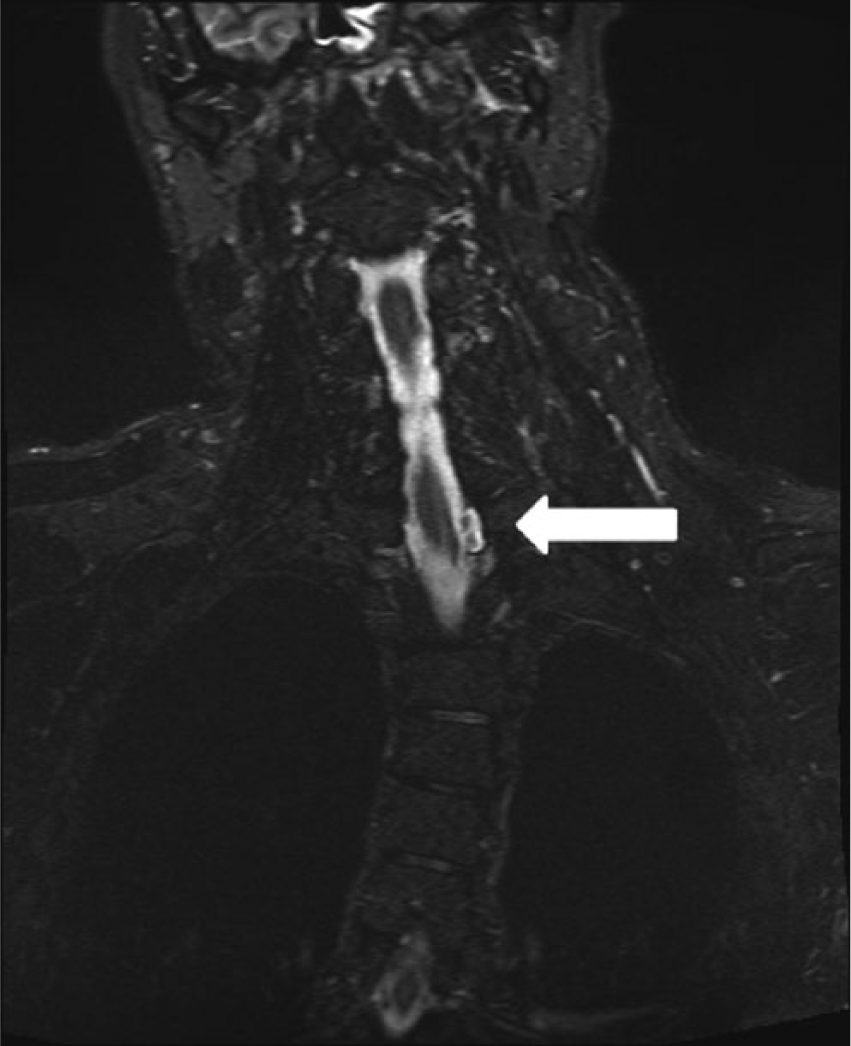
Pseudomeningocele detectable in MRI (short tau inversion recovery [STIR] sequence) 26 years after a motorcycle accident.
Discussion
As Aquilina and colleagues stated, in cases of brachial plexus trauma with cervical nerve root avulsions, regular neurological examination including evaluation of the eighth nerve function (clinical examination and audiometry) should be performed. These patients should be offered CNS MRI upon detection of myelopathy, ataxia or early cranial nerve symptoms, particularly those involving the vestibulocochlear and facial nerves [Aquilina et al. 2005]. As shown in our case, the SS symptomatology and severity of symptoms might be highly variable and change over time. Accordingly lumbar puncture results might be normal depending on when the examination takes place [Aquilina et al. 2005]. Thus, we would recommend that repeated lumbar puncture to exclude SS should be considered in cases with severe back pain and a history of traumatic root avulsion, as in our case. T2 axial brain MR images are known to be sensitive to the detection of hypointense signal changes in several regions of the brain, including the medial temporal lobe, the brainstem and the cerebellar as a hint for SS [Aquilina et al. 2005]. Modern susceptibility weighted MR imaging (SWI) techniques (see Figure 1), sensible to the detection of superficial hemosiderosis, might be even more sensitive and therefore helpful in making the diagnosis.
As a most impressive and possibly misleading symptom, the patient in our case describes a severe pain requiring morphine as pain medication only in the second half of the day with no pain in the morning. This symptomatology has not been described so far in cases with SS. Possible pathophysiological mechanisms remain unclear. As a possible explanation, stimulation of sacral and lumbar roots due to sedimented erythrocytes and hemosiderin hours after getting up might explain the circadian aspect of the symptomatology. A pathophysiological context between SS and the circadian back pain is supported by the relief of symptoms after operation of the traumatic pseudomeningocele as the origin of the SS. The patient refused a control lumbar puncture in the further course several weeks after operation, since he was free from pain.
To the best of the authors’ knowledge, the pathophysiological mechanism for subarachnoid bleeding due to a traumatic pseudomeningocele is unknown at this time. In a case with an arachnoid cyst causing SS, Cheng and colleagues have suggested that increased epidural pressure micro traumatizing the fragile internal venous plexus leads to recurrent microbleeding and thus to a superficial siderosis [Cheng et al. 2011]. Similar mechanisms might be involved in our case.
Footnotes
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Conflict of interest statement
The authors have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.