
Abstract
Background:
During surgical treatment for ulcerative colitis, an ileal pouch-anal anastomosis is often constructed. Pouchitis, the most common complication after this surgery, substantially reduces patients’ quality of life (QoL). In chronic pouchitis, antibiotic treatment often proves ineffective. Fecal microbiota transplantation (FMT) has emerged as a potential treatment for chronic pouchitis.
Objectives:
To determine the effect of FMT on QoL in patients with chronic pouchitis.
Design:
An exploratory post hoc analysis of data from the MicroPouch trial. A double-blinded, placebo-controlled study comprising a 4-week intervention period and 12-month follow-up.
Method:
Thirty patients with chronic pouchitis were randomized 1:1 to receive either FMT or placebo. Treatment was administered by enema once daily for 2 weeks, then every other day for the following 2 weeks. QoL was assessed using three questionnaires—the Short Inflammatory Bowel Disease Questionnaire (SIBDQ), the Pouch Dysfunction Score (PDS), and the 36-item Short Form Questionnaire (SF-36)—at baseline and at subsequent follow-ups.
Results:
At the 30-day follow-up, FMT-treated patients showed a significant decrease in QoL from baseline, measured by the SIBDQ (p = 0.03). Within the FMT group, the PDS did not change significantly from baseline to day 30 (p = 0.36). The placebo group reported higher SF-36 QoL scores at both baseline and day 30 (p = 0.02), although neither group showed significant within-group changes over time.
Conclusion:
In patients with chronic pouchitis, FMT may temporarily worsen symptoms and reduce QoL, as indicated by three QoL questionnaires showing no improvement or poorer outcomes versus placebo.
Plain language summary
Some patients with ulcerative colitis need surgery in which the colon is removed, and a new internal pouch is created to help store stool. A common problem after this surgery is pouchitis, an inflammation of the pouch that can cause frequent bowel movements, pain, and fatigue. These symptoms can greatly affect quality of life and overall well-being. When pouchitis becomes long-lasting (chronic), antibiotics often stop being effective. Fecal microbiota transplantation (FMT) is a treatment that transfers gut bacteria from a healthy donor to a patient. It has been suggested as a possible new treatment for chronic pouchitis, but its effects on patients’ quality of life are not well understood. This study aimed to examine whether FMT improves quality of life in patients with chronic pouchitis compared with a placebo group.
Introduction
Pouchitis is the most common long-term complication of ileal pouch-anal anastomosis (IPAA) performed for medically refractory ulcerative colitis (UC) or familial adenomatous polyposis (FAP). 1 Although medical treatment using steroids, immunosuppressants, and increasingly biologics is the primary approach for UC, failure rates remain high, with more than 10% of patients ultimately requiring surgery.2,3 The preferred surgical procedure involves a colectomy followed by IPAA with creation of a J-pouch.2,4 –6 The incidence of pouchitis has been reported to range from 14% to 59% and to increase with longer follow-up.7 –10 A systematic review and meta-analysis reported a pooled pouchitis prevalence of 32% among patients operated for UC and 6% among those operated for FAP. 11 Pouchitis is an inflammatory disorder of the ileal pouch following IPAA. 12 The pathogenesis of pouchitis is not fully understood, but it is hypothesized to involve a combination of gut microbiota dysbiosis, mucosal immune dysregulation, and genetic predisposition.5,13,14 Antibiotics, typically metronidazole or ciprofloxacin, are the preferred treatments for acute pouchitis. 15 Second-line treatment remains challenging, although biologic therapies show some promise. Vedolizumab and infliximab are considered safe and may be effective in some patients, although further evidence is required. 16 In approximately 20% of patients, pouchitis becomes chronic, either antibiotic-dependent, requiring repeated or constant antibiotic therapy, or antibiotic-refractory, unresponsive to standard antibiotic treatment.2,12 Patients with chronic pouchitis face a high risk of pouch failure, with approximately 10% ultimately requiring pouch removal and conversion to an ileostomy.17,18
Fecal microbiota transplantation (FMT) is a therapeutic procedure that involves transferring stool from a healthy donor to a patient’s gastrointestinal tract with the aim of restoring a balanced gut microbiota. 19 FMT has shown promising results in the treatment of UC, where it appears safe and potentially effective in moderate-to-severe cases. 20 FMT has therefore been proposed as a potential option for chronic pouchitis to restore microbial balance. 15 However, three small randomized controlled trials (RCTs) in patients with chronic pouchitis have demonstrated limited clinical efficacy or remission with FMT compared with placebo.14,21,22 FMT is an established and effective therapy for infection with Clostridioides difficile. Studies on FMT for recurrent C. difficile infection (rCDI) have demonstrated significant post-treatment improvements in quality of life (QoL). 23 In 2023, Zaman et al. 24 conducted a systematic review and meta-analysis on FMT use in chronic pouchitis. Of the nine studies included, only two reported QoL outcomes, yielding conflicting findings; Landy et al. 25 observed no significant change, whereas Karjalainen et al. 22 ’s RCT demonstrated a significant improvement.22,24,25 Given the limited number of studies evaluating QoL, definitive conclusions cannot yet be drawn.
This study represents a post hoc exploratory analysis of the MicroPouch trial by Kousgaard et al. 14 The original study focused on short-term outcomes after 30 days: Clinical remission as the primary endpoint, and clinical response, changes in Pouch Disease Activity Index (PDAI) sub-scores, and stool frequency as secondary outcomes. The present analysis is based on the prespecified 1-year QoL follow-up of the MicroPouch cohort. This analysis is presented separately to provide a detailed assessment of QoL over a 1-year period, allowing evaluation of whether any effects of FMT are immediate or delayed. A delayed response could be influenced by adverse events. This study is important as QoL is the most valuable outcome for patients with this debilitating disease. The primary aim was to assess the long-term effects of FMT on QoL compared with placebo using three QoL instruments. Secondary aims included evaluating the symptomatic sub-score of the PDAI and assessing the effect of open-label FMT on QoL during a 3-month follow-up period. 14
Methods
The project was approved by the Regional Research Ethics Committee of Northern Jutland, Denmark (N-20150021). Written informed consent was obtained. The study is registered at ClinicalTrials.gov (Trial number NCT04100291; htttp://clinicaltrials.gov/). 14
Study design
Thirty patients with chronic pouchitis participated in the original MicroPouch RCT. A power calculation was performed, and an aim of 50 participating patients was set. Unfortunately, the study was terminated prematurely after inclusion of 30 patients, because of the coronavirus disease in 2019. 14 All patients had previously undergone IPAA surgery with a J-pouch for UC and had experienced symptoms of chronic pouchitis, including diarrhea, rectal bleeding, and abdominal cramps, for more than 4 weeks. Furthermore, all patients had required antibiotic therapy for three or more pouchitis episodes within the past year. Patients were eligible for inclusion if their total PDAI score was 7 or higher. The PDAI comprises three components: clinical symptoms, endoscopic findings, and histologic assessment. 14 The patients were excluded if they were using antibiotics, had immunosuppression, pouchitis caused by other than UC, any serious food allergies, pregnancy, or treatment with probiotics within the 2 weeks before the trial. 14
Patients were recruited from five Danish hospitals: the Department of Gastrointestinal Surgery, Aalborg University Hospital; the Department of Hepatology and Gastroenterology, Aarhus University Hospital; the Department of Medical Gastrointestinal Diseases, Odense University Hospital; the Gastrounit, Copenhagen University Hospital, Hvidovre; and Køge Hospital, Zealand University Hospital.
Trial design, donors, and FMT preparation
The study was designed as a randomized, double-blind, placebo-controlled clinical trial. 14 The 30 patients were randomized 1:1 to receive either FMT or placebo; 15 received FMT and 15 received placebo.
Fecal donors were recruited at the Blood Bank at Aalborg University Hospital. Exclusion criteria included the following: any bowel system disease, previous bowel surgery, abnormal stool frequency (>2 per day), and use of prescribed or natural medicines. The donors were thoroughly screened with a blood test and fecal test for any transmissible diseases (bacterial or viral). No specific microbial composition was required. See the MicroPouch study for further information. 14 Thirteen healthy donors were approved for fecal donation.
Enemas were chosen as the route of administration, as they can be self-administered at home and are less invasive than colonoscopy or gastroscopy, thereby minimizing the risk of serious adverse events. European consensus guidelines recommend multiple administrations when using enemas to enhance clinical response.13,26 The fecal samples were handled in accordance with international consensus. 27 Fecal samples were not processed under aerobic conditions. Enemas were prepared by mixing 50 g of donor stool with sterile water, then homogenizing and filtering. Finally, it was mixed with glycerol to a final volume of 100 mL. The placebo enemas consisted of sterile water, 10% glycerol, and brown food color (E150) in 100 mL enema bottles to resemble FMT enemas. 14 The enemas were frozen at −80 degrees until delivery to the patient. The patient stored the bottles at −20 degrees at home until use. The enemas had to be room temperature when administered. No bowel preparation was administered prior to the enema treatment. 14
At inclusion, all patients underwent pouchoscopy and completed the QoL questionnaires.
During the trial, all patients received treatment with an enema once daily for 14 consecutive days, followed by treatment every second day for an additional 14 days. In total, each patient received 21 days of active treatment, either FMT or placebo (see Figure 1). Further details have been published earlier. Any use of antibiotics, immunomodulators, or biologics during the trial led to exclusion. 14

Flowchart of the trial design (inclusion, day 30, 6-month, and 12-month follow-up).
All patients were followed up on days 14 and 30 of treatment, as well as 6 and 12 months after completing treatment (see Figure 1). These follow-ups included assessments of symptoms, adverse events, stool frequency, and completion of QoL questionnaires. A pouchoscopy was performed again 30 days after initiation of treatment, and the findings were used to calculate a PDAI score. All pouchoscopies were performed by a blinded endoscopist. Adverse events were defined as any medical problem or symptom occurring during the treatment period. 14
After completing the MicroPouch study, all patients were offered the opportunity to participate in an open-label FMT treatment phase. Eleven patients chose to participate and received FMT using the same treatment regimen as in the MicroPouch RCT study. Each patient underwent 21 treatments over a 30-day period. QoL questionnaires were completed at baseline, at day 14, and at the 30-day follow-up. A symptom assessment using the clinical PDAI (cPDAI) score was performed at the 30-day follow-up, as well as at 1 and 3 months after FMT. 14
Quality of life
QoL was assessed using three questionnaires at baseline, day 14, day 30 of treatment, and at 6 and 12 months after treatment. The questionnaires were administered electronically at the pre-determined timepoints using the online tool in REDCap hosted at Aalborg University Hospital, Aalborg, Denmark (redcap.rn.dk) for the patients to answer at home.
Two questionnaires were used to assess symptoms related to pouchitis. The first questionnaire is the Danish-validated Pouch Dysfunction score (PDS), 28 which consists of 14 questions assessing the severity of pouchitis symptoms and their impact on daily life. Each response corresponds to a specific value, and the total score, ranging from 0 to 8.5, is calculated by summing these values. A lower score indicates fewer symptoms and a higher QoL, whereas a higher score reflects more severe symptoms and a lower QoL. The second questionnaire is the Short Inflammatory Bowel Disease Questionnaire (SIBDQ), which is validated for UC patients, 29 but is also considered applicable to patients with pouchitis. 30 This questionnaire includes 10 items focusing on symptoms and general mood over the preceding 2 weeks. The total score is obtained by summing the responses to all 10 questions. Score ranges from 10 to 70 points. A lower score indicates a poorer QoL, while a higher score reflects a better QoL. The final questionnaire assesses overall health-related QoL. The 36-Item Short Form Survey (SF-36) is a validated, generic questionnaire that evaluates eight domains of QoL: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. These domains are grouped into two dimensions: physical and mental.31,32 A sub-score is calculated for each of the eight domains, and the means of these sub-domains are used to determine the total score. Total scores range from 0 to 100. A lower total score indicates a poorer QoL, whereas a higher score reflects a better QoL.
Statistical analysis
Descriptive data are presented in Table 1 with data from the MicroPouch study. 14 Due to the small sample size, Mann–Whitney U was used for continuous data and Fisher’s exact test for categorical data at the time of inclusion (n = 30). For QoL assessment, the PDS and SIBDQ scores were calculated by summing responses to all items. For the SF-36 questionnaire, a subscore was calculated for each of the eight domains, and the total score was derived from the mean of these eight subscores. Mean scores for each of the three QoL questionnaires in the FMT and placebo groups were compared at baseline, 30-day follow-up, and at 6- and 12-month follow-ups using linear regression analysis. In these analyses, the QoL score at each follow-up time point was the dependent variable, while treatment group (FMT vs placebo) and the corresponding baseline value of the outcome were independent variables. Furthermore, within-group changes from baseline to each follow-up were compared using linear regression models with the change score (follow-up minus baseline) as the dependent variable and controlling for baseline scores. No additional covariates were included due to the limited sample size. Missing data were not imputed. All analyses were performed as complete-case analyses, including only participants with available data for the variables included in each model. Associations between QoL scores (SF-36, SIBDQ, and POUCHDYS) and disease activity (PDAI) were assessed using linear regression analyses and reported as correlation coefficients (r). Analyses were performed separately for the FMT and placebo groups at baseline and at 30-day follow-up. Differences in associations between groups were evaluated by testing the equality of regression slopes. All analyses were based on complete cases.
Baseline characteristics in the FMT and placebo group.
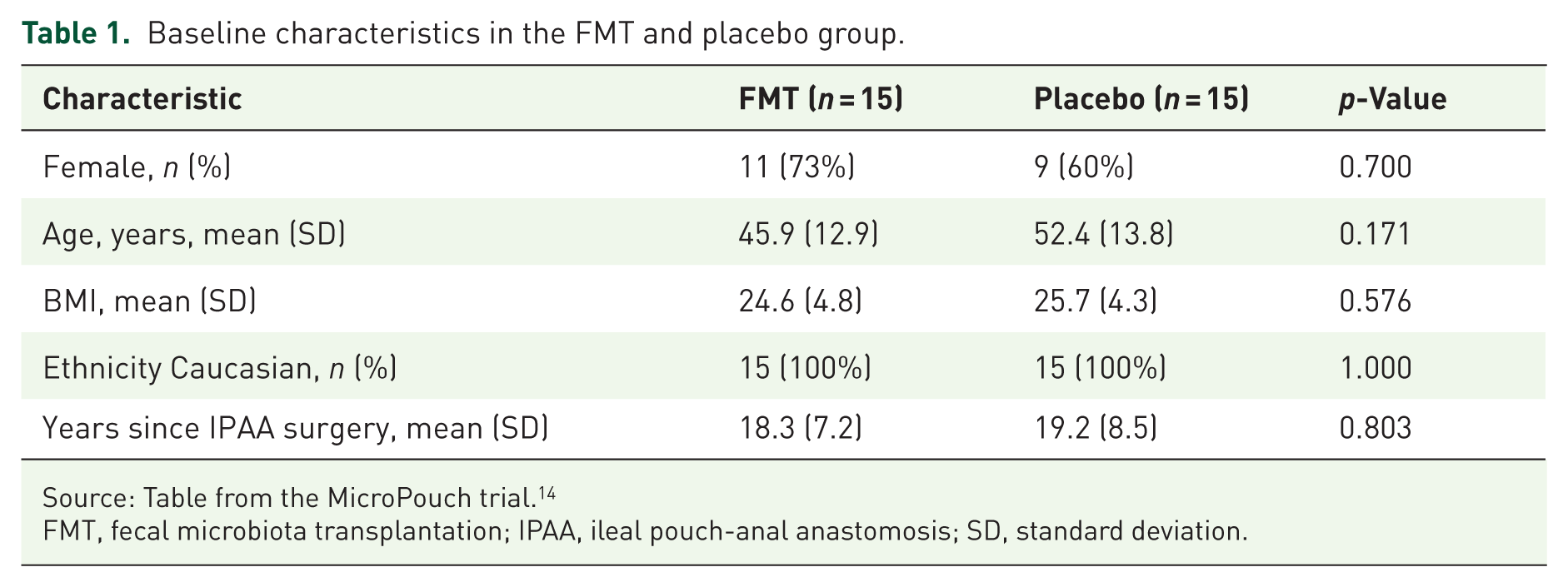
Source: Table from the MicroPouch trial. 14
FMT, fecal microbiota transplantation; IPAA, ileal pouch-anal anastomosis; SD, standard deviation.
Data from the 11 patients in the open-label FMT group were analyzed separately using linear regression analysis. PDAI scores were compared both within and between groups using linear regression analysis with adjustment for baseline PDAI. All analyses were performed using STATA® version 18 (StataCorp, Texas, USA). A p-value p ⩽ 0.05 was considered statistically significant.
Results
Thirty patients were included and randomized equally to FMT or placebo. The two groups were comparable at inclusion with no significant differences in gender, age, BMI, ethnicity, or years since IPAA surgery (see Table 1). 14 Twenty-six patients answered the QoL questionnaires at the 30-day follow-up and went pouchoscopy performed. Ten patients answered the QoL questionnaires at the 6-month follow-up, and seven patients returned the questionnaires at the 12-month follow-up.
QoL questionnaires
Regarding SIBDQ QoL (Figure 2), both groups had comparable baseline scores (Table 2). By day 30 (n = 26), patients in the placebo group showed higher SIBDQ means than those in the FMT group (p < 0.01; Table 2). Within-group analysis revealed improvement in the placebo arm (p < 0.01) and a decline in the FMT arm (p = 0.03; Table 3). These differences were no longer significant at 6 (n = 10, p = 0.55) or 12 months (n = 7, p = 0.44), though follow-up data were limited.
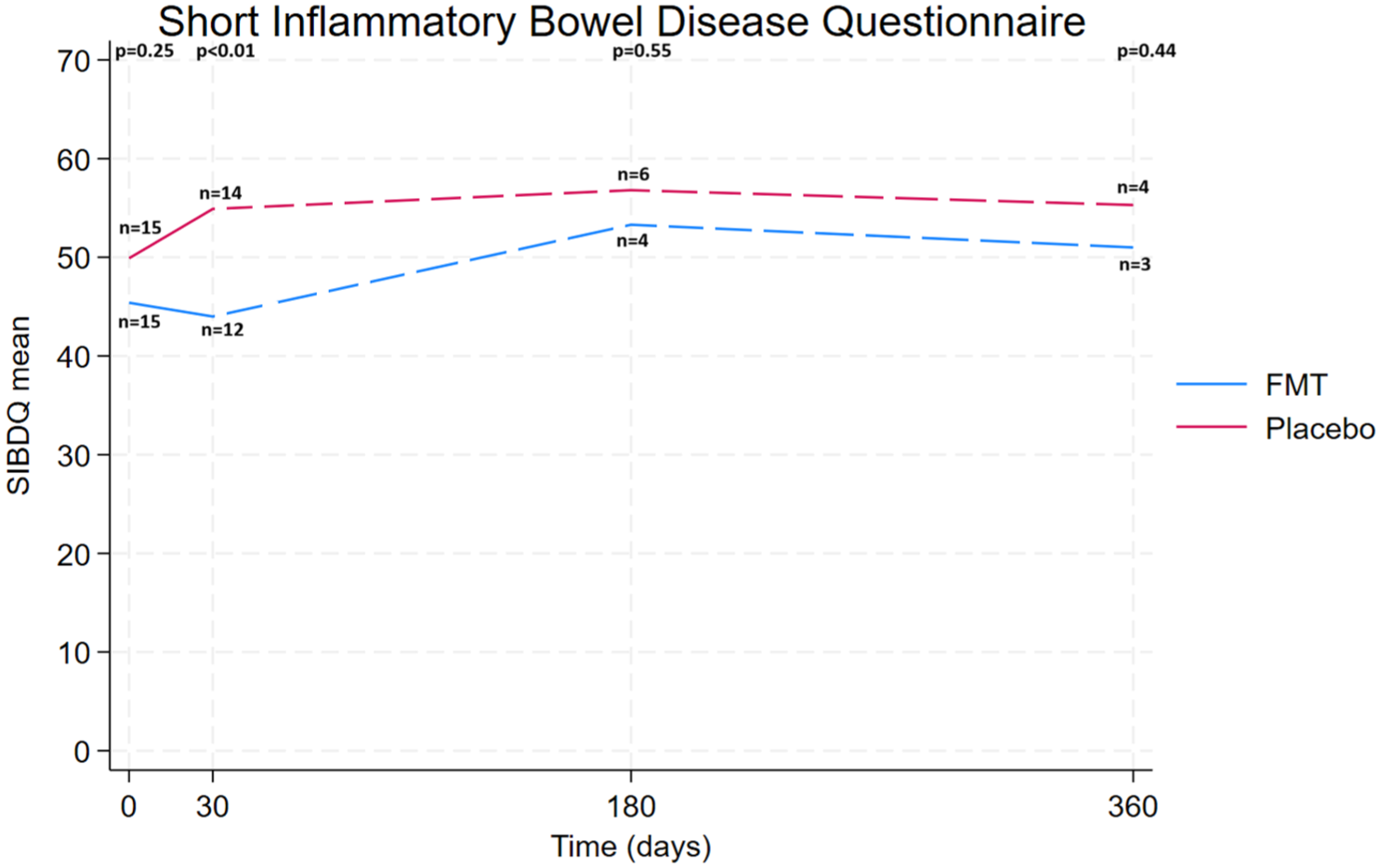
Mean scores for Short Inflammatory Bowel Disease Questionnaire for FMT and placebo over time (0 = inclusion, 30 = day 30, 180 = 6-month, and 360 = 12-month). p-Values represent between-group differences at each timepoint.
Baseline and 30-day follow-up questionnaire means: comparison between FMT and placebo.
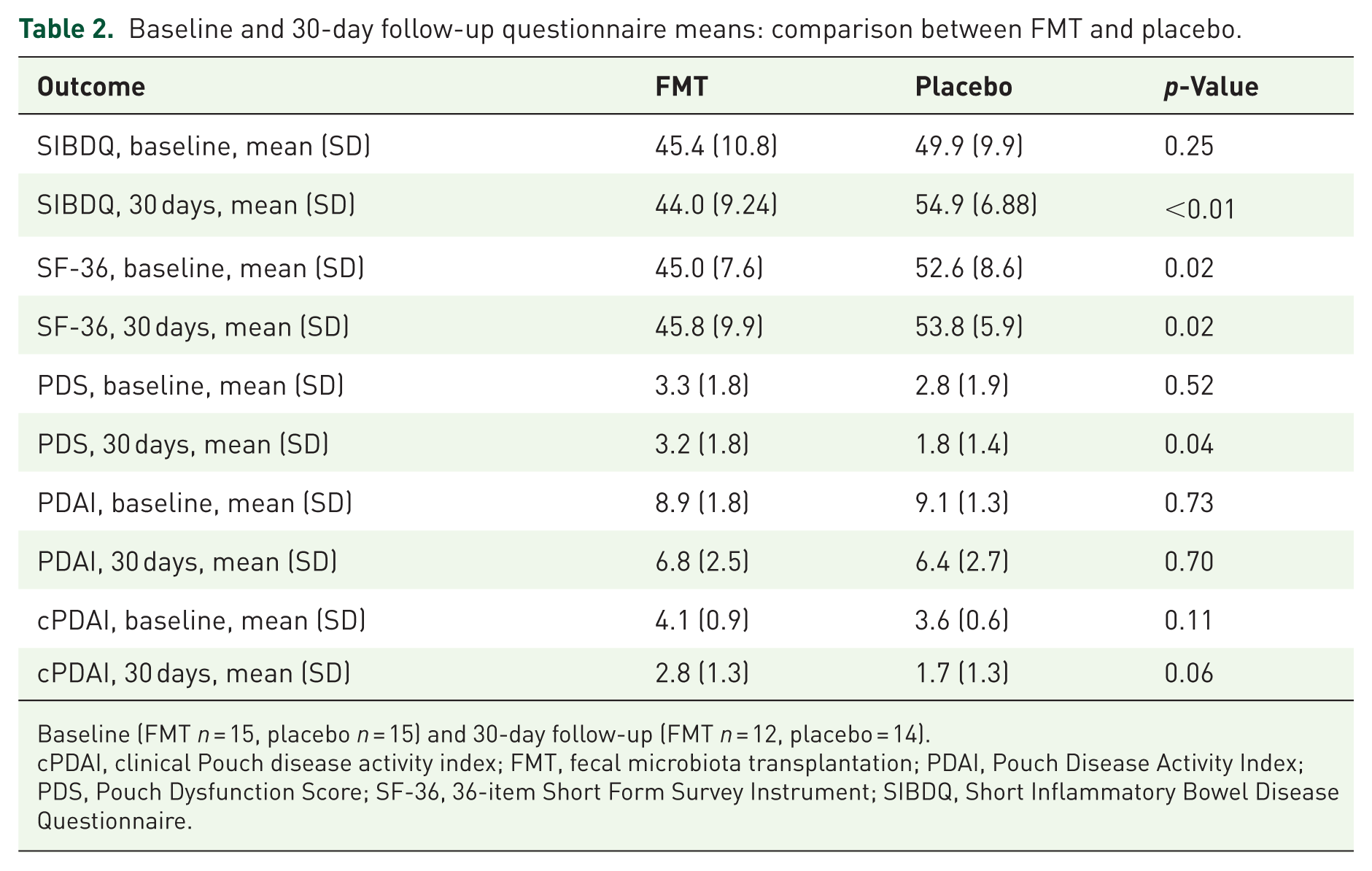
Baseline (FMT n = 15, placebo n = 15) and 30-day follow-up (FMT n = 12, placebo = 14).
cPDAI, clinical Pouch disease activity index; FMT, fecal microbiota transplantation; PDAI, Pouch Disease Activity Index; PDS, Pouch Dysfunction Score; SF-36, 36-item Short Form Survey Instrument; SIBDQ, Short Inflammatory Bowel Disease Questionnaire.
Baseline and 30-day follow-up questionnaires adjusted mean differences controlled for baseline: within-group comparison for FMT and placebo.
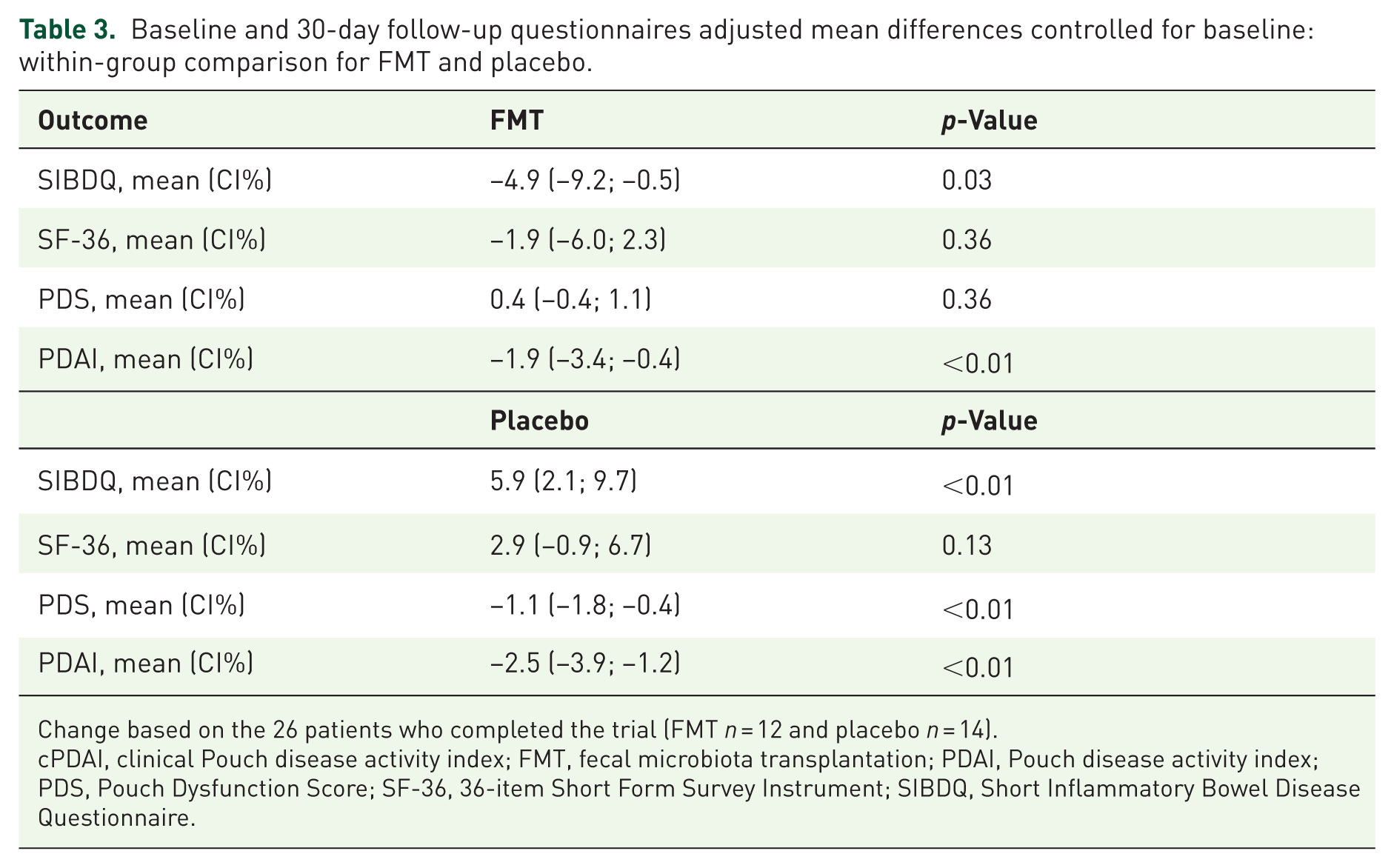
Change based on the 26 patients who completed the trial (FMT n = 12 and placebo n = 14).
cPDAI, clinical Pouch disease activity index; FMT, fecal microbiota transplantation; PDAI, Pouch disease activity index; PDS, Pouch Dysfunction Score; SF-36, 36-item Short Form Survey Instrument; SIBDQ, Short Inflammatory Bowel Disease Questionnaire.
For the PDS (Figure 3), no difference was seen at baseline between the groups (Table 2). At day 30 (n = 26), the placebo group reported fewer symptoms compared to the FMT group (mean 1.8 vs 3.2; p = 0.04; Table 2). Within-group, placebo scores improved significantly at day 30 (n = 14, p < 0.01), but no significant changes were found for the FMT group (n = 12, p = 0.36; Table 3). The differences between the groups showed a trend at 6 months (n = 10, p = 0.06), although no change was observed at 12 months (n = 7, p = 0.35).

Mean scores for Pouch Dysfunction Score for FMT and placebo over time (0 = inclusion, 30 = day 30, 180 = 6-month, and 360 = 12-month). p-Values represent between-group differences at each timepoint.
In the generic SF-36 questionnaire (Figure 4), placebo scores exceeded those of FMT both at baseline and at day 30 (n = 26, p = 0.02; Table 2). Neither group demonstrated significant within-group changes across any follow-up points (Table 3).

Mean scores for the 36-item Short Form Survey for FMT and placebo over time (0 = inclusion, 30 = day 30, 180 = 6-month, and 360 = 12-month). p-Values represent between-group differences at each timepoint.
Clinical indices mirrored these results. Both groups showed significant improvement in PDAI from baseline to day 30 (n = 26, p < 0.01, and p < 0.01, respectively), but without a between-group difference (Tables 2 and 3). For cPDAI, no baseline difference was detected, yet a non-significant trend favored the placebo group at day 30 (n = 26, p = 0.06; Table 2).
Correlations
The results are exploratory and based on the 30 answers at baseline and 26 at the 30-day follow-up. At baseline, moderate correlations between QoL scores and PDAI were observed, although with substantial variability. In the FMT group, inverse correlations were seen for SF-36 (r = −0.478), SIBDQ (r = −0.242), and PDS (r = −0.215), whereas the placebo group showed weaker or positive correlations. The difference in correlations was statistically significant for both SF-36 (p = 0.023) and SIBDQ (p = 0.049), but not PDS (p = 0.461).
At 30-day follow-up, inverse correlations between QoL scores and PDAI were again observed in the FMT group (SF-36: r = −0.539; SIBDQ: r = −0.524; PDS: r = 0.166), while correlations in the placebo group remained weak. However, these associations did not reach statistical significance, and differences between groups were not statistically significant.
Adverse events
Adverse events occurred more frequently among FMT-treated patients (80% vs 60%; p = 0.02). 14 The number of adverse events did not correlate with SIBDQ or PDS means (p = 0.36 and p = 0.69), while a trend toward lower SF-36 scores with more events was observed in the FMT group (p = 0.07). Adverse events were reported during the treatment period, including abdominal pain, fatigue, discomfort, diarrhea, fever, feeling bloated, and nausea. 14 No adverse events were reported during the follow-up period. All were mild and self-limiting. No serious adverse events were reported during the trial.
QoL and clinical assessment in FMT open-label
In the open-label FMT phase (n = 11), no significant change in QoL scores (SIBDQ, SF-36, or PDS) was found from baseline to day 30 (Table 4). The cPDAI score (Figure 5), however, declined significantly at day 30 (n = 11, p < 0.01) and remained lower at 1- and 3-month follow-ups (both n = 11 and p = 0.01; Table 4).
Open-label FMT treatment.
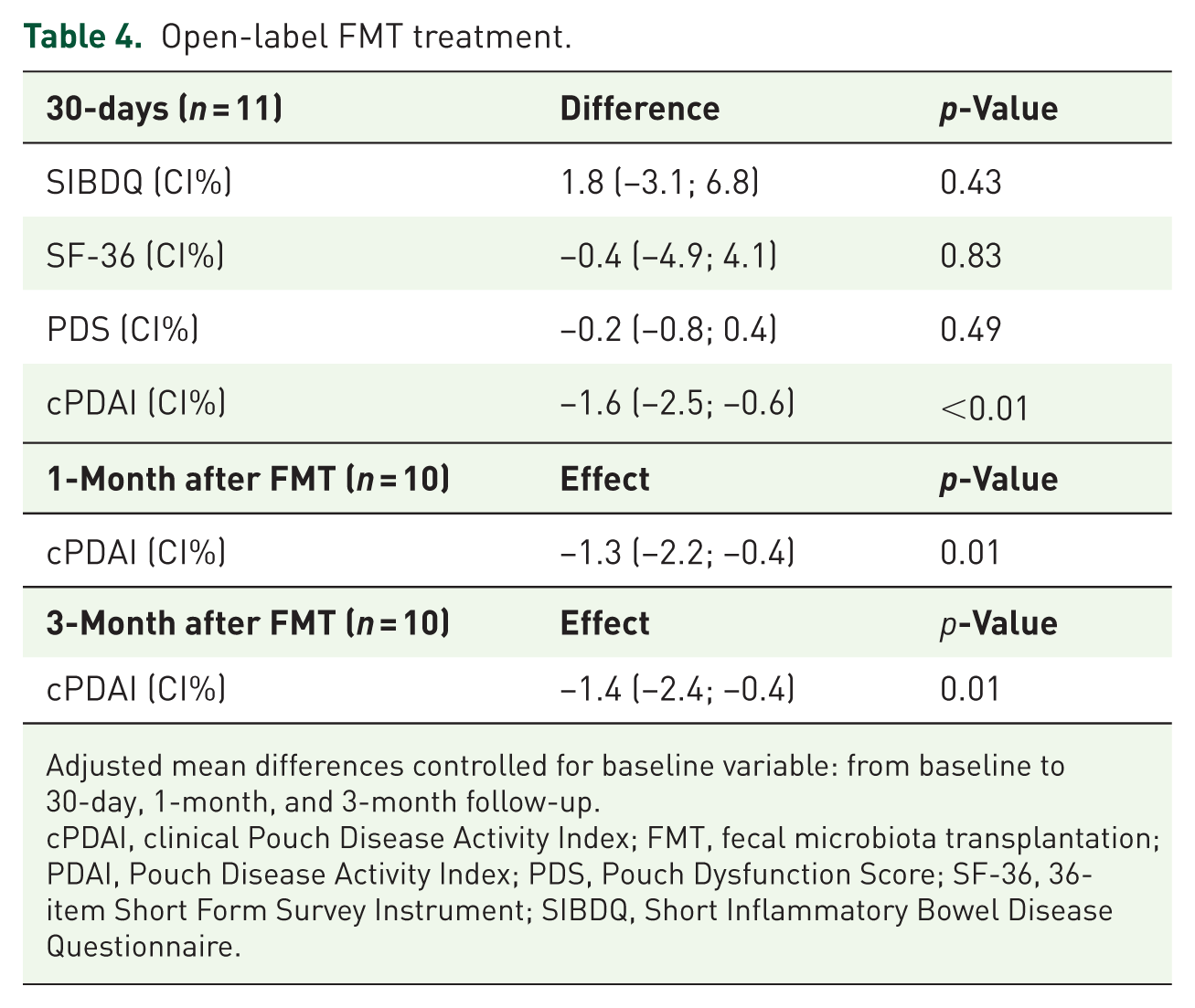
Adjusted mean differences controlled for baseline variable: from baseline to 30-day, 1-month, and 3-month follow-up.
cPDAI, clinical Pouch Disease Activity Index; FMT, fecal microbiota transplantation; PDAI, Pouch Disease Activity Index; PDS, Pouch Dysfunction Score; SF-36, 36-item Short Form Survey Instrument; SIBDQ, Short Inflammatory Bowel Disease Questionnaire.

Mean score over time (day 30, 1 month, and 3 months) for the clinical PDAI for n = 11 open-label patients.
Discussion
At day 30, patients with chronic pouchitis treated with FMT showed no improvement—and in some measures, a decline—in QoL, whereas placebo recipients improved on SIBDQ and PDS. However, it should be noted that the FMT group had lower baseline scores on both SIBDQ and PDS (Figures 2 and 3). Although these differences were not statistically significant, they raise the question of whether the apparent worsening reflects a true clinical decline or a baseline imbalance. During longer follow-up, QoL did not differ from baseline; however, only approximately 25% of questionnaires were returned at 6 and 12 months (n = 10 and n = 7), limiting inference. SF-36 did not change within either group despite a higher adverse-event burden in the FMT arm. In the open-label cohort (n = 11), QoL scores (SIBDQ, PDS, SF-36) showed no significant change from baseline to day 30, while clinical disease activity improved: cPDAI decreased at day 30 and remained lower at 1 and 3 months. Moderate inverse correlations were observed between QoL scores (SF-36 and SIBDQ) and PDAI in the FMT group at baseline; however, these associations were not statistically significant at the 30-day follow-up and should be interpreted with caution given the small sample size.
Patients with chronic pouchitis experience substantial disruption of their daily lives and must adapt their routines to manage persistent symptoms. In a recent qualitative study by Barnes et al., 33 semi-structured interviews with patients who had undergone IPAA surgery for UC and later developed pouchitis revealed increased concern about incontinence, higher stool frequency, and greater pain during flare episodes. These findings mirror the symptoms reported by patients in the present study. Notably, the FMT group reported more abdominal cramping, higher stool frequency, and greater fatigue. Despite these symptom differences, neither group showed changes in overall health-related QoL (SF-36), although disease-specific measures (SIBDQ and PDS) indicated more severe symptoms in the FMT group. Because patients with pouchitis already live with a considerable symptom burden and reduced baseline QoL, 33 short-term fluctuations, whether due to FMT or placebo, are unlikely to meaningfully alter their perception of overall health-related QoL. Baseline SF-36 scores were significantly lower in the FMT group despite randomization, whereas no other parameters differed between groups. This imbalance complicates the interpretation of SF-36 outcomes, as the groups may not have been fully comparable.
Validated questionnaires offer a standardized and quantifiable method to assess how a disease affects patients’ daily lives. Their utility, however, depends on a clear understanding of patient experience and on validation within the relevant population. Although several studies have applied various tools to evaluate pouchitis after IPAA surgery, no pouchitis-specific QoL instrument is currently available. 34 Focus groups conducted by Barnes et al. 33 identified frequency of bowel movements, urgency, and incontinence as the symptoms most critical to patients. To capture these domains, we selected two symptom-specific instruments: the SIBDQ, validated for UC patients, and the PDS, validated for UC patients who have undergone IPAA. Both assess these key symptoms and their impact on daily and social functioning.28,29 In this study, FMT was associated with no improvement—and at times a transient decline—in QoL, whereas the placebo group showed modest improvement, likely reflecting a placebo effect.
The FMT group had a significantly lower QoL SIBDQ score at day 30 than at baseline. Because the SIBDQ focuses on symptoms experienced over the preceding 14 days, this short-term decrease may be related to a higher frequency of treatment-related adverse events. All adverse events were mild and disease symptom-related. The transient disease flares are likely FMT-related, resulting in a temporary worsening of QoL. The effect had disappeared by the 6- and 12-month follow-ups, suggesting no lasting effect of FMT on QoL. To assess broader health-related QoL, we applied the SF-36 questionnaire, 20 which showed no significant change in either group. As noted by Koerdt et al., 35 disease-specific tools may be more sensitive to clinical change than general instruments. This likely explains why the SF-36 failed to detect group differences, highlighting the greater sensitivity of SIBDQ and PDS in this patient population. The placebo group showed significant improvement in both SIBDQ and PDS scores at day 30. This likely reflects a placebo response. Symptom severity in chronic pouchitis may fluctuate over time, and part of the improvement may therefore reflect the natural course of the disease. In addition, expectancy effects may influence patient-reported outcomes such as QoL, as patients’ perception of symptom relief can be affected by participation in a clinical trial. Regression to the mean is also a likely contributor, as patients were included during periods of active disease, and extreme baseline values tend to move toward the average at follow-up.
FMT is already a recommended treatment for rCDI in several European countries. Studies have shown that a single FMT procedure can successfully induce clinical remission and improve QoL in patients with rCDI.23,36 Although no disease-specific questionnaire has yet been developed for rCDI, the Short Health Scale questionnaire, validated in IBD patients, and the generic EuroQoL 5-Dimensions 3- and 5-Levels questionnaires have been applied. FMT has been shown to increase health-related QoL after treatment compared with baseline and to be superior to antibiotics in preventing recurrence.23,36 In general, few studies have examined the impact of FMT on QoL in patients with chronic pouchitis. Nonetheless, QoL remains an essential outcome when evaluating the overall effectiveness of treatment. The few studies addressing this aspect have used different questionnaire instruments and reported inconsistent results. Landy et al. 25 evaluated QoL using the Cleveland Global Quality of Life (CGQoL) score following nasogastric FMT treatment and found no significant difference between baseline and 4 weeks after treatment. By contrast, the RCT by Karjalainen et al., 22 which used the generic 15D health-related QoL questionnaire, administered FMT via flexible endoscopy and transanal catheter. Although FMT did not achieve clinical remission in that study, patients in the FMT group demonstrated a significantly improved QoL 26 weeks after treatment compared with baseline. Supporting this, Fang et al. 37 presented a case report describing improved QoL after FMT administered by flexible sigmoidoscopy, assessed using the SIBDQ and CGQoL instruments. The patients with chronic pouchitis reported higher QoL and fewer symptoms 3 months after treatment. Overall, our study aligns most closely with the findings of Landy et al. 25 as no sustained improvement in QoL was observed. On the contrary, according to the SIBDQ results, patients even experience a temporary decline in QoL following FMT treatment.
The open-label FMT phase in our study demonstrated a significant reduction in cPDAI, which persisted up to the 3-month follow-up. This finding is consistent with the results reported by Karjalainen et al. 22 and Fang et al. 37 The open-label phase included 11 patients undergoing unblinded FMT using the same treatment regimen as applied in the RCT FMT. Given the small sample size, the results lack sufficient statistical power to support final conclusions. Furthermore, no significant difference was observed in QoL scores between baseline and day 30 after treatment. Only the self-reported cPDAI score showed a significant reduction, whereas endoscopic and histological inflammation were not assessed. The unblinded design further increases the risk of bias. In addition, differences in follow-up intervals between the RCT FMT and open-label phases complicate direct comparison of the outcomes.
A potential explanation for the lack of QoL improvement may lie in donor-recipient compatibility. Previous studies suggest that both donor- and recipient-specific factors influence FMT efficacy, and that optimal characteristics in both are required to achieve the best outcome. Unfortunately, these determinants have not yet been clearly identified. 38 Another possible explanation concerns the route of administration. A systematic review concluded that both the method of delivery and the number of administrations significantly affect the clinical response to FMT. Lower gastrointestinal endoscopy was deemed superior to both enemas and upper gastrointestinal endoscopy. Although repeated administrations enhance the effect of FMT,26,39 this approach may still have reduced clinical efficacy, particularly if patients were unable to retain the infusion for the recommended 30 min, as outlined in the European guidelines. 26 An alternative approach is dual-route administration, which may enhance the efficacy of FMT. Previous studies have combined initial delivery via colonoscopy with subsequent administration using oral capsules. This strategy has been shown to be safe and may represent a potential treatment approach in patients with UC, 40 and therefore could possibly have enhanced the potential effect of FMT in this study as well. Sterile water with food coloring was administered in this study as a placebo. Some trials have used autologous FMT as a placebo, as it introduces the known bacterial complex and is considered a safe approach in IBD trials. 41 It was not chosen here, as it potentially could have biological effects by reintroducing the patient’s own microbiota, and therefore would not serve as an inert control.
As mentioned above, no pouchitis-specific questionnaire currently exists to evaluate QoL. 34 The use of generic or disease-related instruments validated for other conditions, such as UC, may therefore have limited the patients’ ability to report subtle or condition-specific changes in symptoms. Consequently, true treatment effects could have been obscured if the questionnaires failed to capture all relevant aspects of living with pouchitis.
Our study has several limitations. A substantial proportion of questionnaires were missing at the 6- and 12-month follow-ups in both the FMT and placebo groups, posing a significant limitation. This low response rate limits the ability to draw definitive conclusions at these time points, although trends have been discussed above. Despite active follow-up by study nurses and physicians, some questionnaires remained incomplete. Another limitation is potential response bias among participants who completed the study; patients with greater energy and resources may have been more likely to return questionnaires, thereby introducing bias. Reasons for missing data were not consistently documented, although some patients discontinued participation due to relapse and the need for antibiotics.
The small sample size further limits the statistical power of the study and increases the risk of type II errors, which may have obscured real differences between the groups. Moreover, the main QoL analyses are based on short-term follow-up due to few responses, restricting the interpretation of long-term effects. The open-label phase was unblinded, which may have introduced expectancy bias in self-reported outcomes. Another limitation is the absence of microbiological or inflammatory data, which could have clarified the relationship between microbial changes and QoL.
Finally, the choice of questionnaires may have affected sensitivity to change. Of the three instruments used, only the PDS is validated specifically for pouch patients. The other two are considered appropriate but may be overly generic or emphasize domains less relevant to pouchitis, potentially limiting the detection of subtle, condition-specific changes in patients’ daily functioning. Despite these limitations, the study contributes valuable insight into the complex relationship between FMT and QoL in patients with chronic pouchitis and highlights the need for larger, long-term studies using pouchitis-specific outcome measures.
Conclusion
Treatment with FMT did not improve QoL scores compared with placebo. On the contrary, patients with chronic pouchitis who received FMT experienced a higher burden of symptoms in the short term. Taken together, these findings suggest that FMT may not be a beneficial therapeutic approach for improving QoL in this patient population. However, given the small sample size, limited follow-up, and lack of pouchitis-specific outcome measures, the long-term effects and potential benefits in selected patient subgroups remain uncertain and warrant further investigation.
Footnotes
Acknowledgements
None.
Authors’ note
Conference presentation: European Society of Coloproctology (ESCP) 2025, Paris, France. Oral presentation.
Declarations
Generative artificial intelligence
During the preparations of this work, ChatGPT was used to assist with language polishing and sentence refinement.