
Abstract
Background:
Laparoscopic appendectomy (LA) is the conventional treatment for chronic appendicitis. Endoscopic direct-vision appendicitis therapy (EDAT) has emerged as a minimally invasive, organ-preserving alternative.
Objectives:
To compare the efficacy and safety of EDAT versus LA in chronic appendicitis.
Design:
Multicenter retrospective cohort study with propensity score matching (PSM).
Methods:
This multicenter retrospective cohort study was conducted in China between January 2019 and February 2024. PSM was performed to minimize selection bias. A total of 186 patients with chronic appendicitis were included, including 63 who received EDAT and 123 who underwent LA. The primary outcome was the clinical success rate. The secondary outcomes included the technical success rate, duration of hospitalization, adverse event rate, and recurrence rate.
Results:
Compared with LA, EDAT showed comparable clinical success (95.2% vs 100%, p = 0.068) and technical success rates (96.8% vs 98.4%, p = 0.877). EDAT reduced the duration of hospitalization (median 2 vs 3 days, p < 0.001) and short- and long-term overall adverse event rates (6.4% vs 45.5% and 7.9% vs 21.1%, respectively; p < 0.001, p = 0.022). At 6, 24, and 48 h postoperatively, the EDAT group had a greater proportion of patients with no pain or mild pain than the LA group did (68.3% vs 40.7% and 90.5% vs 66.7% and 98.4% vs 74.8%, respectively; all p < 0.001). After the 1-year follow-up, the calculated recurrence rate did not differ between the groups (4.8% vs 0%, p = 0.068).
Conclusion:
Compared with LA, EDAT is a safe, effective, organ-preserving alternative technique for chronic appendicitis, offering a shorter recovery time, reduced adverse event rates, and a low recurrence rate observed during follow-up.
Plain language summary
Chronic appendicitis causes long-term abdominal pain and is typically treated by surgery removing the appendix. While effective, surgery requires incisions, carries risks and involves a longer recovery. We used the digital cholangioscope originally designed for bile duct exams. The cholangioscope was advanced into the appendix lumen through its orifice, allowing doctors to directly visualize the interior, diagnose the problem, and perform targeted treatments. Our results show this technique is safe and feasible for managing chronic appendicitis. It successfully treated patients without any surgical cuts.This research offers a potential new alternative to surgery, leading to less pain, quicker recovery, and no scars.
Keywords
Introduction
Chronic appendicitis is clinically characterized by recurrent or persistent right lower abdominal pain. Although its pathogenesis remains incompletely elucidated, it is often attributed to persistent luminal obstruction, commonly by fecaliths, leading to sustained inflammation. This chronic inflammatory state can result in histopathological changes such as fibrous obliteration of the appendiceal lumen, reactive lymphoid hyperplasia, and lymphocytic infiltration.1,2 The condition tends to recur, with symptoms reappearing over months or even years, contributing to diagnostic delay and patient discomfort. While computed tomography (CT) may reveal findings suggestive of chronic appendicitis, such as appendiceal thickening (>6 mm), appendicoliths, or increased density of periappendiceal fat, these features are not specific to chronic appendicitis and may be absent in confirmed cases. 1
Laparoscopic appendectomy (LA) is the conventional treatment for appendicitis; however, it is associated with potential postoperative adverse events, such as bowel obstruction and loss of appendiceal immune function.3–6 In recent years, endoscopic retrograde appendicitis therapy (ERAT) has emerged as a pioneering, minimally invasive treatment that preserves the appendix while achieving therapeutic efficacy.7–9 Endoscopic direct-vision appendicitis therapy (EDAT), which was first reported in 2012 for the treatment of acute uncomplicated appendicitis,10,11 utilizes a combination of colonoscopy and appendicography, with parallel treatment such as irrigation, fecalith extraction, and stent drainage.12,13 However, this technique requires X-ray guidance and cannot directly observe the appendiceal lumen, leading to limitations, including radiation-induced injury, intubation failure, and the inability to make an accurate diagnosis.12–14
With advances in choledochoscopic technology, which was initially developed for treating bile duct stones and strictures, EDAT was introduced by integrating a colonoscope with a digital single-operator cholangioscope.15,16 This visual technique allows for the real-time visualization of the appendiceal lumen and endoscopic treatment with preservation of the appendix by using a cholangioscope. In 2025, our department reported the efficacy and safety of EDAT with those of LA in treating patients with acute appendicitis, demonstrating a reduction in operative time, postoperative function recovery time, and pain. 17 Notably, no studies have compared the outcomes of EDAT with those of LA in the treatment of chronic appendicitis. Therefore, we conducted a retrospective cohort study to assess the technical success rate, curative success rate, short- and long-term adverse event rates, and recurrence rates within 1 year of EDAT and compare these rates with those of LA.
Methods
Study design
This quality research project was designed as a retrospective observational study. The reporting of this study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 18
Patient selection
This multicenter retrospective study included clinical data from 1155 patients with chronic appendicitis who were treated at three hospitals in China between January 2019 and February 2024. The study cohort included 882 patients from Zhongda Hospital, Southeast University, 185 patients from Liangjiang Hospital, Southeast University, and 88 patients from the Affiliated Changshu Hospital of Nantong University. This study was approved by the ethics committee of Zhongda Hospital, Southeast University (approval no. 2024ZDSYLL042-P01). All study procedures adhered to the Declaration of Helsinki. The ethics committee waived the requirement for obtaining informed consent from the patients owing to the retrospective nature of the study.
Patients were enrolled if they met all of the following criteria: (1) underwent either EDAT or LA; (2) reported experiencing chronic abdominal pain (recurrent or persistent) for ⩾3 months, and had undergone adequate diagnostic evaluation to rule out alternative causes (such as functional gastrointestinal disorders, inflammatory bowel disease) with symptoms persisting despite conservative management; (3) had CT findings indicating an appendicolith or thickening of the appendix but without features of acute appendicitis such as periappendiceal exudate; and (4) had an EDAT intraoperative endoscopic presentation consistent with chronic appendicitis or pathologically confirmed chronic appendicitis after LA.
Patients were excluded if they met any of the following criteria: (1) had clinical or radiographic evidence of acute appendicitis; (2) had an appendiceal perforation or abscess; (3) had CT findings suggestive of appendiceal stenosis; (4) had a suspected appendiceal tumor; (4) had an acute disease such as cholecystitis, pancreatitis, and urinary stones; (5) had a serious underlying disease (American Society of Anesthesiologists class III–IV); (6) had incomplete clinical data; or (7) had incomplete follow-up data.
The included patients were divided into EDAT and LA groups on the basis of their treatment strategies for chronic appendicitis. Variables such as sex, age, body mass index (BMI), and underlying disease status were matched between the two groups using the propensity score matching (PSM) method (1:2) to determine the final number of patients enrolled.
Methodology
Data collection
Data related to patient characteristics, procedures, postoperative adverse events, and follow-up were collected from hospital medical records, endoscopic photographs, and videos.
Procedure
Main instruments
An Olympus CF-HQ290I therapeutic colonscope (Olympus, Tokyo, Japan), an Olympus transparent cap (D-201-11804), a digital single-operator cholangioscope (eyeMax; Microtech, Nanjing, China), a zebra guide wire (Boston Scientific, Marlborough, MA, USA), and a pancreatic duct plastic stent (Microtech, Nanjing, China) were used.
Anesthetic management and safety measures
All EDAT procedures were performed under conscious sedation in a fully equipped endoscopic center with standard monitoring and resuscitation capabilities, performed by experienced endoscopists and anesthesiologists. Before the procedure, patients were thoroughly informed of potential risks. In the event of an uncontrolled complication (e.g., perforation and significant bleeding), the patient would be immediately transferred to the operating room for emergency laparoscopic surgery by the standby surgical team.
Main steps
EDAT group: All patients underwent standardized bowel preparation preoperatively. After successful conscious sedation, the disposable eyeMax imaging system was used during EDAT to treat chronic appendicitis through the following steps: (1) The colonoscope was equipped with a transparent cap to advance to the cecum without looping and observe the appendiceal orifice. (2) A digital cholangioscope was inserted into the appendiceal lumen through the appendiceal orifice. If insertion was difficult, a zebra guidewire was first inserted, and the digital cholangioscope was guided into the appendix. (3) After the appendix was entered, continuous irrigation with water was performed to observe the appendiceal cavity. (4) The appendiceal lumen was flushed with saline solution or ornidazole. In the case of purulent secretions or debits, thorough lavage was performed. For a stone obstruction, a mesh basket was used to remove the stone; for a narrow appendiceal lumen, balloon dilation was performed. In the case of a large amount of pus, a 7–8.5 Fr plastic stent (usually 7 cm in length) was inserted under the guidance of the zebra guidewire to maintain drainage. (5) Upon reaching the distal appendiceal lumen, the scope was slowly withdrawn under continuous irrigation to ensure complete clearance. The appendiceal lumen was re-examined to confirm adequate flushing. (6) For patients for whom an appendiceal stent was placed, a follow-up ultrasound was performed 1–2 weeks after EDAT to confirm the stent position. If necessary, the stent was subsequently removed under colonoscopy (Figure 1). During the EDAT procedure, mucosal biopsies were not routinely obtained. In cases, findings suggestive of malignancy (e.g., mass lesions or irregular mucosal growth) were encountered, a biopsy would be performed.

EDAT therapy procedure. (a) A colonoscope was inserted into the cecum for observation of the appendiceal orifice. (b) A digital cholangioscope was inserted into the appendiceal lumen through the appendiceal orifice. (c) If insertion was difficult, a zebra guidewire was first inserted, and digital cholangioscopy was guided into the appendix. (d) Continuous irrigation with water was performed to observe the appendiceal cavity. (e, f) A 7 Fr plastic stent was inserted under the guidance of the zebra guidewire.
LA group: All surgeries were performed by LA. The specimens were removed through the umbilical orifice. All the removed specimens were sent for histopathological analysis after surgery.
Postprocedural management
All patients were given antibiotics for ⩽48 h postoperatively. Postoperative pain was managed conservatively, with no supplemental analgesic medications administered to patients in either group. After their abdominal pain was relieved, the patients started a liquid diet, which was subsequently increased as tolerated. The discharge criteria included the following: (1) complete relief of abdominal pain and (2) normalization of inflammatory markers (white blood cell count and C-reactive protein (CRP) level). The patients were closely monitored for abdominal pain, hemorrhage, perforation, fever, and other adverse events after EDAT and LA. The patients were examined with abdominal radiography or CT, if necessary.
Follow-up
All patients received telephone or outpatient follow-up at 1, 6, and 12 months postoperatively, with regular review of abdominal ultrasound or CT scans annually and timely follow-up in case of any discomfort.
Definitions of terms
In this study, the technical success of EDAT was defined as successful completion of the procedure described in Figure 1, and that of LA was defined as successful appendectomy without conversion to open appendectomy. Clinical success was defined as no recurrence of appendicitis during the 1-year follow-up period in both the EDAT group and the LA group. Intubation failure was defined as unsuccessful insertion of the cholangioscope into the appendiceal lumen. Appendicolith extraction failure was defined as the inability to remove appendicoliths from the appendiceal lumen. An appendiceal stricture was defined as failure to advance the cholangioscope through the appendiceal lumen because of narrowing. The visual analog scale (VAS) score (ranging from 0 to 10 points) was used to assess abdominal pain intensity, with scores categorized as follows: 0 (no pain), 0.1–3.0 (mild pain); 3.1–7.0 (moderate pain); 7.1–9.9 (severe pain); and 10 (unbearable pain). 11 The patients selected a number from 0 to 10 to indicate their pain level, which was recorded by the nurse on the postoperative day. For patients with multiple pain scores, the highest score was selected. Recurrence was defined as the reappearance of symptoms suggestive of chronic appendicitis (e.g., right lower quadrant abdominal pain), supported by corresponding imaging findings on abdominal ultrasound or CT, such as appendiceal thickening (>6 mm), or the presence of appendicoliths.
Outcome assessment
The primary outcome was the clinical success rate. The secondary outcomes included the technical success rate, duration of hospitalization, short- and long-term adverse event rates, and recurrence rate.
Propensity score matching
The PSM method was used to reduce the bias caused by the nonrandom selection of patients, and the optimal pairing method of matching at a 1:2 ratio was used, with matching variables including age, sex, BMI, and underlying disease status. The propensity scores were calculated using logistic regression and 1:2 nearest neighbor matching (caliper = 0.05) using the R software (version 4.3.1, Vienna, Austria). p Values for all the confounding variables were above 0.05 for both groups, implying satisfactory equilibrium. The matched cohorts comprised 63 and 123 patients in the EDAT and LA groups, respectively.
Statistical analysis
SPSS (version 27.0; IBM, Armonk, NY, USA) software was used for the statistical analyses. Normally distributed continuous variables are presented as the means ± standard deviations and were analyzed using independent samples t-tests for comparisons between two groups. Nonnormally distributed quantitative data are expressed as medians (interquartile ranges) and were compared using the Mann–Whitney U test. Categorical variables are expressed as frequencies (%) and were compared between groups using the Pearson χ2 test, corrected χ2 test, or Fisher’s exact probability method. p < 0.05 was considered to indicate statistical significance.
Results
Patient characteristics
Figure 2 presents the patient selection flowchart for this study. We initially assessed 1155 patients with suspected chronic appendicitis treated at Zhongda Hospital, Southeast University, between January 2019 and May 2024. A total of 823 patients (65 in the EDAT group, 758 in the LA group) were ultimately eligible after the following patients were excluded: patients with appendiceal perforations or abscesses (n = 28), patients with CT findings suggestive of appendiceal stenosis (n = 52), patients with suspected appendix tumors (n = 12), patients with acute diseases such as cholecystitis, pancreatitis, and urinary stones (n = 49), patients with other serious underlying diseases (n = 50), patients with incomplete clinical data (n = 76), and patients lacking follow-up data (n = 65). After PSM, the final cohort consisted of 186 matched patients: 63 in the EDAT group and 123 in the LA group. As demonstrated in Table 1, the baseline characteristics of the matched patients were well balanced after PSM, with no statistically significant differences observed (all p > 0.05).

Flow diagram of patient selection.
Baseline characteristics of the patients.

EDAT, endoscopic direct-vision appendicitis therapy; IQR, interquartile ranges; LA, laparoscopic appendectomy; PSM, propensity score matching.
Table 2 summarizes the pretreatment symptoms and auxiliary examination characteristics of the patients after PSM. Patients in the EDAT group exhibited a shorter median duration of chronic appendicitis than those in the LA group did (13 (8.0–21.5) vs 24 (10.5–39.5) months, respectively; p = 0.003). The intensity of abdominal pain differed between the groups: patients in the EDAT group predominantly reported mild abdominal pain (69.8%), whereas moderate abdominal pain was more common in the LA group (49.6%). In terms of preoperative inflammatory indicators, the proportion of patients with CRP levels >5 mg/L was greater in the LA group than in the EDAT group, although there was no difference in the leukocyte count between the two groups (p = 0.101). The abdominal CT imaging findings in both groups were dominated by appendicoliths, with no difference observed between the two groups (p = 0.607).
Characteristics of pretreatment symptoms and auxiliary examinations of patients after PSM.

CRP, C-reactive protein; CT, computed tomography; EDAT, endoscopic direct-vision appendicitis therapy; IQR, interquartile ranges; LA, laparoscopic appendectomy; NA, not applicable; PSM, propensity score matching; VAS, visual analog scale.
EDAT characteristics
In the EDAT group, the cholangioscopy findings included appendicoliths (95.2%), congestion and swelling of the appendix lumen (52.4%), narrowing of the appendix lumen (7.9%), and food residue (6.3%; Figure 3). Therapeutic interventions were based on cholangioscopy findings, with some patients requiring multiple interventions, including stent placement for drainage, which was performed in 34.9% of the patients; simple lavage, which was performed in 69.8% of the patients; basket extraction, which was performed in 25.4% of the patients; and stricture dilation, which was performed in 7.9% of the patients (Figure 3 and Table 3).

EDAT intraoperative findings and interventions. (a) A massive amount of pus was discovered during saline irrigation. (b) One appendicolith was identified in the appendiceal lumen. (c) Appendicoliths were extracted by a mesh basket under direct visualization via digital cholangioscopy. (d) The mucosa of the appendix was found to be congested and edematous. (e) For patients with appendiceal lumen stenosis, a controlled radial expansion balloon was employed to dilate the narrowed segment. (f) Food residue was observed in the lumen of the appendix, after which a 7 Fr plastic stent was placed in the appendiceal lumen to maintain drainage.
EDAT characteristics and outcomes (N = 63).

EDAT, endoscopic direct-vision appendicitis therapy.
Intraoperative and postoperative outcomes
EDAT was successfully performed in 61 patients (96.8%), with a success rate comparable to that of LA (98.4%; p = 0.877). Two patients for whom EDAT failed underwent LA: one due to unsuccessful intubation caused by severe appendiceal stenosis and the other due to incomplete appendicolith removal. The median duration of hospitalization was longer in the LA group than in the EDAT group (3 (2–4) vs 2 (2–3) days, respectively; p < 0.001). There was no statistically significant difference in medical costs between the two groups (p = 0.192). At 6, 24, and 48 h postoperatively, the EDAT group had a significantly greater proportion of patients with no pain or mild pain than the LA group did (all p < 0.001; Table 4).
Comparison of outcomes and follow-up between the groups after PSM.
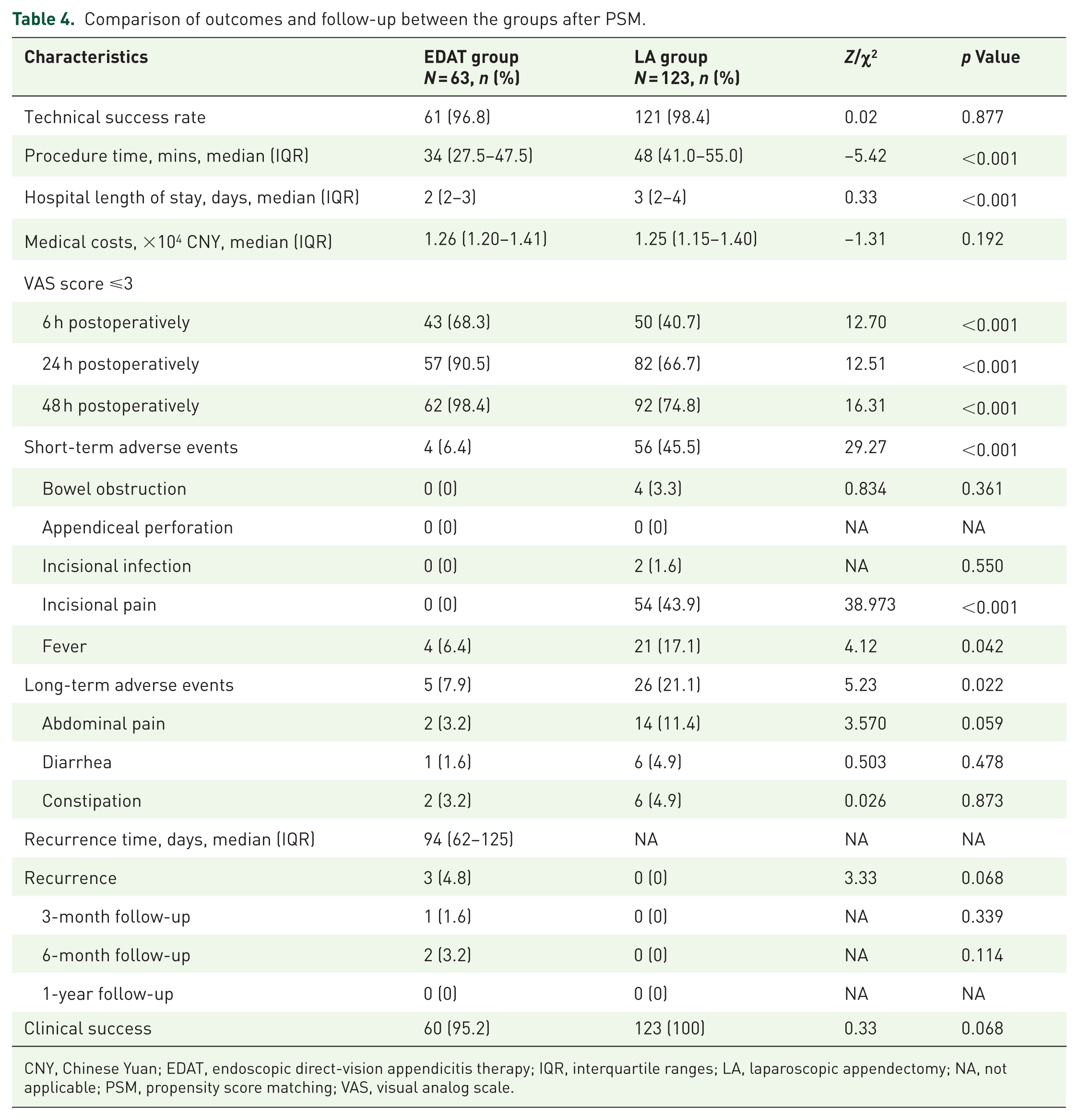
CNY, Chinese Yuan; EDAT, endoscopic direct-vision appendicitis therapy; IQR, interquartile ranges; LA, laparoscopic appendectomy; NA, not applicable; PSM, propensity score matching; VAS, visual analog scale.
In terms of postoperative complications, both short- and long-term overall adverse event rates were lower in the EDAT group than in the LA group (6.4% vs 45.5% and 7.9% vs 21.1%, respectively; p < 0.001, p = 0.022). In the EDAT group, four (6.3%) patients had fever, which was considerably lower than the number of patients in the LA group (21 (17.1%) patients; p = 0.042). Short-term complications in the LA group included bowel obstruction (3.3%), incisional infection (1.6%), and incisional pain (43.9%). There were no differences in the incidence of long-term chronic abdominal pain, diarrhea, or constipation between the two groups (all p > 0.05; Table 4).
Recurrence after EDAT at the 1-year follow-up
Table 4 and Figure 4 illustrate the recurrence rates of chronic appendicitis in the EDAT group. Among the 63 patients in the EDAT group, 3 experienced recurrence, resulting in a calculated recurrence rate of 4.8%. Among the patients who experienced recurrence, one patient experienced recurrence within 3 months, and two patients experienced recurrence within 6 months post-EDAT. The median recurrence time was 94 (62–125) days. The management of recurrence included LA in two patients (with postoperative pathology confirming chronic appendicitis) and repeat EDAT in one patient, who was followed for up to 1 year without further recurrence. The clinical success rate did not significantly differ between the two groups (95.2% vs 100%, p = 0.068).

Kaplan–Meier graph of the time to chronic appendicitis recurrence after EDAT during follow-up.
Discussion
This study reported a novel endoscopic technique for the management of chronic appendicitis, which has been performed in our center. To our knowledge, this is the first cohort study comparing EDAT and LA for treating chronic appendicitis using PSM. Our study demonstrated that EDAT achieved technical and clinical success comparable to LA, while also providing more rapid abdominal pain relief, reducing both short- and long-term adverse event rates, and maintaining a low recurrence rate during follow-up.
The symptoms of chronic appendicitis-associated abdominal pain are atypical and are mainly located in the right lower abdomen. A few patients present with pain in atypical locations, including periumbilical, pelvic, or total abdominal pain, which can last for months or even years. Appendicoliths are considered the etiological factor of appendicitis-associated abdominal pain. 19 Chronic appendicitis needs to be considered on the basis of a combination of medical history, imaging findings, and exclusionary diagnosis. This diagnostic ambiguity frequently leads to misdiagnosis, and patients are often initially misdiagnosed with functional dyspepsia, chronic pelvic pain, or irritable bowel syndrome in clinical practice. During recurrent episodes, many patients may undergo prolonged and ineffective treatment, such as repeated antibiotic therapy or acid suppression therapy. The treatment of abdominal pain associated with chronic appendicitis includes antibiotics and LA. However, patients who receive antibiotic therapy are prone to recurrence, and LA is associated with complications such as incisional infections, bowel obstruction, and potential loss of immune function.
In recent years, appendicoscopy using a single-operator cholangioscope has gained increasing attention as a minimally invasive technique for the treatment of appendicitis and preservation of appendiceal function.15–20 In this study, we further extended this technique to chronic appendicitis and named it EDAT. The results revealed that EDAT shortened the duration of hospitalization and reduced short- and long-term adverse event rates. Our findings corroborate those of previous studies on acute appendicitis.15,20 Kong et al. 21 reported that when direct colonoscopy imaging and cholangioscopy were used for acute appendicitis treatment, the technical success rate reached 100% without recurrence during 2–24 months of follow-up. Another multicenter retrospective study highlighted the advantages of ERAT over antibiotic therapy, including faster pain relief, shorter hospital stays, and lower recurrence rates. 20
Previous studies indicate that the overall complication rate of endoscopic appendicitis therapy ranges from approximately 0% to 9.8%,11,20,22–24 which is significantly lower than that of LA. Commonly reported complications include postoperative fever (1.6%–2.6%), appendiceal perforation (0.5%–1.3%), and chronic abdominal pain (0%–6.6%).11,20,22,23 Most of these complications can be managed endoscopically or conservatively. The incidence of serious complications (e.g., infection, conversion to surgery) is below 2%. In the present study, the short- and long-term adverse event rates in the EDAT group (6.4% and 7.9%, respectively) were consistent with the ranges reported in the literature, further supporting the safety of this technique within well-defined indications.
In this study, we calculated VAS scores for postoperative abdominal pain in both groups. We found that patients in the EDAT group achieved rapid relief of postoperative abdominal pain, which was attributed to immediate lumen decompression and avoidance of surgical trauma. The vast majority of appendicoliths can be successfully flushed under direct choledochoscopic visualization, with only a small percentage requiring removal using a mesh basket. Our previous study reported a case of complex multiple appendicoliths managed using the EDAT technique. During extraction, a mesh basket was entrapped because of luminal stenosis, and a controlled radial expansion balloon was subsequently deployed to dilate the narrowed segment. Finally, subsequent calculus extraction was performed using a balloon-anchored traction. 25
Notably, the diagnosis of chronic appendicitis remains challenging due to the nonspecific nature of its clinical presentation and the limitations of conventional imaging such as CT. In this study, appendicoscopy identified appendiceal stenosis in five patients, which was not visualized by CT. This result suggests that conventional imaging may be insufficient for diagnosing chronic appendicitis, which is consistent with the findings of a previous study. 22 With the help of EDAT, we could directly visualize the appendiceal lumen and provide precise diagnoses and treatment of mucosal congestion, edema, fecaliths, and appendiceal stenosis in patients with suspected abdominal pain associated with chronic appendicitis. Interestingly, we observed differential inflammatory patterns between the two groups. The LA group had a significantly higher proportion of elevated CRP levels compared to the EDAT group, suggesting that patients selected for LA may have had a more inflammatory phenotype. This finding supports that inflammatory markers may provide valuable clues for differentiating appendicitis subtypes. Although the retrospective nature of this study limited our ability to fully explore the diagnostic value of inflammatory markers, their observed heterogeneity hints at potential utility in stratifying chronic appendicitis subtypes, particularly in identifying obstructive or more inflammatory phenotypes.
During the follow-up period, the recurrence rate in the EDAT group was 4.8%, with all recurrence cases further confirmed through either postoperative pathology or direct endoscopic visualization. All three patients with recurrence exhibited appendiceal stenosis, indicating that luminal stricture might impair proper drainage and predispose to recurrent fecalith obstruction, consequently triggering recurrent abdominal pain. This suggests that appendiceal stenosis might be a risk factor for the poor therapeutic outcomes of EDAT. These findings highlight the importance of EDAT as a therapeutic tool and a valuable diagnostic tool for risk stratification. Noninvasive appendicitis treatment can also be used as a secondary or even multiple treatments for patients with recurrent chronic appendicitis and contraindications to surgery.
On the basis of our practical experience, we summarize the advantages of EDAT: (1) Direct endoscopic visualization technology improves the efficacy and safety of appendiceal treatment. Under endoscopic guidance, clinicians can clearly observe appendiceal luminal contents (feces, purulent secretions), mucosal inflammation, and structural abnormalities (tortuosity, dilatation, or stenosis) and thus make more accurate diagnoses. (2) EDAT avoids the risk of radiation exposure to both physicians and patients, improves safety for patients allergic to contrast media, and reduces the risk of peritonitis due to contrast extravasation in cases of perforated appendicitis. Furthermore, EDAT has a short learning cycle and is easy for young physicians to perform, making it easy to promote in the clinic. In clinical practice, EDAT is particularly suitable for patients desiring organ preservation or with surgical contraindications, especially in special populations such as children, pregnant women, and elderly patients with comorbidities. This approach should be considered in cases of uncomplicated chronic appendicitis, as it serves both diagnostic and therapeutic purposes. Decision-making should involve a multidisciplinary team to integrate patient preferences, imaging findings, and clinical status for individualized treatment planning.
Limitations
This study has several limitations. First, its retrospective design inherently introduces potential selection bias. Second, we lacked data on potential confounding factors such as patients’ diet, lifestyle, and genetic characteristics, which may influence the development and course of appendicitis. Furthermore, the diagnostic criteria for chronic appendicitis remain unstandardized, and some enrolled patients may have had other conditions with similar clinical presentations. Future research should include larger sample sizes, longer follow-up periods, and incorporate comprehensive biomarker, dietary, and genetic data in multicenter prospective studies.
Conclusion
In conclusion, EDAT was demonstrated to be a safe and effective minimally invasive technique for treating chronic appendicitis, with faster recovery, fewer adverse events, and a low recurrence rate observed during follow-up. In addition, EDAT eliminates the need for X-ray equipment, thus broadening the population of recipients, including infants, young children, adolescents, and pregnant women.