
Abstract
Background:
Non-variceal gastrointestinal bleeding (NVGIB) is a critical situation and needs immediate resuscitation therapy. Hemostatic powder (HP) is an effective way to achieve hemostasis.
Objectives:
This study compares the outcomes of HP and conventional therapies (CT) for NVGIB patients.
Design:
Systematic review and meta-analysis of randomized controlled trials (RCTs).
Data sources and methods:
We searched PubMed, Scopus, and other medical databases up to August 2024. This meta-analysis includes studies that reported data on rebleeding, hemostasis, and hospital stays. Using a random-effect model, we analyzed the odds ratios (OR) of the outcomes between the HP and CT groups.
Results:
Nine RCTs meeting the inclusion criteria were included in this study, comprising data from 796 patients. HP demonstrated a statistically significant advantage in achieving hemostasis compared to CT, with an OR of 2.73 (95% confidence interval (CI): 1.09–6.80; p = 0.03). However, no significant differences (p > 0.05) were observed in rebleeding rates (OR: 0.73; 95% CI: 0.36–1.47) or length of hospital stay (mean difference: 1.38 days; 95% CI: −1.18 to 3.93). Secondary outcomes, including mortality, surgical intervention requirements, blood transfusion needs, intensive care unit admissions, transfusion units, and procedure time, also showed no significant disparities between groups. Subgroup analyses based on bleeding etiology revealed enhanced efficacy of HP in cases of tumor-related bleeding.
Conclusion:
Both HP and CT effectively manage NVGIB with similar rebleeding rates, but HP demonstrates superior immediate hemostasis, offering a critical advantage in acute bleeding control.
Meta-analysis registration:
This systematic review and meta-analysis was registered at PROSPERO (https://www.crd.york.ac.uk/PROSPERO/) with registration number CRD42024523237.
Plain language summary
Non-variceal gastrointestinal bleeding (NVGIB) is a serious condition that requires quick treatment. This study compared hemostatic powder (HP) with conventional therapies (CT) to see which is more effective. Analyzing data from nine studies with 796 patients, the results showed that HP is better at achieving quick hemostasis, significantly improving bleeding control. However, both treatments had similar outcomes regarding rebleeding rates and hospital stays. Overall, while HP offers a crucial advantage in stopping acute bleeding, both HP and CT are effective for managing NVGIB.
Keywords
Introduction
Gastrointestinal bleeding (GIB) is a critical medical condition that poses a high risk of morbidity and mortality.1,2 Non-variceal gastrointestinal bleeding (NVGIB) continues to be an important medical problem leading to morbidity and mortality, especially in elderly patients, and more than 20,000 deaths are reported every year.3,4 Over time, experts have devised multiple therapeutic strategies to find the most efficient technique for achieving hemostasis. However, the probability of successful intervention is influenced by a multitude of factors, including lesion topography, pathophysiological characteristics, patient comorbidities, and operator proficiency. Multiple endoscopic accessories are available for performing hemostasis, including forceps, clips, injection needles, endoscopic stitching, banding devices, electrocoagulation probes, and hemostatic powders (HPs).5,6 Endoscopists often encounter challenges when dealing with the site of the bleeding, the size of the affected blood vessel, and the possibility of complications. 7 Technical factors such as the complex anatomical location of hemorrhagic foci and the heterogeneity of bleeding patterns, ranging from focal to diffuse, significantly impact the efficacy of various therapeutic interventions.7–10
Recently, there has been a significant increase in the utilization of inorganic HP such as Hemospray (Cook Medical, Winston Salem, NC, USA) or TC-325, particularly in the management of GIB encompassing non-variceal and malignant bleeding lesions. Its ability to coat extensive regions without requiring direct contact with the target tissue through spraying onto the lesion has made this more effective and easier to use. Studies have shown a higher rate of initial hemostasis (>90%) and a lower rate of rebleeding (<15%) using the HP.11–13 The recent American College of Gastroenterology guidelines also supported using HP for NVGIB. 14 But on the other hand, the European Society of Gastrointestinal Endoscopy supports its use for refractory GIB. 1 The Asia-Pacific working group suggests using HP as an effective treatment for temporarily managing bleeding in NVGIB when definitive hemostasis cannot be established. 15
Several meta-analyses have also been published to evaluate better treatment procedures for GIB, 16 but there is still a paucity of information about using HP.8,17–20 Recently published randomized controlled trials (RCTs) have shown that HP is as effective as conventional therapy (CT) with similar adverse events. 8 This study compared the efficacy of HP to the CT for NVGIB, including tumor and peptic ulcer GIB or both.
Materials and methods
Guidelines for Preferred Reporting Items in Systematic Reviews and Meta-Analyses were followed in conducting this study. 21 This systematic review and meta-analysis was registered at PROSPERO with registration number CRD42024523237.
Search strategy
Medical databases, including PubMed, Web of Science, Embase, and Scopus, were searched. We used the following terms and combinations in the search: “gastrointestinal hemorrhage,” “gastrointestinal bleeding,” “hemostatic powder,” “hemospray,” and TC-325. We completed the investigation on August 25, 2024. Two authors selected the relevant studies and discussed and resolved any issues that emerged.
Studies selection
We used the following criteria to determine which studies to include and which to exclude.
Inclusion criteria
(1) Studies comparing the efficacy of HP and CT for NVGIB (both upper and lower).
(2) Only RCTs were included.
(3) Studies conducted only in patients with NVGIB.
(4) Studies on adult patients aged >18 years.
(5) Only human studies published in English.
Exclusion criteria
(1) Letters, reviews, cohort studies, retrospective studies (observational studies), abstracts, single-arm studies, and case reports were not included.
(2) Single-arm studies reporting only HP or CT treatments.
(3) Studies reporting patients with variceal bleeding.
(4) Studies missing the primary outcomes or inadequate results.
(5) Studies on patients aged less than 18 years.
(6) Animal research and studies in another language.
Data extraction
Two researchers (H.K. and Y.Y.T.) extracted data from the selected research studies. Two researchers extracted the following details from each study: publication year, country, study design, total patients, mean age, sex proportion, number of patients in HP or CT, etiology, forest types, rebleeding, hemostasis, procedure time, hospital stay, intensive care unit (ICU) admission, surgery need, mortality, blood transfusion need, and units of blood transfusion. The studies were divided into two subgroups: the HP and CT groups.
Outcome and definitions
The primary outcomes were rebleeding (defined as a significant drop in hemoglobin level (>2 g/dL), the presence of fresh bleeding signs like hematemesis, melena, or hematochezia, hemodynamic instability, or endoscopic evidence of ongoing bleeding after initial endoscopic treatment). Secondary outcomes include hemostasis, defined as endoscope-confirmed bleeding stopping for 3–5 min. It may also refer to bleeding control within 30 days of randomization. Hemostasis during the initial endoscopy and prevention of bleeding later. Mean procedure time (defined as the time taken for the treatment procedures), hospital stay (defined as the length of hospital stay after the endoscopic treatment), ICU admission (defined as patients who need to be admitted to the ICU due to poor health conditions), need for surgery (defined as the number of patients who failed endoscopic hemostasis and need surgery), mortality (defined as death due to any cause after randomization), and need for blood transfusion (defined as the number of patients who need blood transfusion due to a low hemoglobin level). Subgroup analyses were performed on the basis of bleeding (GI tumor bleeding, peptic ulcer bleeding, or both).
Quality assessment of studies
The revised Cochrane risk-of-bias tool for randomized trials (RoB2) evaluation method was used in this study. 22 The assessment assigned a “low” score when there was a minimal risk of bias, a “high” grade when there was a significant risk of bias, and a “some concerns” grade when the available evidence was insufficient to determine the risk of bias. During the study analysis, several factors were considered, such as the absence of outcome data, the promptness of participant identification or recruitment, the measurement of the outcome, variations from the intended treatments, and the selection of the reported outcomes.
Publication bias and study effect
A funnel plot was utilized to assess the probability of publication bias in this meta-analysis. To identify the impact of each study on the overall outcome, a systematic process was employed whereby each study was individually eliminated. 23
Statistical analysis
This study utilized the Review Manager software (version 5.4.1, The Cochrane Collaboration, 2020) to calculate odds ratios (ORs) for the outcomes. We calculated the OR and 95% confidence intervals (95% CI) for each outcome using a random-effect model, following the Mantel–Haenszel technique. We calculated the mean difference using the continuous inverse variance approach with a random-effect model. We measured the statistical heterogeneity using Cochrane χ2 and I2 statistics. The degree of heterogeneity was determined by considering the following criteria: if the values fall between 30% and 60% (moderate), 50% and 90% (substantial), and 75% and 100% (considerable). 24 For the data to be considered statistically significant, the p-value should be below 0.05.
Results
Search results and characteristics of included studies
We retrieved 592 articles through various database searches and other means. Finally, this meta-analysis included a total of nine RCT studies25–33 (Figure 1). These 9 studies comprised 796 patients, with 393 patients in the HP group and 403 in the CT group. There was no significant difference in the basic characteristics of the patients, and the studies included 547 male and 249 female patients. The etiology of most of the studies involved patients with bleeding from gastric or duodenal ulcers,25,26,31 as well as bleeding from gastrointestinal malignancies28,30,32 or both and others.27,29,33 Some other etiologies included patients with post-sphincterotomy bleeding, Mallory–Weiss syndrome, Dieulafoy lesions, esophagitis, esophageal erosion, gastritis, gastric amyloidosis, post-endoscopic submucosal dissection (ESD) or post-endoscopic mucosal resection bleeding, and diffuse hemorrhage from erosive gastritis.

PRISMA flow diagram of study selection.
The studies included in this meta-analysis consisted of two carried out in Brazil27,30 and Korea31,33 and one conducted in each of the following countries: Singapore, 25 Canada, 28 Hong Kong, 29 Thailand, 32 and Iran. 26 Patients with ulcers showing high-risk stigmata of bleeding (Forrest classes IA, IB, IIA, and IIB) or bleeding caused by malignancies were included in these studies. All studies employed HP, with seven using TC-325, one utilizing a polysaccharide hemostatic powder (PHP) 31 (a similar mechanism to TC-325 but comprising different components), and another study using CEGP-003 33 (a mixture of hydroxy-ethyl-cellulose and epidermal growth factor). Most studies used 9–20 g of HP. Only one study used a maximum of 150 g of HP after nonresponse at 20 g of HP. The CT therapy included many procedures such as endoscopic hemoclips, bipolar electrocautery, argon plasma coagulation, electrical coagulation, saline adrenaline injections, epinephrine injection, heater probes, and laser photocoagulation. In one study, a combination of epinephrine injection and TC-325 was administered, while HP was used as monotherapy in all the other trials.
Further characteristics of the included studies are shown in tables (Tables 1 and 2). No study with a high risk of bias was found. Four studies had some concerns regarding bias, while the remaining studies had a low risk of bias (Supplemental Material risk of bias outcomes). Because this meta-analysis included fewer than 10 studies, the possibility of publication bias was eliminated. No study showed a statistically significant impact on the final results.
Basic characteristics of included studies.
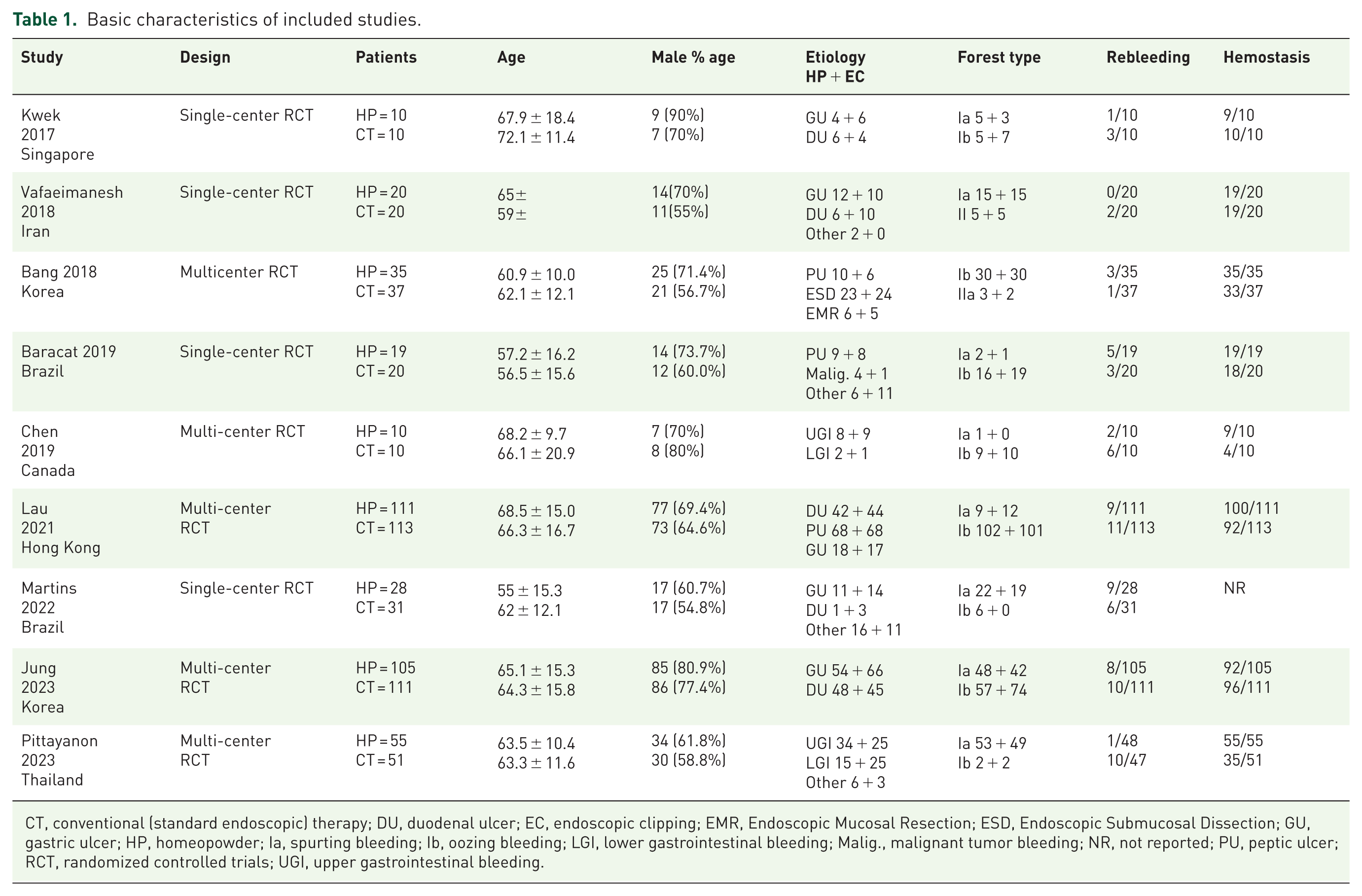
CT, conventional (standard endoscopic) therapy; DU, duodenal ulcer; EC, endoscopic clipping; EMR, Endoscopic Mucosal Resection; ESD, Endoscopic Submucosal Dissection; GU, gastric ulcer; HP, homeopowder; Ia, spurting bleeding; Ib, oozing bleeding; LGI, lower gastrointestinal bleeding; Malig., malignant tumor bleeding; NR, not reported; PU, peptic ulcer; RCT, randomized controlled trials; UGI, upper gastrointestinal bleeding.
Characteristics of included studies.
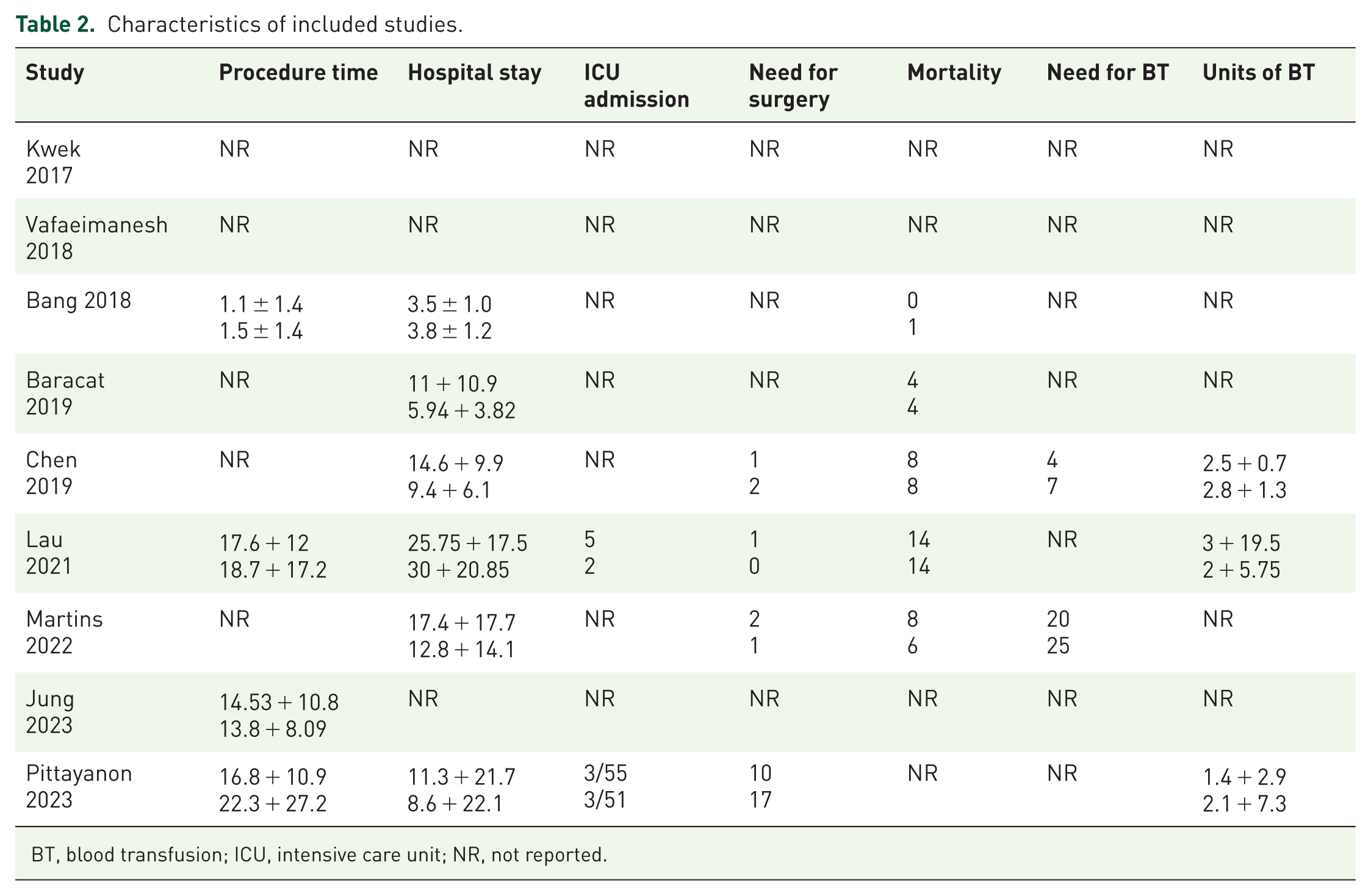
BT, blood transfusion; ICU, intensive care unit; NR, not reported.
Rebleeding
All nine trials included in the analysis reported data on the rebleeding. There was no statistically significant difference in the OR (0.73, 95% CI: 0.36–1.47; I2 = 43%; p = 0.37) of rebleeding incidents between the two groups (Figure 2).

Forest plot of bleeding.
Hemostasis
We used data from the eight studies to calculate the OR for hemostasis. The OR for achieving immediate hemostasis through HP compared with the CT was 2.73 (95% CI: 1.09–6.80; I2 = 48%, p = 0.03), indicating a statistically significant difference with moderate heterogeneity in the result (Figure 3(a)).

(a) Forest plot of hemostasis. (b) Forest plot of hospital stay.
Hospital stay
The mean difference in length of hospital stay was 1.38 days (95% CI: −1.18 to 3.93; I2 = 42%, p = 0.29), and did not show any significant difference with moderate heterogeneity (Figure 3(b)).
Mortality
Five studies recorded patient deaths during the study period. There was no statistically significant difference between the two groups, as the OR for mortality was 1.11 (95% CI: 0.62–1.97; I2 = 0%; p = 0.73; Figure 4(a)).
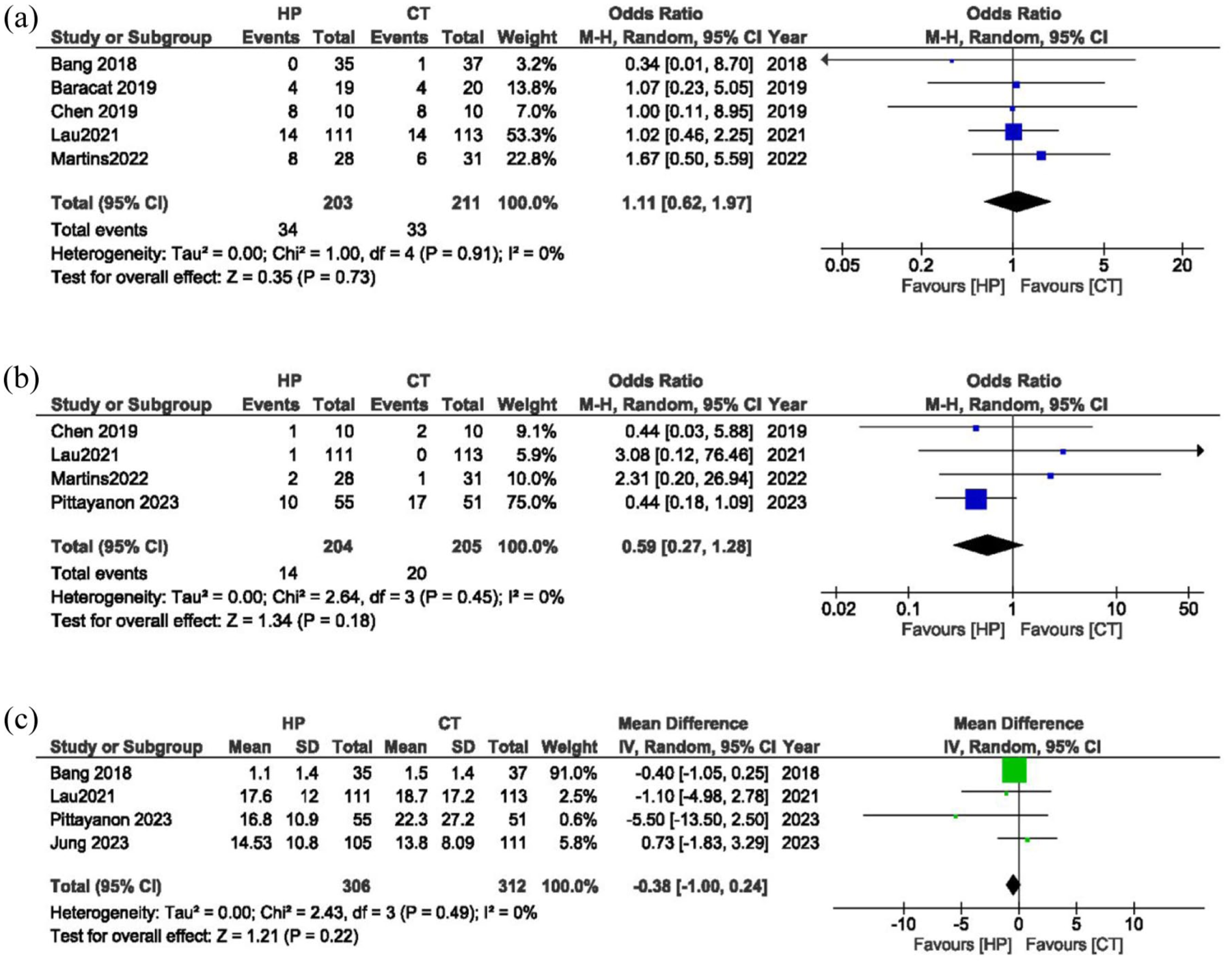
(a) Forest plot of mortality. (b) Forest plot of need for surgery. (c) Forest plot of procedure time.
Need of surgery
Reports on patient data regarding the need for surgery treatments showed an OR of 0.59 (95% CI: 0.27–1.28; I2 = 0%; p = 0.18), indicating no significant difference between the two groups (Figure 4(b)).
Procedure time
The endoscopic procedure time showed no significant difference between the HP and CT groups, with a mean difference of −0.38 min (95% CI: −1.00 to 0.24; I2 = 0%; p = 0.22; Figure 4(c)).
ICU admission
Only two studies provided data on the admission of patients with NVGIB to the ICU following endoscopic therapy. The OR of 1.55 (95% CI: 0.48–4.80; I2 = 0%; p = 0.46) showed no significant difference between the two groups (Supplemental Figure 1(a)).
Need for blood transfusion
The OR for the requirement for a blood transfusion was 0.48 (95% CI: 0.17–1.32; I2 = 0%; p = 0.16), indicating no difference between the HP and CT groups (Supplemental Figure 1(b)).
Unit of blood transfusion
The mean blood transfusion unit did not show a significant difference between the two groups, with a mean difference of −0.30 units (95% CI: −1.12–0.52; I2 = 0%; p = 0.48; Supplemental Figure 1(c)).
Subgroup analyses
Subgroup analyses based on bleeding etiology revealed the following findings: (Figures 1 and 2).
Peptic ulcer bleeding (three studies)
No significant differences were observed between the HP and CT groups in rebleeding rates (OR: 0.64, 95% CI: 0.27–1.52; I2 = 0%, p = 0.31) or hemostasis rates (OR: 1.03, 95% CI: 0.49–2.17; I2 = 0%, p = 0.94).
GI tumor bleeding (three studies)
The HP group indicated a statistically significant difference in immediate hemostasis rates (OR: 23.72, 95% CI: 2.75–150; p = 0.0008; I2 = 0%). The rates of rebleeding showed no significant difference between the groups (OR: 0.34, 95% CI: 0.04–2.95; p = 0.33; I2 = 78%) with significant heterogeneity. The duration of hospital stay showed a trend to be longer in the HP group (mean difference 4.28 days, 95% CI: −0.27 to 8.82; p = 0.07; I2 = 0%), while the results were not statistically significant.
Mixed NVUGIB cohorts (three studies, including peptic ulcer, GI tumor, and other etiologies)
Hemostasis rates were significantly higher with HP compared to CT (OR: 2.40, 95% CI: 1.15–5.01; I2 = 0%; p = 0.02), while rebleeding rates demonstrated no difference between groups (OR: 1.17, 95% CI: 0.55–2.48; I2 = 0%; p = 0.69). Hospital stay also showed no significant difference (mean difference 0.44 days, 95% CI: −2.70 to 3.58; I2 = 57%; p = 0.78).
Discussion
This meta-analysis of nine RCTs concluded that HP outperformed CT in the management of NVGIB. The key finding of our study is the significantly higher immediate hemostasis rate with HP, with nearly triple the odds of immediate hemostasis (OR: 2.73, p = 0.03), especially in subgroups experiencing GI tumor-related bleeding (OR: 23.72, p = 0.0008) and mixed etiologies (OR: 2.40, p = 0.02). Rebleeding rates (OR: 0.73, p = 0.37) and length of hospital stay (mean difference 1.38 days, p = 0.29) exhibited no statistically significant differences. In addition, mortality rates, the need for surgical interventions, blood transfusion requirements, procedural time, and transfusion units indicated no significant differences between the groups (p > 0.05). The subgroup study highlighted HP’s superior effectiveness in managing malignancy-associated bleeding, promoting it as the preferred initial treatment for acute bleeding management in GI tumors.
The result indicates that HP may be beneficial in situations requiring rapid hemostasis, such as malignancy-associated bleeding or diffuse mucosal lesions, where conventional endoscopic techniques encounter technical difficulties. HP’s non-contact application and capacity to cover extensive areas likely strengthen its efficacy in these scenarios. However, the absence of a significant decrease in rebleeding (OR: 0.73, p = 0.37) suggests that HP’s mechanical hemostatic effect may be temporary, necessitating supplementary therapies for lasting control. This finding is consistent with previous studies highlighting the necessity of integrating HP with definitive treatments (e.g., clips or thermal therapy) for high-risk lesions. Recently published meta-analyses have also demonstrated that the HP performs better than the CT.10,23 A meta-analysis of RCTs has provided significant evidence suggesting that HP is more effective than CT in achieving primary hemostasis (OR: 3.48, 95% CI: 1.09–11.18). Furthermore, the study found that HP and CT have similar rates of adverse events and need for surgery. 23 In addition, HP is better at achieving immediate hemostasis for treating GIB, as confirmed by two meta-analyses consisting of 19 studies and 11 studies, respectively.34,35 A recent meta-analysis of eight studies also suggested that HP monotherapy surpassed conventional endoscopic therapy (CET) in both the initial hemostasis rate and the 30-day recurrence of bleeding in patients experiencing GIB related to malignancies. 36 Our results also align with this study.
In certain situations, conventional treatment methods may not be enough to successfully treat the underlying cause of the bleeding. 5 Endoscopists are now considering HP because it can be rapidly shed from the mucosa and eliminated from the body within 24 h of application. Nevertheless, a limitation exists: in research investigations involving the use of HP, there is still a propensity for bleeding to recur.11,12 In addition, the CT technique might not stop bleeding in up to 15% of cases where peptic ulcers are actively bleeding. Following an initial successful outcome from combined endoscopic therapy, it is possible to encounter a recurrence of bleeding in approximately 5%–10% of patients.7,37 HP is an acceptable alternative for CT because it can effectively treat broader areas with indeterminate bleeding sites and can be used in difficult-to-access areas where CT is hard to perform.34,35
Pittayanon et al. 32 conducted a study involving 106 patients with gastrointestinal tumor bleeding. The data revealed that the rebleeding rate with HP (TC-325) was significantly lower compared to standard endoscopic therapy (SET) (2.1% vs 21.3%; p = 0.003). In addition, the immediate hemostasis rate was higher with HP (TC-325) compared to SET (100% vs 68.6%; p = 0.001), although other outcomes were similar between the two groups. A recently published meta-analysis of 5 studies involving 362 patients found that there were no significant differences in the risk ratios (RR) for primary hemostasis (RR 1.09), rebleeding (RR 1.13), or the standard mean difference in length of hospital stay. 8 Another meta-analysis of 20 trials concluded that HP is equally effective as CT in treating NVGIB, indicating that there is no significant difference in their efficacy. 38 But our study has found that HP is superior in achieving immediate hemostasis, especially for GI tumor-related bleeding.
Efficacy of HP for hemostasis is not only limited to NVGIB but is also effective for other GIB. A meta-analysis, consisting of 59 studies including 3417 patients with GIB, concluded that topical hemostatic treatments are equally safe and effective as CT, with similar outcomes. 39 Our comprehensive analysis of nine RCTs also revealed no significant difference in the OR of rebleeding duration of hospital stay. Another study involving 86 patients with esophagogastric variceal bleeding compared the effectiveness of HP and SET, revealing that HP is more effective than SET for achieving immediate hemostasis. 40 HP is beneficial not only in the treatment of NVGIB but also in lower GIB (LGIB), with improved outcomes and the ability to induce immediate hemostasis in most LGIB cases.11,37,41 A meta-analysis of 9 studies with 194 patients with LGIB also stated that HP is safe and effective for the treatment of LGIB. 34 Barkun et al. 5 also showed that hemospray not only improves the effectiveness of traditional hemostasis but also less costly in most NVUGIB patient populations.
Previous research has indicated that the length of hospital stay was comparable between both groups. 8 Our meta-analysis also revealed no significant difference between the HP and CT groups. Recently published studies have also shown no significant difference in hospital stay.31,32 The HP application led to faster hemostasis and earlier discharge of patients compared to the CT group. The benefit of hemospray is that it does not necessitate the employment of highly specialized abilities. It does not require precise measurement and is neither thermal nor contact-based. This allows a broader range of medical professionals, including endoscopists who are not necessarily specialists in GIB, to use it. This ability to adapt is vital in rural locations, where qualified endoscopists are rare. 35 A recent study has also shown that HP performs better in achieving immediate hemostasis than CT. 32 NVGIB is not the only condition for which HP is beneficial; it is also helpful for esophagogastric variceal bleeding. 40 However, the cost and other factors remain obstacles to utilizing HP as a regular treatment.
The subgroup analysis illustrates significant differences in the efficacy of HP against CT for NVGIB, depending on the etiology of the bleeding. This strongly supports the utilization of HP in these scenarios, particularly given the unpredictable bleeding of tumors and the potential limitations of conventional treatments. Nonetheless, the efficacy of HP in preventing rebleeding was unclear, perhaps due to the influence of variables such as tumor kind and vascular supply. Although further investigation is required, HP may serve as an essential initial choice for the rapid management of tumor-associated bleeding. In mixed NVGIB cases (e.g., ulcers, tumors, or other etiologies), HP revealed a significant benefit in achieving hemostasis (OR: 2.40, p = 0.02). This indicates that the use of HP is an effective approach for urgent bleeding control in various NVGIB patients. Nonetheless, it did not reduce rebleeding rates, indicating that other interventions may still be required to rectify the underlying source of bleeding. In cases of peptic ulcer bleeding, HP and CT had comparable efficacy. This is logical as ulcers frequently respond favorably to CT, such as clipping or thermal therapy. HP also offers similar advantages in this context, making it the preferred method.
This meta-analysis demonstrated several significant strengths. This study exclusively included RCTs addressing NVGIB, thereby ensuring strong evidence for the efficacy of HP compared to CT. Studies that had significant effects on outcomes were excluded, leading to low heterogeneity in the analyses. This study analyzed nine RCTs from various countries, highlighting the international significance of the results. A comprehensive literature review included studies from previous meta-analyses to guarantee complete coverage of existing RCTs. Our results differed from earlier studies but were consistent with the latest research findings. The subgroup analysis defined by bleeding types further strengthened the significance of this study.
We need to acknowledge the limitations of our study for clarity. These trials included patients with various causes (such as malignant GI tumors, peptic ulcers, duodenal ulcers, etc.), demonstrating different types and levels of bleeding. Second, the definition of outcomes varied in particular studies, but we treated them as similar. Some studies lacked results, so most analyses included only three or four. Third, when interpreting these results, it is essential to consider the heterogeneity. Because the cost results were absent, we could not compare the costs of the groups. In addition, we did not analyze cases involving oozing and/or spurting bleeding (Forrest IA and IB). At the same time, the publication bias that could not be reliably assessed should also be kept in mind while interpreting the results. For an optimal hemostasis strategy, large-scale RCTs should compare HP monotherapy to combination therapies (e.g., HP plus clips). HP methods (kind, dose, reapplication intervals) must be standardized to reduce heterogeneity. Given HP’s greater material costs, cost-effectiveness and patient-centered outcomes (e.g., quality of life) should be investigated in future studies. Studies on GI malignancies or post-procedural bleeding may improve patient selection.
Conclusion
HP significantly improves hemostasis in NVGIB, especially in cases of tumor-associated bleeding, compared to CT. No differences in rebleeding, duration of hospital stay, or secondary outcomes support HP’s selection as a recommended intervention for acute GI bleeding management.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251406219 – Supplemental material for Efficacy of hemostatic powder for non-variceal gastrointestinal bleeding: a systematic review and meta-analysis of randomized trials
Supplemental material, sj-docx-1-tag-10.1177_17562848251406219 for Efficacy of hemostatic powder for non-variceal gastrointestinal bleeding: a systematic review and meta-analysis of randomized trials by Yingying Tao, Hayat Khizar, Haibin Zhou, Qingfeng Wu, Huang Jian, Yilei Lin and Jianfeng Yang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848251406219 – Supplemental material for Efficacy of hemostatic powder for non-variceal gastrointestinal bleeding: a systematic review and meta-analysis of randomized trials
Supplemental material, sj-docx-2-tag-10.1177_17562848251406219 for Efficacy of hemostatic powder for non-variceal gastrointestinal bleeding: a systematic review and meta-analysis of randomized trials by Yingying Tao, Hayat Khizar, Haibin Zhou, Qingfeng Wu, Huang Jian, Yilei Lin and Jianfeng Yang in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
None.
Declarations
Code availability
Not applicable.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the author(s) used AI-assisted technologies to improve language quality and Grammar checking. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.