
Abstract
Background:
Fecal microbiota transplantation (FMT) is an effective treatment for recurrent Clostridioides difficile infection (CDI) and shows promise for other dysbiosis-related conditions such as inflammatory bowel disease (IBD). Awareness and acceptance remain underexplored in the Middle East, where cultural and social factors may influence adoption.
Objectives:
To evaluate awareness, perceptions, willingness, and acceptance of FMT among the Lebanese population.
Design:
A nationwide cross-sectional survey with nonprobability sampling was conducted between April and November 2024.
Methods:
A total of 725 participants were recruited through mixed sampling across Lebanon’s governorates: 379 from the general population, 109 healthcare workers, 155 physicians, and 82 IBD or CDI patients. A structured bilingual questionnaire assessed awareness, perceptions, treatment preferences, and willingness to disclose or undergo FMT. Analyses included Chi-square tests, logistic regression, and false discovery rate-adjusted comparisons.
Results:
Overall, 31% of participants had prior awareness of FMT, while 60.1% reported positive perception. Awareness and perception were significantly associated (p = 0.0017) and were highest among physicians (59.4% and 70.2%) and lowest among patients (17.1% and 52.4%). Sources varied by group: universities for the general population, media for patients, and professional networks for healthcare workers and physicians. Logistic regression identified physician status, younger age, and prior awareness as predictors of favorable perception. Capsules were the preferred delivery route across groups. Willingness to disclose (81.4%) and to donate stool (68.4%) were high, while 17.2% expressed stigma-related concerns. Major concerns included hygiene, infection risk, and psychological discomfort.
Conclusion:
FMT awareness in Lebanon remains limited, particularly among patients and the public. Although perceptions are generally positive, misconceptions, stigma, and unrealistic expectations persist. These findings stem from a nonprobability sample that overrepresents younger, female, and highly educated participants and is not nationally representative. Targeted education, stronger physician–patient communication, and culturally sensitive approaches are needed to promote FMT acceptance and integration into practice.
Plain language summary
Fecal microbiota transplantation (FMT) is a treatment where healthy bacteria from one person’s stool are transferred to another person to help fix gut problems. It works very well for a serious infection called Clostridioides difficile (CDI), and it may also help people with diseases like inflammatory bowel disease (IBD). In this study, we asked 725 people in Lebanon—including doctors, patients, and members of the general public—what they know and think about FMT. We found that most people had never heard of FMT before, especially patients and non-medical individuals. Those who knew about it were more likely to think positively of it, especially younger people and doctors. After learning about FMT, most people were open to trying it, especially if it was recommended by a doctor. People had different opinions about how the treatment should be given, with many preferring capsules over other methods like colonoscopy. Common concerns included hygiene, infection risk, and the idea of using stool as treatment. Our results show that more education is needed to raise awareness and reduce stigma about FMT in Lebanon. Clear information from doctors and public campaigns could help more people accept this helpful treatment in the future.
Keywords
Introduction
Clostridioides difficile infection (CDI) and inflammatory bowel disease (IBD) are gastrointestinal (GI) diseases with overlapping risk factors and symptoms. CDI is primarily associated with antibiotic use, aging, and exposure to healthcare settings. 1 IBD is a chronic, relapsing inflammatory disorder encompassing two primary forms: Crohn’s Disease (CD) and Ulcerative Colitis (UC). While genetic predisposition plays a role in IBD susceptibility, it is insufficient to explain the high prevalence of the disease in developed and developing countries. Lifestyle factors, such as smoking and dietary habits, have been identified as significant contributors to IBD development.2,3 A common consequence of these factors is gut dysbiosis, a disruption in the composition and function of the intestinal microbiota, which plays a central role in the pathogenesis of both CDI and IBD. In CDI, antibiotics disrupt the gut microbiota, creating an environment favorable for the overgrowth of C. difficile. 4 In IBD, dysbiosis contributes to immune dysregulation, increased gut permeability, and chronic inflammation, which further perpetuates microbial imbalance. 5 Given the central role of the gut microbiota in GI homeostasis, strategies aimed at restoring microbial balance have emerged as promising therapeutic approaches for both conditions.
CDI presents a significant challenge in clinical treatment, particularly due to its high recurrence rate. 6 Physicians typically rely on antibiotics such as vancomycin or fidaxomicin, which effectively clear the infection in most cases. However, 15%–30% of patients experience recurrent CDI (rCDI) after an initial response to antibiotics, and 40% suffer another recurrence after recovering from their first relapse. 7 Given these challenges, researchers have explored fecal microbiota transplantation (FMT) as an alternative treatment. Studies have shown that while antibiotics alone have a 65% success rate, FMT boasts a 90% success rate with a significantly lower probability of recurrence. 8
IBD, on the other hand, is traditionally treated with medications such as aminosalicylates, corticosteroids, immunosuppressants, and biologics. However, these treatments often have serious drawbacks, including long-term complications and poor efficacy in some patients. FMT presents a highly promising alternative for IBD, as it has the potential to restore a healthy gut microbiome. Encouraging evidence from over 16 clinical trials has demonstrated that FMT can induce clinical remission in patients with UC, with reported remission rates ranging from 24% to 85%.9,10 These studies have primarily focused on evaluating FMT as a therapeutic option for UC, highlighting its potential effectiveness in managing the disease.
FMT offers a promising approach to restoring gut microbiota by transferring fecal matter from a healthy donor to a patient’s disrupted gut. 11 Historically, FMT traces back to ancient China, where the “yellow soup” was used to treat severe diarrhea and food poisoning. Modern FMT applications began in the 1980s with the use of fecal enemas to treat pseudomembranous colitis. 12 By the early 2000s, FMT gained recognition as a treatment for rCDI. A landmark 2013 study demonstrated remarkable outcomes, with 13 out of 16 patients achieving resolution of CDI after a single fecal infusion and additional successes following subsequent infusions. 13 In 2013, the U.S. Food and Drug Administration (FDA) allowed the use of FMT for rCDI without requiring enrollment in clinical trials, leading to its official FDA approval in 2022. 12
Due to its unconventional nature and strong cultural and psychological dimensions, awareness and acceptance of FMT vary widely across countries and cultures, shaped by differences in healthcare practices, public education, and social norms. The need to improve awareness of FMT and address access issues is particularly relevant in regions such as Lebanon, where the perception of FMT remains largely unexplored. This study aims to assess the awareness and perception of FMT among the Lebanese population while also providing education about its potential benefits and applications. By highlighting low awareness levels across sampled categories, the study underscores the necessity of targeted educational initiatives to bridge knowledge gaps and facilitate broader acceptance of FMT as a therapeutic option.
Methods
Participants and data collection
The study design follows the Consensus-Based Checklist for reporting of Survey Studies (CROSS) statement (Table S3). 14 This research was based on a cross-sectional survey conducted between April and November 2024 across various geographic areas in Lebanon, including Beirut, Bekaa/Baalbek-Hermel, Mount Lebanon, North Lebanon/Akkar, and South Lebanon/Nabatiyeh, to ensure broad representation.
We conducted an a priori sample size calculation for estimating a single proportion at 95% confidence using p = 0.50 and a margin of error ±5%, yielding n ≈ 385. Our final sample (n = 725) exceeds this threshold, corresponding to an approximate 95% margin of error of ±3.6% for overall proportions under simple random sampling. Participants were eligible if they were adults (⩾18 years) and belonged to one of the four target categories: general population, healthcare workers (nurses, pharmacists, dietitians, laboratory technicians, etc.), physicians, or patients diagnosed with IBD (UC or CD) or CDI. Individuals who did not agree to provide informed consent, or those with incomplete questionnaires, were excluded from the analysis.
A total of 725 responses were collected, comprising 379 individuals from the general population, 109 healthcare workers, 155 physicians, and 82 patients (75 IBD and 7 CDI patients). Participants were recruited using a mixed sampling approach that combined elements of random and convenience sampling. To introduce randomization, surveyors—students of the Lebanese American University (LAU)—were assigned to collect data in their respective governorates, ensuring coverage of diverse regions. All surveyors were trained to use a standardized strategy to reach the different target categories, ensuring consistency in recruitment methods. For the general population, participants were approached in high-traffic public locations such as streets, universities, malls, markets, and shops. Social media posts and stories were also used, with surveyors sharing their phone numbers so that interested individuals could complete the questionnaire via phone call. Convenience sampling was applied mainly to recruit physicians, patients, and healthcare workers. Physicians were approached through direct outreach at the LAU Medical Center–Rizk Hospital, affiliated clinics, and private hospitals, with additional contacts identified through hospital websites, particularly targeting gastroenterologists. Healthcare workers were recruited in hospitals, pharmacies, and private clinics through professional contacts. Patients were recruited via IBD and CDI social communities, support groups, and referrals from gastroenterologists’ private practices; no patient contact information was shared without prior permission from the relevant community or physician. Most participants in these categories completed the questionnaire in person at hospitals and clinics, while patients unable to attend were interviewed by phone. Importantly, none of the approached targets were asked any demographic questions to qualify their participation in advance; eligibility was instead determined by their belonging to the predefined categories.
To minimize human error in data entry, responses were entered directly by trained surveyors into a pre-coded database. Surveyors received standardized training on data collection procedures, and questionnaires were reviewed on the same day for completeness and consistency before entry. Double-checking of randomly selected entries was performed to ensure accuracy. All variables were pre-coded with unique identifiers to reduce transcription errors.
Participation was anonymous; no identifying information, such as names, contact details, or personal identifiers, was collected. Each completed questionnaire was assigned a unique study code. Data were stored in password-protected files accessible only to the research team. Hard-copy questionnaires (when applicable) were kept in locked cabinets at LAU. All electronic records were stored on secure institutional servers, and no data were shared with third parties. These measures ensured confidentiality and protected against unauthorized access.
Study development
A cross-sectional study was conducted to assess awareness and perceptions of FMT as a treatment for GI diseases among the Lebanese population (Figure S1). A structured questionnaire was designed, inspired by a previous study by Zipursky et al. 8 and modified to align with the objectives of this study. To ensure linguistic accuracy, the questionnaire was first translated into Arabic and then back-translated into English by bilingual experts. Both language versions underwent pilot testing to evaluate the clarity of instructions, question comprehension, and response ease. Participants completed the version of their choice—Arabic or English—according to their language preference.
The questionnaire included multiple sections tailored to different groups: physicians, IBD patients, CDI patients, and the general population. The questionnaire collected demographic data, including age, gender, current governorate of residence, governorate of origin, educational level, and healthcare worker status. Participants were presented with two scenarios to assess their treatment preferences for IBD and CDI. Background information was provided on the factors contributing to the depletion of healthy bacteria in the GI tract, which can lead to diseases such as UC, CD, and CDI, along with associated symptoms. In the first hypothetical scenario, participants were asked to imagine they had one of the above-mentioned conditions and to choose between two treatment options: (1) a course of antibiotics or an anti-inflammatory drug with lower chance of symptom cure or reduction, or (2) a new procedure (referred to as “X”) with higher chance of symptom cure or reduction. After recording their responses, participants were asked if they had heard of FMT. A brief introduction to FMT was then provided, including its routes of delivery, risks, and benefits. In the second hypothetical scenario, participants were asked the same question again after being informed that treatment (X) referred to FMT. For physicians, the questionnaire additionally explored their knowledge of FMT practices in Lebanon, the minimum remission rate they would consider acceptable, as well as their preferred timing to recommend FMT, preferences between synthetic and fecal stool, and their perceptions toward FMT as a future treatment option. For patients, the questionnaire examined their previous treatments, disease perceptions, openness to FMT, the severity of the disease required to consider FMT, factors encouraging them to try it, and the preference between fecal or synthetic stool for the treatment. The questionnaire included multiple-choice and optional short-answer questions, with participants invited to share any additional comments about FMT at the end.
Statistical analysis
Descriptive statistics were used to summarize demographic characteristics and survey responses. Associations between categorical variables (e.g., perception, awareness, respondent category, and demographics) were assessed using the Chi-square test, with pairwise comparisons and post hoc residual analysis performed when significant differences were observed. For ordinal outcomes, the Kruskal–Wallis H test was applied. McNemar’s test was used to evaluate within-subject changes in binary responses under different hypothetical scenarios. A binary logistic regression was conducted to identify predictors of positive perception toward FMT; the outcome was dichotomized (positive vs non-positive), and predictor variables included age, gender, education level, respondent category, and awareness. For multiple-choice questions, frequency analysis was performed to account for multi-response entries. Reported p-values are Benjamini–Hochberg false discovery rate (FDR)-adjusted within each outcome (Awareness, Positive perception) across m = 5 comparisons (Age, Gender, Education level, Governorate, Category), with FDR controlled at q = 0.05. The overall association between Awareness and Positive perception was a single test and was not multiplicity-adjusted. No weighting adjustments or formal sensitivity analyses were performed; national benchmarks were instead used to contextualize sample deviations. All statistical analyses were conducted using Python version 3.10 (Pyhton Software Foundation, OR, USA), and graphical figures were created using GraphPad Prism version 9 (GraphPad Software, Inc., CA, USA). Statistical significance was set at p < 0.05 or q < 0.05. Only complete responses were included in each analysis.
Results
Demographics of the study population
A total of 725 participants completed the survey. The most represented age group was 18–24 years (32.28%), indicating strong engagement from younger adults. The majority of respondents identified as female (62.21%) and held a bachelor’s degree (49.52%), reflecting a highly educated sample. Most participants were from the general population (52.28%, n = 379), while healthcare workers, physicians, and patients comprised 15.03% (n = 109), 21.38% (n = 155), and 11.31% (n = 82) of the sample, respectively. Geographically, the largest proportion of respondents resided in Beirut City (46.07%), followed by Mount Lebanon (32.14%; Table 1).
Demographic characteristics of the study population.

Treatment preferences, awareness, and perception
Following the initial presentation of a hypothetical treatment scenario and prior to the disclosure of treatment X as FMT, 75.46% of the general population, 79.27% of patients, and 82.58% of physicians selected it as their preferred option. After participants were informed that treatment X referred to FMT and were provided with a brief explanation of its nature, procedure, advantages, and disadvantages, the same scenario was reassessed. A slight decrease in preference was noted among the general population and healthcare workers (72.39%), and patients (74.39%), while physicians showed a modest increase (+2.59%). Despite these shifts, McNemar’s test within each group indicated that changes in preference were not statistically significant (p > 0.26 for all). Similarly, a Chi-square test comparing the magnitude of change across categories revealed no significant difference in preference change among the groups (p = 0.28).
Analysis of participant awareness revealed that overall familiarity with FMT in Lebanon was notably low, with only 31.03% of respondents (225 out of 725) indicating prior knowledge of the procedure (Table 2). Awareness differed markedly by participant category: physicians reported the highest awareness (59.35%), followed by healthcare workers (33.03%), while the general population (21.90%) and patients (17.07%) showed much lower awareness (q < 0.0001). Education level was also significantly associated with awareness (q < 0.0001), with respondents holding postgraduate degrees showing the highest awareness (41.41%), whereas those with no formal education reported the lowest (4.35%). Other factors, including gender (q = 0.057), age group (q = 0.0573), and governorate of residence (q = 0.2281), were not statistically significant after correction for multiple testing. Descriptively, younger participants aged 25–34 years showed somewhat higher awareness (39.46%) compared to older participants aged 51 and above (25.81%), and males reported slightly higher awareness (33.82%) compared to females (29.05%). However, these differences should be interpreted as trends only and not as statistically significant associations. Interestingly, only 18% of physicians who were aware of FMT knew that it is performed in Lebanon, while this proportion did not exceed 5% among the general population and patient groups.
Awareness and positive perception of fecal microbiota transplantation across demographic groups.

p-Values shown are FDR-adjusted.
q < 0.05.
Among those who were aware of FMT, sources of awareness differed significantly across categories (p < 0.0001, Chi-square test; Figure 1). In the general population, the most common source was university exposure (51.81%), followed by media (39.76%). Healthcare workers reported physicians or professional colleagues most frequently (52.78%), with university (19.44%) and media (22.22%) also contributing. For patients, the media was the dominant source (57.10%), while all other sources were equally cited (14.30% each). Physicians overwhelmingly reported professional sources: 69.6% learned from other physicians or healthcare professionals, while 17.40% cited university settings, and only 9.80% from the media.

Sources of awareness of FMT by participant category. Stacked bar chart showing the distribution of reported sources of awareness of FMT across four participant categories: general population, healthcare workers, patients, and physicians. Reported sources included friends/family, media, physicians/healthcare professionals, and the university. The y-axis indicates the percentage of respondents who reported each source within each category (Chi-square test, p < 0.0001).
Regarding perception, 60.13% of respondents held a positive view of FMT, 35.45% were neutral, and 4.41% expressed a negative perception. Notably, physicians demonstrated the most favorable perception, with 70.32% indicating a positive view, followed by healthcare workers (63.30%) and, general population (56.73%). Patients showed the lowest positive perception, with only 52.44% reporting favorable views. Notably, a strong correlation was observed between prior awareness and positive perception (Chi-square, p = 0.0017; Table 2). A multivariate logistic regression model identified younger age (OR = 1.69, p = 0.035), physician category (OR = 1.73, p = 0.034), and prior awareness of FMT (OR = 1.54, p = 0.02) as independent predictors of positive perception. Educational level, gender, and region were not significant in the adjusted model (Table 3).
Multivariable logistic regression identifying predictors of positive perception toward FMT.
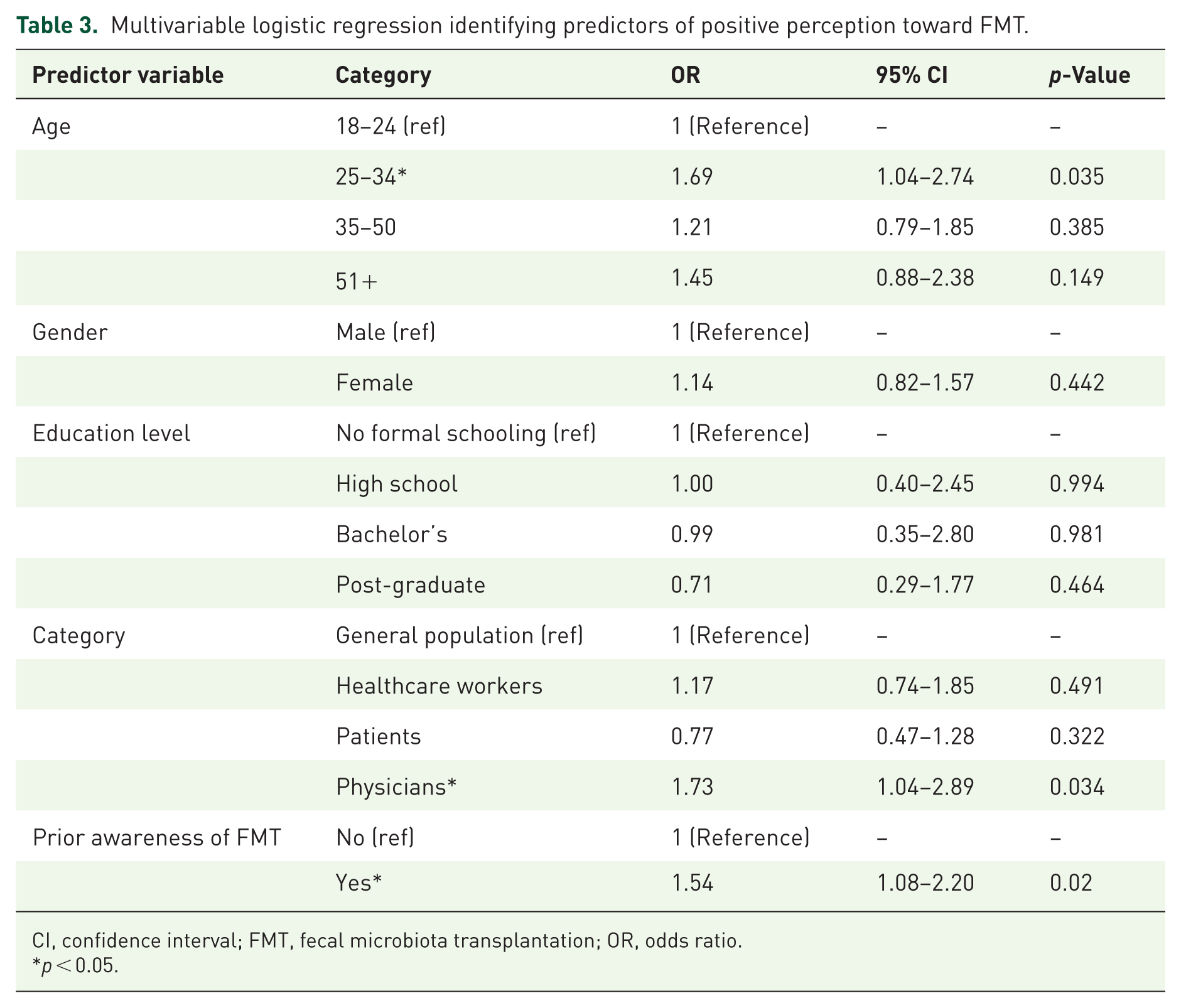
CI, confidence interval; FMT, fecal microbiota transplantation; OR, odds ratio.
p < 0.05.
Upon introducing FMT, participants were presented with its various routes of administration and asked to indicate their preferred method of delivery. Among the general population and healthcare workers, the most preferred route was the capsule, selected by 63.85% and 61.47% of respondents, respectively. Patients showed nearly equal preferences for colonoscopy and capsule, each chosen by approximately 45.12%. Physicians also predominantly favored the capsule, with 51.61% selecting this option (Figure 2).

Preferred routes of FMT delivery by participant category. Bar graph showing the distribution of preferred FMT delivery routes among respondents in each category (General Population, Healthcare workers, Patients, and Physicians). Options included colonoscopy, enema, nasogastric tube, and capsule. The observed variation in delivery route preferences across categories was statistically significant (Chi-square test, p < 0.0001).
Concerns and decision-making factors
We assessed how participants’ willingness to disclose having received FMT, their readiness to donate stool, and perceived stigma varied across sociodemographic groups. Overall, 81.38% of respondents reported willingness to disclose having undergone FMT, 68.37% were willing to donate stool, and 17.24% expressed fear of stigmatization (Table 4). After FDR correction, there were no statistically significant differences in willingness to disclose or willingness to donate stool between categories or demographic groups (q > 0.05). For fear of stigmatization, a trend was observed with differences across educational levels (uncorrected p = 0.0301), where participants with no formal schooling reported higher fear (26.09%) compared to those with higher education; however, this association did not reach significance after FDR adjustment (q = 0.1456). The only statistically significant difference that persisted after correction was by participant category (q < 0.0001), with physicians reporting the greatest concern about stigma (34.19%), compared to levels around 12% in the other three categories (Table 4).
Impact of demographics on FMT disclosure, stigma, and donation willingness.

p-Values shown are FDR-adjusted.
q < 0.05.
Concerns about FMT also varied significantly both within and across respondent categories (p < 0.001). Across all groups, the most frequently reported concerns were related to cleanliness and hygiene and the presence of infectious agents. Cleanliness and hygiene were cited by 39.80% of the general population, 44.04% of healthcare workers, 51.90% of patients, and 32.90% of physicians. Similarly, concerns about infectious disease transmission were reported by 54.90% of the general population, 45.87% of healthcare workers, 49.40% of patients, and 45.20% of physicians (Figure 3). Furthermore, differences emerged in the types and distribution of secondary concerns. Disgust or psychological aversion was cited most frequently by healthcare workers (47.71%) and the general population (40.20%), and less commonly by patients (30.90%) and physicians (27.10%). Patients expressed unique concerns reflecting clinical vulnerability, including fears that FMT might interfere with their current treatment (11.10%) or worsen their condition (33.30%). Physicians, in contrast, prioritized concerns grounded in scientific rigor and procedural consistency. These mainly included the absence of long-term efficacy and safety data (27.70% and 47.01%, respectively), lack of a standardized protocol (3.20%), and doubts about patient acceptance (8.40%). While concerns about disgust and infection were still present, they were less dominant relative to more technical issues. Chi-square tests within each category confirmed significant internal variability in concern distribution (p < 0.0001 for all groups).

Concerns about FMT by participants’ category. Bar graph showing the distribution of reported concerns regarding FMT among respondents in each category (General Population, Healthcare Workers, Patients, and Physicians). Concerns included hygiene, presence of infectious agents, safety, psychological aversion, and lack of clinical evidence or standardization (Chi-square test, p < 0.0001).
To explore physicians’ attitudes toward the timing of FMT recommendation, they were asked when they would consider advising its use. The majority (76.10%) indicated they would recommend FMT only after multiple recurrences or in severe stages of the disease. A smaller proportion (15.50%) supported its use as a first-line treatment immediately after diagnosis, while 8.40% stated they would never recommend it. Their reported timing of recommendation was significantly associated with physicians’ concerns about FMT (p = 0.0236). A post hoc standardized residual analysis revealed that the concern “I have no particular concern” was significantly overrepresented among physicians who would recommend FMT as a first-line treatment (standardized residual = +3.64). This finding suggests that lack of concern is a key determinant of physicians’ willingness to recommend early FMT, whereas specific concerns—such as hygiene, safety, or insufficient evidence—were more common among those preferring to delay recommendation or withhold it altogether.
To further investigate the factors influencing patients’ willingness to undergo FMT, the survey included a follow-up question exploring potential conditions under which initially hesitant patients might reconsider. Among these patients, 56.10% indicated they would be more likely to accept FMT if recommended by their physician, 41.46% if assured of its safety, 12.20% due to concerns about the side effects of their current treatments and a desire to reduce medication use, and 29.27% if all other therapies failed and they wished to avoid surgery (Table S1).
Accordingly, both patients and physicians were asked to indicate the minimum acceptable remission rate they would require for FMT to be considered a viable treatment. The majority of both groups—56.10% of patients and 59.35% of physicians—selected a 75% remission threshold. However, a significantly higher percentage of patients (29.27%), compared to physicians (9.03%), required a 100% remission rate (p = 0.0001; Figure 4).

Minimum acceptable remission rate for FMT by participant category bar graph showing the distribution of minimum remission rates considered acceptable for FMT among patients and physicians. Response options included >25%, >50%, >75%, and 100% remission thresholds. The observed difference in remission rate expectations between groups was statistically significant (Chi-square test, p = 0.0001).
Preferences regarding donor identity and fecal matter type were evaluated to explore factors influencing acceptance of FMT (Table S2). Across all participant groups, the most common response concerning donor identity was “doesn’t matter,” selected by 37.50% of the general population, 37.61% of healthcare workers, 45.68% of patients, and 49.03% of physicians. A preference for a family member was also frequently cited, particularly among the general population and healthcare workers (43.12% and 42.42%, respectively), compared to 30.97% of physicians and 36.42% of patients. As for the type of fecal material, no statistically significant differences were observed between groups in their preference for natural stool versus synthetic alternatives (Chi-square p > 0.05).
Discussion
FMT has emerged as a promising therapeutic option for GI, particularly for conditions such as CDI and IBD. While FMT is an established treatment for rCDI, it remains experimental for IBD due to limited clinical evidence and ongoing safety concerns.15,16 Its broader adoption, even for CDI, depends heavily on public and professional awareness, acceptance, and understanding.
To the best of our knowledge, this is the first study to assess awareness and perceptions of FMT in Lebanon, where cultural and societal factors significantly influence health-related decisions. Understanding these perspectives is essential to identifying implementation barriers and addressing misconceptions. Unlike previous studies that focused on specific subgroups, this study included the general population, healthcare workers, physicians, and IBD and CDI patients, allowing for a more comprehensive view of perceptions across various levels of knowledge and cultural backgrounds.
The hypothetical scenarios revealed shifts in treatment preferences after participants learned that treatment X referred to FMT. Initially favoring conventional options, preferences slightly declined among the general population and patients, but increased among physicians, though differences were not statistically significant. A similar trend was observed in other studies, where FMT’s identification led to decreased acceptance among some participants. 8 Our findings revealed a significant disparity in FMT awareness across the three studied groups. While physicians and healthcare workers demonstrated greater familiarity with the procedure, awareness among the general population and patients was limited. These results align with global studies indicating low awareness of FMT in nonmedical populations.17,18 Similarly, even among postgraduate medical students, half had limited knowledge of FMT, reflecting its relative novelty and limited clinical application. 19 The main sources of information also varied: the general population cited universities, patients cited media, while healthcare workers and physicians cited professional networks. The low percentage of patients receiving FMT information from their physicians highlights a gap in patient-provider communication.
Perception of FMT was generally positive, with nearly two-thirds of respondents expressing favorable attitudes. Physicians and healthcare workers were the most supportive group, consistent with prior studies indicating that healthcare professionals are more likely to endorse FMT due to their clinical familiarity. 20 In contrast, neutral or negative perceptions were more common among patients and the general public, likely reflecting knowledge gaps and misconceptions.
Awareness was strongly associated with positive perception, reinforcing the role of prior exposure, as previously demonstrated in quantitative research. 19 Younger age, physician status, and awareness were identified as independent predictors of favorable attitudes. Another noteworthy finding is that only 18% of physicians who were aware of FMT knew that the procedure is performed in Lebanon. This reflects an information gap within the medical system, likely attributable to the fact that FMT is currently offered in only a very limited number of centers. Because our physician sample was drawn from diverse institutions, many respondents were not exposed to centers where the technology is practiced. This limited dissemination may also reflect the absence of standardized national guidelines or structured training opportunities on FMT. Addressing this gap will be essential to improve physician awareness and ensure broader clinical integration of the procedure. The limited awareness of FMT across all groups, including its availability in Lebanon, points to the need for targeted educational efforts. Media campaigns may be more effective for the general population, while professional development and improved physician–patient communication are needed in clinical settings. Our findings support the need for initiatives that enhance understanding and acceptance of FMT, especially as its applications expand beyond infectious diseases and broader clinical adoption relies on reducing public hesitancy.
FMT delivery routes significantly influenced participant preferences. Capsules were the most preferred method across all groups, while patients also equally favored colonoscopy. These findings are in line with other research, which reported strong preferences for oral administration. 21 Interestingly, patients’ preference for colonoscopy may be due to familiarity with the procedure or the belief that a single administration is less burdensome than repeated treatments.
Disclosure willingness was relatively high, suggesting increasing social acceptance of FMT. However, stigma remains a concern, particularly among those unwilling to disclose, due to taboos surrounding bodily functions. Fear of judgment and lack of a clear rationale also contributed to reluctance. Physicians’ concerns about long-term effects influenced their willingness to recommend FMT, mirroring the findings of other studies.22,23 Stigma and patient hesitancy also emerged as major issues. While other studies found that most patients were open to trying FMT despite initial discomfort,16,19,24 our findings suggest more caution, especially due to fears of condition worsening. Interestingly, our study revealed that physicians reported greater concerns about stigma than patients. This observation may have several explanations. Given the novelty of FMT, its limited awareness in Lebanon, and the lack of long-term outcome data, physicians may fear that recommending such a procedure could negatively impact their professional reputation if results do not meet expectations. Another factor could be communication gaps, where physicians anticipate resistance from patients and thus project stigma concerns onto them. It is also important to note that physicians, as members of the broader society, are themselves influenced by prevailing cultural and ethical attitudes toward bodily substances. Consequently, their concerns may not be purely clinical but also shaped by the same social norms and sensitivities that affect the general population. These findings highlight the need for physician-targeted education and training to reduce stigma and improve patient–physician dialogue around FMT.
Common concerns included disease transmission, aligning with. 25 Hygiene and psychological disgust were other concerns—consistent with studies that found that the term “fecal” itself reduced acceptance. 26 These concerns highlight the need for further research to fully acknowledge the side effects and long-term effects of FMT. Furthermore, this expresses the need to standardize the procedure and enhance the screening protocols to minimize the risk of infection and promote safety.
Efficacy was a critical factor in FMT acceptance. Most physicians and patients required a remission rate of over 75% to consider it viable. This aligns with the study by Zhang et al., 27 which reported high remission rates in UC patients treated with FMT. Our data also reveal a striking gap in expectations, with 29.3% of patients demanding a “100% remission rate” compared to only 9.7% of physicians. This mismatch likely reflects an information and communication gap between patients and their healthcare providers. Unrealistic expectations of absolute cure may amplify disappointment, reduce trust, and complicate treatment adherence if outcomes fall short. While our study could not investigate this aspect directly, it underscores the importance of physician–patient dialogue and structured educational efforts to align expectations. Future work should assess how best to provide patients with accurate, accessible information about FMT outcomes and to integrate expectation-setting into clinical practice and guideline development.
Physicians played a central role in shaping patients’ willingness to undergo FMT. Many IBD patients were more likely to accept FMT if it was physician-recommended, with physician endorsement identified as the most influential factor, consistent with Liu et al. 16 and Wu et al. 19 Safety was the second most important consideration, reflecting concerns about infection transmission and long-term effects.24,26 Some patients also viewed FMT as a last-resort treatment before surgery, a sentiment echoed in Ma et al. 22 and Al-Bakri et al. 23 Others were drawn to FMT for its potential to reduce medication use or because it is perceived as a “natural” therapy. 23 CDI patients, in particular, saw FMT as a natural and safer alternative to conventional treatments. Most physicians preferred recommending FMT after several recurrences or in severe cases, rather than as a first-line option, which is consistent with other studies.19,23 Few physicians reported they would never recommend FMT, likely due to safety and long-term efficacy concerns.
Regarding stool donation, most participants were willing to donate, with physicians showing the highest willingness. Among those unwilling, discomfort, disgust, and privacy concerns were common. 19 Physicians and patients were generally indifferent to donor characteristics, while the general population preferred family donors, likely due to trust and familiarity. Physicians’ preference for anonymous donors reflects their understanding of standardized screening.
Cultural and religious beliefs may also play a role in shaping attitudes toward FMT. 22 In the Lebanese context, both cultural stigma and religious considerations are likely to influence willingness to undergo or recommend FMT. Social stigma around bowel health and fecal material is deeply rooted, and the psychological “disgust” factor may be amplified by cultural taboos against openly discussing GI issues. Religious perspectives also carry weight. Both Islam and Christianity, the predominant religions in Lebanon, emphasize the preservation of health and generally allow donation practices if they relieve suffering and do not cause significant harm to the donor. Informed consent of the donor is also a shared requirement. In Islam, the main concern does not center on donation itself but rather on the fact that fecal matter is considered impure. Nonetheless, Islamic jurisprudence permits exceptions when medical necessity or life-saving treatments are involved, which could support the use of FMT if it improves outcomes. Within Christianity, donation is typically viewed positively as an act of compassion and solidarity, provided it respects the dignity of both donor and recipient. Additional concerns may also arise for individuals adhering to religious dietary restrictions, who might question whether the donor’s habits could affect the recipient’s body or health. 23 Although these religious and cultural dimensions are central to understanding FMT acceptance in Lebanon, our study could not explore them directly. In Lebanon’s sociopolitical context, asking about religion is highly sensitive due to the presence of multiple sects and their historical role in shaping political and social life. For this reason, collecting religious identifiers may have discouraged participation or introduced bias. We therefore acknowledge this as a limitation, while underscoring that future studies in the Middle East should carefully incorporate religious and cultural variables to better capture their impact on FMT acceptance.
In our study, participants across groups generally favored synthetic over natural stool, citing safety and infection risk as key factors. Similar preferences were observed by Al-Bakri et al., 23 while other studies28,29 noted interest in natural stool for its perceived holistic benefits. Safety concerns and donor limitations have driven the development of alternatives such as Fecal Microbiota Products (FMP) and Live Biotherapeutic Products (LBP). 30 Unlike FMT, which relies on stool donors, LBPs consist of defined microbial strains and have received FDA approval for CDI, whereas FMPs, stool-derived products with standardized processing, 31 remain experimental.
This study has some limitations. First, the sample was obtained via mixed convenience and targeted recruitment and is not probability-based, which limits generalizability. Compared with national benchmarks from Lebanon’s Labor Force and Household Living Conditions (LFHLCS) 2018–2019 survey, our sample tends to over-represent females, younger adults, and highly educated participants compared to national population benchmarks. 32 For example, young adults formed a larger share of our respondents than they do in the national data, and the proportion of participants with a university degree or higher was also higher than reported in the national survey. It is important to note, however, that the LFHLCS education figure reflects the highest attainment across all residents aged 3 and above at the time of the survey and is categorized differently from ours; it should not be interpreted as the eventual lifetime proportion of university-educated adults. Another limitation of our study is the low number of CDI patients (n = 7) compared to the total sample of 725 participants. This is explained by the fact that CDI incidence in Lebanon has only been reported in hospital-based settings (≈2 per 1000 admissions), with no available population-based prevalence data. 33 In our study, CDI patients were recruited exclusively from cases diagnosed upon admission at the LAU-affiliated hospital during the study period, which represented the maximum number accessible during the study period. Although this limits the strength of conclusions regarding CDI, their inclusion nonetheless provides valuable first insights into awareness and perception in this under-represented patient population. These deviations likely inflate awareness and acceptance estimates relative to the general adult population and may shape preferences (e.g., route of delivery). We therefore interpret level estimates cautiously and emphasize patterns/directions rather than population prevalence.
In addition, religious affiliation and cultural background were not collected, which limited our ability to conduct subgroup analyses on these potentially influential factors. Furthermore, as a cross-sectional survey, the study captures perceptions at a single point in time and cannot establish causal relationships. Awareness and attitudes toward FMT are likely to evolve as the procedure becomes more widely available and as new evidence emerges. A longitudinal design would therefore be needed to assess changes over time and to determine whether interventions, such as awareness campaigns or clinical exposure, effectively shift perceptions. Finally, the study relied on self-reported data, which may introduce subjectivity and response bias. Participants may have provided socially desirable answers, overestimated their knowledge, or misinterpreted questions despite the surveyor’s guidance. In addition, telephone interviews with some patients may have influenced how openly sensitive topics were discussed. These factors may lead to overreporting of awareness or positive perceptions and underreporting of stigma, and they should be considered when interpreting the findings.
Conclusion
This study provides the first systematic assessment of FMT awareness and perceptions in Lebanon across four key groups: the general population, healthcare workers, physicians, and patients with IBD or CDI. Overall awareness of FMT was low, especially among patients and the general public, though perceptions were generally positive and capsules were the preferred delivery route across groups. Important gaps were identified, including physicians’ limited knowledge of local FMT availability, patients’ unrealistic expectations of cure, and stigma-related concerns. These findings underscore the influence of cultural and educational factors on acceptance and highlight the need for targeted awareness campaigns, improved physician–patient communication, and culturally sensitive educational strategies. The study sample, however, overrepresented females, younger individuals, and highly educated participants, and should not be interpreted as nationally representative. Despite limitations related to sampling, subgroup size, and cross-sectional design, this study provides valuable baseline data to inform future longitudinal and interventional research aimed at facilitating the integration of FMT into clinical practice in Lebanon and the wider region.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251399034 – Supplemental material for Awareness and perception of fecal microbiota transplantation in Lebanon: a cross-sectional survey among the general population, healthcare workers, physicians, and patients
Supplemental material, sj-docx-1-tag-10.1177_17562848251399034 for Awareness and perception of fecal microbiota transplantation in Lebanon: a cross-sectional survey among the general population, healthcare workers, physicians, and patients by Maysam Shayya, Zeinab Wehbi, Miriam Matar, Mariana Elzein, Zeinab Safieddine, Karen El Khoury, José-Noel Ibrahim, Hussein F. Hassan, Omar Jamal, Rajaa Chatila and Philippe Hussein Kobeissy in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.