
Abstract
Background:
To standardize the treatment of inflammatory bowel disease (IBD) by establishing clear treatment targets and optimizing management strategies, the International Organization for the Study of IBD has proposed a treat-to-target (T2T) approach, which is now a popular management paradigm for IBD. However, this paradigm, which was derived primarily from Western countries with a high prevalence of IBD, has not been adopted universally. There is limited information on how T2T strategies are implemented around the world, and particularly in countries where IBD is a more recent phenomenon and has lower prevalence.
Objectives:
The aim of this study was to take advantage of the existence of the BRICS IBD Consortium (Brazil, Russia, India, China, and South Africa), a newly formed multinational organization, to get a realistic appraisal of gastroenterologists’ attitudes concerning the IBD treatment strategies.
Design:
A 59-question online questionnaire was distributed to 227 gastroenterologists from the BRICS countries between February and April 2024.
Methods:
Data on gastroenterologists’ characteristics, treatment strategies, and adoption of the STRIDE (Selecting Therapeutic Targets in Inflammatory Bowel Disease)-II consensus were collected, focusing primarily on viewpoints and challenges toward IBD T2T strategies.
Results:
More than 70% of respondents considered clinical and endoscopic remission, improved quality of life, absence of disability, and restoration of normal growth in children as the most important goals for IBD treatment. Concerns and challenges raised toward the International Organization for the Study of IBD (IOIBD) T2T strategy were the lack of a validated definition of mucosal healing (66.1%), guidelines conflicted with clinical experience (40.1%), psychological comorbidities (89.4%), loss of response to medical therapy (74.9%), complications associated with penetrating Crohn’s disease (CD; 74%), fistulising perianal CD (67.4%), and high out-of-pocket costs of therapeutic drug monitoring (69.6%). A step-up strategy was preferred (89%) in mild-to-moderate ulcerative colitis, whereas a top-down strategy was selected by the majority (72.2%) of respondents for CD management. Overall, the BRICS survey indicated that most of the participants had relatively high confidence in the IOIBD T2T recommendations.
Conclusion:
Although various concerns were identified, the BRICS survey showed that T2T strategies for IBD have been generally well received but not universally adopted by most gastroenterologists in countries with the more recent emergence of IBD.
Introduction
Inflammatory bowel disease (IBD) is a highly heterogeneous immune-mediated disorder that includes primarily Crohn’s disease (CD) and ulcerative colitis (UC) and is characterized by chronic relapsing-remitting inflammation of the gastrointestinal tract with serious medical, social, familial, financial, and quality of life (QOL) implications. The incidence and prevalence of IBD are lower in newly industrialized countries than in Western countries such as Europe and North America. However, by 2020, a rapid increase in IBD incidence had been observed in emerging nations. 1
Despite its multifactorial and very complex pathogenesis, significant progress made over the last decades has led to new and more effective treatment strategies that offer numerous single or combined therapeutic choices. 2 Among these, the STRIDE (Selecting Therapeutic Targets in Inflammatory Bowel Disease) consensus, first proposed in 2014 by the International Organization for the Study of IBD (IOIBD) and subsequently updated in 2021, is an expert consensus that recommends the Treat-to-Target (T2T) approach.3,4 The strategy for IBD represents an adaptation of the one originally developed for the management of other chronic diseases such as rheumatoid arthritis, hypertension, and diabetes. The T2T approach includes short, intermediate, and long-term targets tailored to the characteristics of the disease, with the goal of identifying specific therapeutic targets rather than merely obtaining a clinical response, and includes both clinical and endoscopic remission, with the ultimate aim of improving QOL and preventing disability.
Although STRIDE proposed a management consensus, to what extent gastroenterologists at large are aware of it and adhere to its T2T approach or adopt other therapeutic modalities is unknown, particularly in countries where IBD prevalence is lower. This is further confounded by the notable differences in healthcare systems and the availability of IBD experts, technologies, and medications across countries. Therefore, this study aimed at assessing the attitudes of physicians from newly industrialized nations toward T2T guidelines, document challenges encountered with their use, and eventually propose actions to address gaps and differences. This was accomplished by taking advantage of the newly created BRICS IBD Consortium whose countries (Brazil, Russia, India, China, and South Africa) belong all to the category of emerging nations, but are markedly diverse in regard to geographic location, climate, population size and territorial distribution, ethnicity, educational level, geopolitical status, industrialization, access to medical care, and overall human development index (https://hdr.undp.org/data-center/human-development-index#/indicies/HDI). All these factors are notably different from those of the Western countries where the T2T guidelines were developed, making a comparison with BRICS countries especially informative.
Materials and methods
Study design
A web-based questionnaire prepared based on the STRIDE-II guidelines 4 was distributed to gastroenterologists from BRICS countries between February 16 and March 31, 2024, securing 227 respondents out of 227 invitations, achieving a 100% response rate. Each participant received one invitation to minimize duplication and ensure data reliability. The questionnaire was pilot-tested by three independent IBD experts prior to dissemination, and several items were revised based on their feedback to improve clarity and content validity. It consisted of 59 questions. Questions 16–20, 22–23, 25–38, 42–44, 48–52, 55, and 58–59 are directly related to the T2T approach, which is central to manage IBD patients. The final version inquired about the following components:
Professional and work setting characteristics
Ancillary laboratory and technological resources
Medications
Treatment goals
Treatment strategies
Monitoring and follow-up
Adoption of and alternatives to the STRIDE-II consensus
In this study, we primarily analyzed the overall responses from BRICS countries. In addition, we compared IBD specialists with general gastroenterologists, and less experienced physicians (1–5 years of IBD experience) with more experienced physicians (>5 years), particularly in terms of treatment approaches and treatment goals.
In China, the members of the IBD group of Digestive Disease Branch, China Association of Medical Equipment, the members of China IBD Youth Club, and some senior Physicians of IBD Regional Center across China were invited to participate in the survey. In other BRICS countries, the questionnaires were sent to physicians affiliated with leading IBD centers of each country.
The study was conducted in compliance with the ethical guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board in accordance with the regulations and institutional policies of the Zhuo Pu Hospital, Shanghai University of Medicine and Health Sciences, China (approval No. 2024-C-45). It was reported in accordance with the Checklist for Reporting Results of Internet-Based Surveys (CHERRIES). 5 Details of the questionnaire are shown in the Supplemental Material. All invited BRICS physicians participated voluntarily in the survey, and no compensation was offered for participation.
Statistical analysis
Given that all the study variables were qualitative, descriptive statistics used for data presentation included frequencies (n) and percentages (%). The Chi-square test or Fisher’s exact test was used for the analysis between groups, with a level of statistical significance set at p < 0.05. The data were analyzed using SPSS for Windows version 29.0 statistical software (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 10.0 (San Diego, CA, USA).
Results
Professional and work setting characteristics
Respondent included 203, 9, 6, 5, and 4 gastroenterologists from China, India, South Africa, Brazil, and Russia, respectively. Characteristics of the survey respondents and their work setting characteristics are illustrated in Supplemental Table 1.
Most of the respondents were from a university teaching hospital (68.7%), with India having the highest proportion (100%). Among respondents, 64.8% were women, with the highest proportion observed in China (69.0%), while India reported no female participants. Specialty distribution varied slightly, with 49.8% being general gastroenterologists and 45.8% being IBD specialists. In addition, 54.2% of the respondents had >10 years of clinical experience in IBD management. Apart from treating adult patients, 80.6% of all respondents also provided care for patients under 18 years old. Meanwhile, 73.3% of responders had a multidisciplinary team for IBD management, except those for South Africa, with only 33.3%, a noticeably lower difference. Approximately half (54.6%) of the respondents reported having a dedicated IBD electronic database, with the highest prevalence in China (56.7%).
Ancillary laboratory and technological resources
Most institutions offered routine blood testing and measurement of albumin, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR), but only 67% had access to fecal calprotectin (FC), which is markedly lower than other tests. Measurement of routine blood values, albumin, and ESR were lower (66.7%) in South Africa than in the other BRICS countries. Testing for tumor necrosis factor-α (TNF-α) and infliximab (IFX) levels was available for 57.7% and 51.1%, respectively, while that for 6-MP (6-Mercaptopurine), FK506 (tacrolimus), cyclosporine A and ATI (antibodies to IFX) ranged from 35.2% to 14.5%. Most respondents stated that their workplaces had magnetic resonance enterography (MRE, 75.8%), computed tomography enterography (CTE, 83.7%), endoscopy (94.7%), enteroscopy (83.7%), and capsule endoscopy (81.5%), but only 66.5% had intestinal ultrasound (IUS) and 47.6% had 18-fluorodeoxyglucose positron emission tomography.
Medications
The vast majority (>90%) of respondents reported availability of corticosteroids and biological agents for inducing remission (Supplemental Figure 1). Additionally, 74.9% of participants had access to immunomodulators and 60.4% to small-molecule drugs. Nearly half (49.3%) of respondents had access to biosimilars. As for supplementary treatments, nutritional support was available to 91.2% of respondents, while probiotics, traditional medicine compounds, and mineral supplements were accessible to 78.4%, 63%, and 38.8%, respectively.
Treatment goals
More than 70% of respondents favored clinical remission, endoscopic remission, improved QOL, absence or reduction of disability, and restoration of normal growth in children as the most important treatment goals for IBD (Figure 1). Surprisingly, among Indian respondents, achieving endoscopic remission was a significantly less important goal (22.2% vs 89.0% in other BRICS countries for UC, p < 0.001; 44.4% vs 84.4% in other BRICS countries for CD, p < 0.001). Endoscopic mucosal healing (MH) as a treatment goal was favored by 96% of respondents for UC and 91.2% for CD, but only 22.2% and 33.3% of Indian respondents selected MH as an important goal for UC and CD, respectively, a significantly lower (p < 0.001) percentage compared to the other BRICS countries. A possible reason might be the lack of randomized clinical trials (RCTs) that definitively support MH as a therapeutic gold standard in UC or CD. 6
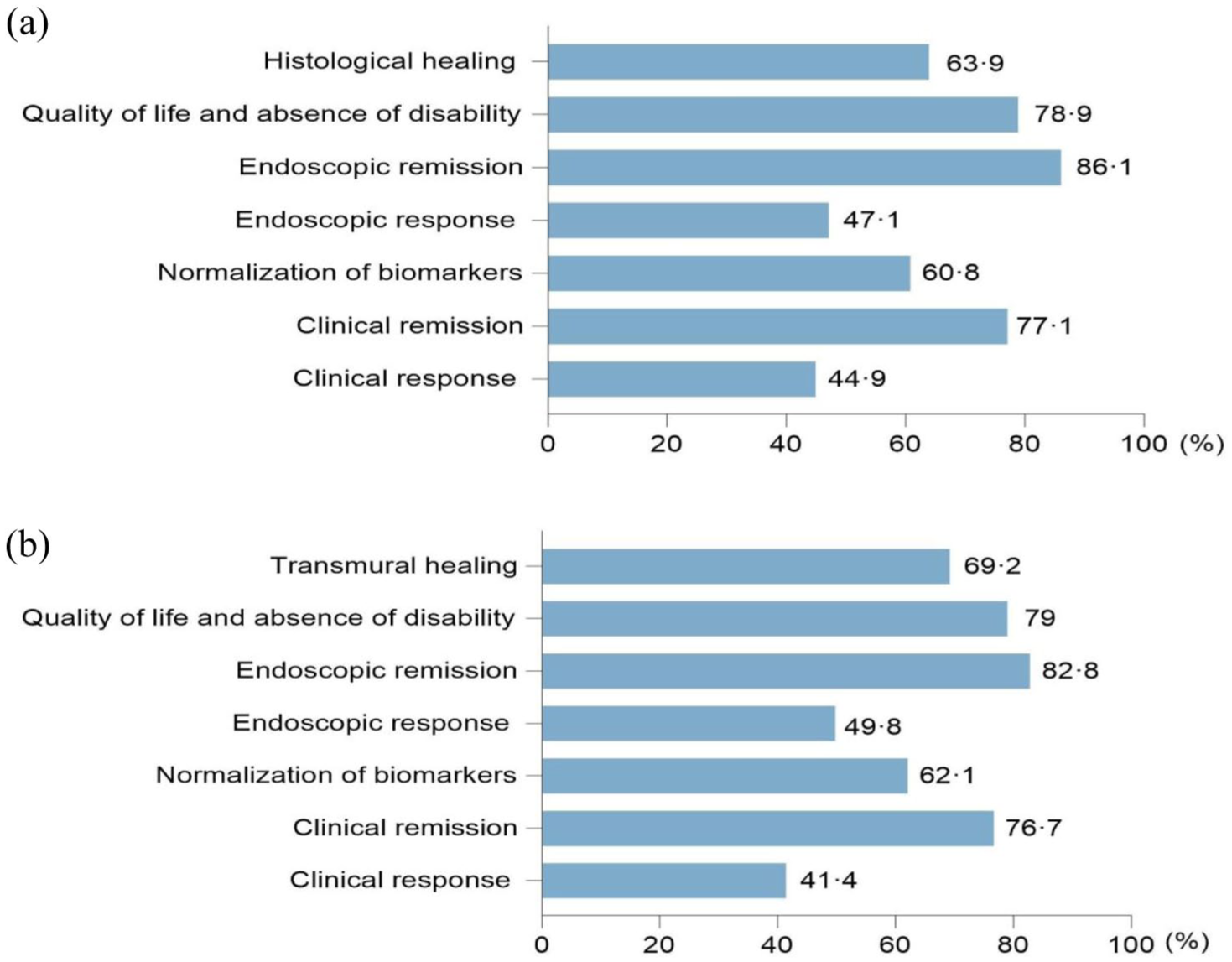
Most important treatment goal in ulcerative colitis (a) and Crohn’s disease (b).
Additionally, 82.4% of responders favored histological remission (HR) as a long-term goal for UC and 79.7% for CD, with 58.2% and 56.4% suggesting assessment every 6 months to 1 year as follow-up for UC and CD.
When defining endoscopic healing in UC, 43.6% of the respondents chose a Mayo endoscopic score (MES) of 0, and 32.2% a MES ⩽1 (Figure 2). For CD, 27.8% of them favored a Simple Endoscopic Score for CD (SES) of ⩽2 to define endoscopic healing, with 26.9% preferring a stricter criterion of SES-CD = 0. Furthermore, 59% and 60.8% of responders considered that the definition of complete deep healing for UC and CD, respectively, involved clinical, biochemical, and endoscopic remission, plus histological healing (HH) for UC and transmural healing (TH) for CD. Less experienced physicians were significantly more likely than experienced physicians to agree with this definition (70.4% vs 55.5%, p < 0.05). Similarly, IBD specialists were more likely to agree compared to gastroenterologists in China (69.5% vs 55.6%, p < 0.05).
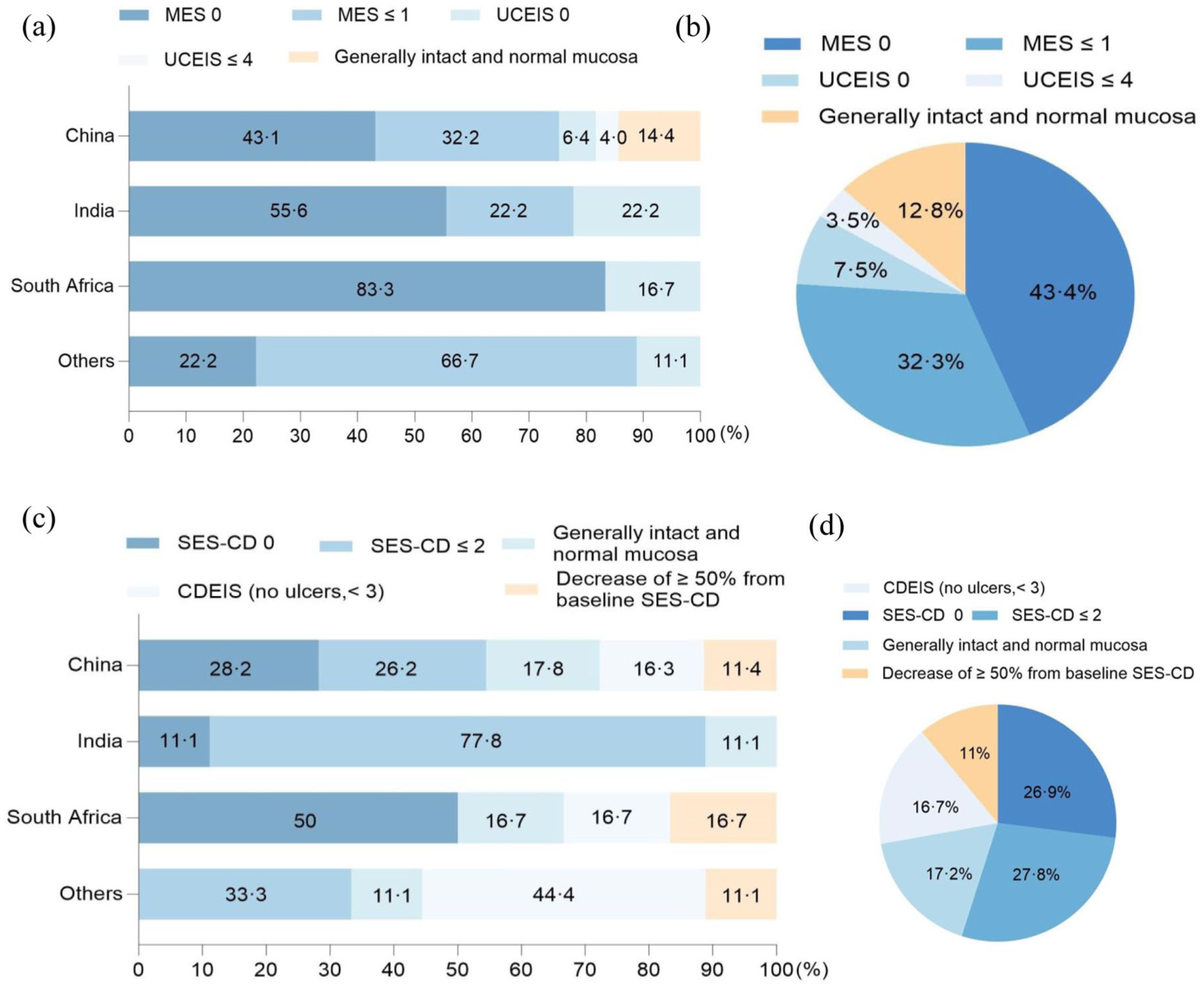
Definition of endoscopic healing in ulcerative colitis (a, b), Crohn’s disease (c, d).
Treatment strategies
Treatment preferences varied significantly depending on disease severity and the country surveyed. Most respondents (89%) indicated that the step-up strategy was appropriate for managing mild-to-moderate UC, and 82.8% preferred the top-down strategy for severe UC. Experienced physicians were significantly more likely to choose the top-down approach than less experienced physicians (85.5% vs 74.1%, p < 0.05).
However, as compared to physicians from other BRICS countries, only 44.4% of Indian physicians favored an outright top-down approach for severe UC (p < 0.001), adopting corticosteroids as the first option, followed by biologics if steroid dependent, azathioprine, or steroid refractory. For CD, 72.2% of participants favored a top-down strategy, but the proportion in India, Brazil, and Russia was lower (44.4%) while in China it was significantly higher (75.4%; p < 0.001), especially compared to IBD specialists with gastroenterologists (83.2% vs 69.7%, p < 0.05). Similarly, experienced physicians were significantly more likely to choose the top-down strategy for CD than less experienced physicians (74.0% vs 66.7%, p < 0.05).
Nearly all participants set short-term, medium-term, and long-term therapeutic objectives for their IBD patients. As for treatment escalation, the primary reasons cited by most participants included lack of clinical response and failure to achieve clinical remission (Figure 3). After achieving clinical remission, 85.5% of the respondents reported they would intensify treatment to attain MH, but only 11.1% of Indian physicians did so. Toward the goal of achieving HR in UC, 63.4% of all respondents would escalate treatment, but only 11.1% in India and 22.2% in Brazil and Russia. Less experienced physicians were more likely to escalate treatment compared to experienced physicians (75.9% vs 59.5%, p < 0.05). In China, 77.8% of gastroenterologists and 57.9% of IBD specialists would escalate treatment (p < 0.05). For CD, 70.9% would escalate treatment to achieve TH,, but only 33.3% in India and 11.1% in Brazil and Russia. In China, 80.1% of gastroenterologists and 69.5% of IBD specialists would escalate treatment (p < 0.05).

Situations to upgrade treatment in inflammatory bowel disease.
Monitoring and follow-up
Almost all respondents performed endoscopy to monitor disease activity and assess treatment response (Supplemental Figure 2). Regarding the frequency of colonoscopy monitoring for UC and CD, 81.9% and 77.1% of the respondents, respectively, favored an interval of 6 months or 1 year. As for the reason for not conducting endoscopic monitoring, 55.5% replied that endoscopy was invasive. Respondents performed CTE, MRE, and IUS at 74%, 70%, and 59%, respectively, for CD, but less so for UC, with CTE at 41.4%, MRE at 26.9%, and IUS at 40.1%. Other methods for disease monitoring included biochemical markers such as CRP, FC, and ESR, as well as various imaging methodologies, with clear discrepancies noted across different BRICS countries.
In terms of the frequency of disease reevaluation for UC, 48.5% of the respondents reported that a period of 1–3 months was appropriate, while 41% preferred an interval of 6–12 months. For CD, 43.6% indicated that the optimal frequency was every 3–6 months, with 40.5% favored a shorter interval of 1–3 months. Most respondents (94.7%) conducted regular blood tests to monitor the clinical efficacy and side effects of medications. Regarding reasons for discontinuing immunomodulators, 91.6% reported adverse events, 74% reported loss of effect, and 67.8% switched to biologics. Among the reasons for discontinuing biologics or biosimilars (as multiple-choice options), 88.5% of respondents cited adverse events, and 81.1% reported loss of effect. In addition, 52.9% of the respondents reported that infectious complications among patients using immunomodulatory or biologic treatments were about <5%, while 27.8% reported a rate of <1%. Finally, 58.6% reported that the incidence of lymphoma post-IBD treatment was essentially zero, while 41% reported 1%–5%. A dual-energy X-ray absorptiometry scan in cases of IBD with persistent or prolonged disease duration was occasionally performed.
Adoption of and alternatives to the STRIDE-II consensus
A considerable proportion of participants always (55.5%) or often (30%) referred to the STRIDE-II consensus, but 55.5% also followed other guidelines, such as the American Gastroenterological Association (AGA) guidelines or European Crohn’s and Colitis Organisation (ECCO) guidelines (Figure 4). More experienced physicians were significantly more likely to refer to other guidelines compared with less experienced physicians (60.1% vs 40.7%, p < 0.05). In China, IBD specialists were also more likely than gastroenterologists to consult international guidelines (65.3% vs 46.5%, p < 0.05). Confidence in the STRIDE-II guidelines was generally high, with 48% of participants expressing high and 42.3% expressing moderate reliance. However, more than half of the Indian respondents reported limited confidence. Regarding the reason for not following the STRIDE-II consensus, 66.1% deemed that the lack of a validated definition of MH was an important factor. Forty percent of respondents stated that if some guidelines conflicted with their own clinical experience, they would intentionally not follow them.

(a, b) Refer to consensus. (c, d) Confidence of consensus.
To acquire the latest information on IBD, the majority of respondents favored conferences (92.5%), followed by reading journal articles (76.7%), and web-based learning (74.9%). These approaches were deemed extremely useful (72.7%) for guiding actual clinical practice.
In the practical management of IBD patients, 89.4% of respondents reported that psychological comorbidities posed significant challenges to implement T2T strategies, followed by the challenges of handling loss of response to medical therapy (74.9%), complications associated with penetrating CD (74%), and managing fistulising perianal CD (67.4%; Figure 5). For therapeutic drug monitoring (TDM), 69.6% of respondents reported that high out-of-pocket cost was an important barrier, 39.6% admitted to a lack of comprehensive TDM knowledge, 35.2% thought TDM processes were cumbersome and/or time-consuming, and 34.4% reported a lack of TDM use in clinical practice.

Challenges in the management of inflammatory bowel disease.
Discussion
The investigation of real-life IBD management practices in the five BRICS nations revealed several enlightening similarities and differences with those of Western countries, as well as variable degrees of acceptance and use of the T2T guidelines recommended by the STRIDE consensus. The majority of BRICS respondents worked in academic settings and routinely managed both adult and pediatric IBD patients, a situation commonly observed also in non-BRICS nations. However, access to dedicated IBD databases, today an essential tool for IBD data collection, diagnosis, and treatment, 7 remained limited.
Essentially, all BRICS respondents had access to laboratory and technological resources. Most utilized noninvasive biomarkers like CRP and FC because of widespread availability in their countries, but, surprisingly, FC was underutilized despite its recognized value. Also surprising was the observation that many BRICS respondents had access to state-of-the-art cross-sectional imaging tools like MRE and CTE, which can offer a comprehensive view of the inflamed gastrointestinal tract, 8 but fewer had access to IUS despite being cheap, radiation-free, easy repetition, and a guide for therapeutic decisions. 9 A possible reason for the limited access to IUS is the lack of training and interpretation ability, as in the case of Brazil.
Notably, CTE and MRE were employed more frequently for CD than UC, likely because of limited confidence with the exams and the small number of expert centers. Thus, it appears that advanced technological tools like CTE and MRE, despite their high cost, are available to BRICS physicians in addition to traditional, cheaper, and noninvasive biomarkers like CRP and FC. These latter two biomarkers not only complement assessment of IBD clinical activity, but are recommended by STRIDE-II to reach the T2T goal of CRP and FC normalization, and can be superior to clinical and endoscopic outcomes for escalation of therapy, as shown by the CALM trial. 10
The majority of BRICS physicians had access to traditional (corticosteroids, immunomodulators) as well as modern medications (biologicals, including biosimilars), and prescribed nutritional support, probiotics, and traditional medicines in lower but still substantial proportions. Because IBD symptoms correlate poorly with endoscopic findings and recurrent inflammation can still be present despite MH, therapy intensification to achieve deep remission and reduce risk of disease progression and complications 11 was commonly considered by BRICS physicians. Most respondents supported the goal of achieving MH, TH, and HH in both UC and CD, a practice beyond the STRIDE consensus (endoscopic and clinical remission). 4 In particular, TH holds significant prognostic value, as it is an independent predictor and is linked to superior long-term clinical outcomes in CD. 12 In addition to MH, most BRICS respondents also supported HR as a long-term treatment goal for UC and CD since persistent histologic activity is associated with a higher risk of relapse, and normalization of HR can significantly reduce relapse rates in UC 13 but not necessarily in CD because of its patchy and transmural nature, even though some reports suggest so.14–16 In the IBD-PODCAST Spain study, most patients were treated according to STRIDE-II long-term treatment targets. However, a large proportion of patients still had suboptimal disease control after targeted immunomodulators, highlighting the gap between ideal treatment goals and real-world clinical outcomes. 17
Less experienced physicians were more likely to escalate treatment to achieve HR and accept the definition of complete deep healing compared to experienced physicians, which is consistent with previous evidence. Physicians in the earlier stages of their careers tend to be more strongly influenced by clinical practice guidelines and demonstrate greater adherence to standardized treatment goals.18,19 Conversely, experienced physicians might rely more on clinical judgment and individualized treatment decisions, prioritizing achievable and clinically meaningful endpoints over idealized but less feasible goals.19–21 Furthermore, gastroenterologists in China were more likely to escalate treatment than IBD specialists. This difference may be due to variations in clinical focus or treatment paradigms. 22
The conventional step-up approach refers to the initiation of corticosteroids and/or immunomodulators before biologics, a strategy endorsed by AGA and ECCO guidelines, particularly in UC.23,24 However, substantial evidence also supports a top-down (early use of biologics) approach in IBD.25–27 Most BRICS respondents preferred the top-down strategy for severe UC and CD, while more than half of Indian physicians supported a step-up therapy for severe UC.
The significant management challenges of IBD faced by physicians worldwide were also encountered by the BRICS respondents, who identified loss of response to medical therapy, fistulising perianal CD, and pregnancy-related complications as some of the most challenging. Interestingly, almost 90% of BRICS respondents listed psychological complications as a major IBD challenge, which is acknowledged but seldom considered a major therapeutic challenge by Western physicians, perhaps due to societal or cultural attitudes. Psychological comorbidities lower the QOL, whose restoration is important and a formal long-term target in the T2T algorithm.4,28,29
Despite some inherent limitations, the importance of endoscopy in IBD management is unquestionable for both diagnostic, treatment, and follow-up purposes, and BRICS physicians largely agreed on its use for achieving MH as a treatment goal. However, some disparities emerged, particularly the significantly lower value of achieving MH in UC reported by Indian physicians because of the aforementioned lack of robust RCT outcomes recommending the widespread implementation of MH in real-life clinical settings. 30 Most BRICS respondents reported intervals of 6 months to 1 year for endoscopic follow-up, which is notably different from the STRIDE-II guidelines (6–9 months).
Other endoscopic practices of BRICS physicians did not fully align with the STRIDE-II recommendations of a MES of 0 or UCEIS ⩽1 in UC and SES-CD <3 or absence of ulcerations in CD (Figure 5), which may lower the risk of clinical relapse, 31 predict steroid-free clinical remission, reduce corticosteroid need, hospitalizations, surgical interventions, IBD-related colorectal cancer, and improve QOL.32,33 Despite this cumulative evidence and the fact that the T2T approach is recognized as useful by BRICS respondents, individual experience and adoption of other types of recommendations (AGA, ECCO) appeared to strongly influence the real-word IBD practice in BRICS countries. A likely reason for this discrepancy is also the fact that the definition of MH has yet to be fully standardized and validated. 34 Finally, endoscopy invasiveness, need for sedation, risk of perforation or bleeding, inadequate bowel preparation, cost, and long waiting time for an endoscopy appointment were significant limiting factors for routine or follow-up endoscopy by BRICS physicians, a situation that likely affects negatively diagnosis and management decisions.
Tight monitoring and timely modifications using clinical symptoms and objective biomarkers yield better clinical and endoscopic outcomes compared to conservative symptom-based decisions alone and are also cost-effective. 35 An important component of tight IBD monitoring is TDM, which allows the optimization of thiopurines and biologics use.36,37 Despite its value, most BRICS respondents found obstacles in routinely using TDM, with high out-of-pocket costs being the biggest one. Moreover, only about half of them could measure serum levels of TNF-α and IFX. Thus, adequate monitoring of IBD patients may be suboptimal among BRICS respondents, due to the limited use of FC and TDM.
Overall, this multinational survey revealed that most physicians of BRICS countries are familiar with the T2T approach proposed by the STRIDE-II, but have variable and moderately strong confidence in its guidelines. Furthermore, if guidelines conflicted with personal clinical experience, BRICS physicians may not follow the STRIDE-II guidelines and use instead the AGA or ECCO recommendations or base decisions on their own personal experience. Some stated that it was difficult to remember specific guidelines or that the adoption of T2T guidelines was too challenging. So, despite the potential benefits of T2T in IBD, BRICS physicians also recognized its drawbacks and shortcomings.
There are various limitations in this study. First, although gastroenterologists from all five BRICS countries participated in this survey, over 80% of them were from China, so the results may be partially country-biased. Second, most (68.7%) of respondents worked in academic teaching hospitals, and the results of the survey may not represent those obtained in community or regional centers, a situation similar to that of Western nations. Third, the reported results are from five BRICS countries, which may or may not represent IBD management practices in other non-Western emerging countries, questioning the generalizability of the findings to other areas of the world. Finally, the survey may not reflect the actual real-world clinical practice in the BRICS countries, a reality that also occurs in Western countries. On the other hand, the BRICS survey also contains considerable strengths, like being the first to investigate whether and how hundreds of physicians trusted or adopted the STRIDE guidelines and implemented T2T strategies, and the first to identify the barriers to its implementation across different healthcare systems in non-Western BRICS nations.
Conclusion
This survey-based study demonstrated a relatively high confidence among BRICS physicians in the STRIDE-II consensus, even though BRICS countries display clear differences among them while sharing multiple socioeconomic and geopolitical similarities. Several obstacles were encountered in the everyday clinical practice of BRICS physicians, indicating a need to customize the STRIDE recommendations to the realities of each country to eliminate existing barriers and improve outcomes for IBD patients living in non-Western communities across the world.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848251383792 – Supplemental material for Gastroenterologists’ attitudes and challenges toward treat-to-target strategies in inflammatory bowel disease: a multinational survey
Supplemental material, sj-pdf-1-tag-10.1177_17562848251383792 for Gastroenterologists’ attitudes and challenges toward treat-to-target strategies in inflammatory bowel disease: a multinational survey by Zhilan You, Jun Shen, Vineet Ahuja, Gillian Watermeyer, Flavio Steinwurz, Marina Shapina, Claudio Fiocchi and Zhihua Ran in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-2-tag-10.1177_17562848251383792 – Supplemental material for Gastroenterologists’ attitudes and challenges toward treat-to-target strategies in inflammatory bowel disease: a multinational survey
Supplemental material, sj-pdf-2-tag-10.1177_17562848251383792 for Gastroenterologists’ attitudes and challenges toward treat-to-target strategies in inflammatory bowel disease: a multinational survey by Zhilan You, Jun Shen, Vineet Ahuja, Gillian Watermeyer, Flavio Steinwurz, Marina Shapina, Claudio Fiocchi and Zhihua Ran in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.