
Abstract
Background:
A yield pathological T0 (ypT0) classification usually indicates the pathologically complete response of rectal cancer to neoadjuvant therapy. However, lymph node metastasis may still be present.
Objectives:
In this study, we aimed to evaluate the prognostic value of residual lymph node status in patients with pathological T0 rectal cancer after neoadjuvant therapy.
Design:
Retrospective cohort study.
Methods:
Patients with locally advanced rectal cancer (LARC) who had undergone preoperative therapy and were pathologically classified as having ypT0 disease at Fudan University Shanghai Cancer Center between December 2012 and September 2022 were retrospectively analyzed. Uni- and multivariate analyses were performed to evaluate the effect of the residual lymph node status on disease-free survival (DFS) and overall survival (OS).
Results:
A total of 457 patients had ypT0 disease; this included 413 patients with ypT0N0 and 44 with ypT0N1–2. Inadequate lymph node retrieval (<12, p = 0.002) and adenocarcinoma (p = 0.009) were more common in the ypT0N0 group than in the ypT0N1–2 group. The ypT0N1–2 group showed marginal evidence of a higher probability of elevated pretreatment carcinoembryonic antigen levels and adjuvant chemotherapy than the ypT0N0 group (p = 0.076 and p = 0.077, respectively). Patients with ypT0N0 had significantly better 5-year DFS than those with ypT0N1–2 (84.8% vs 68.4%, p = 0.016). However, no significant difference was observed in the 5-year OS between the two groups (93.9% vs 88.8%, p = 0.602). Multivariate analysis revealed that residual lymph node status was an independent prognostic factor for DFS (hazard ratio, 2.285; 95% confidence interval: 1.246–4.192, p = 0.008).
Conclusion:
Residual lymph node metastasis may affect DFS, but not OS, in pathological T0 patients who receive neoadjuvant therapy followed by radical surgery for LARC.
Plain language summary
A yield pathological T0 (ypT0) classification describes the regression of rectal cancer after preoperative therapy. However, the lymph nodes may still contain cancer cells that can lead to recurrence. We examined whether the lymph node status in patients with pathological T0 rectal cancer after preoperative therapy affects survival. Patients with locally advanced rectal cancer (LARC) who had received preoperative therapy and were classified as having ypT0 disease were retrospectively analyzed. Uni- and multivariate analyses were performed to evaluate the effect of the residual lymph node status on disease-free survival (DFS) and overall survival (OS). Our findings suggest that residual lymph node metastasis may affect DFS, but not OS, in patients classified as ypT0 who receive preoperative therapy followed by radical surgery for LARC.
Introduction
Neoadjuvant chemoradiotherapy (CRT) followed by total mesorectal excision is recommended as the standard therapy for locally advanced rectal cancer (LARC). The combination of radio- and immunotherapy has recently shown promise in its treatment.1,2
After neoadjuvant therapy, approximately 20%–40% of patients with LARC achieve a pathologically complete response (pCR). 3 The long-term oncological outcomes in patients with LARC who achieve a pCR after neoadjuvant CRT are excellent. 4 Local excision has been attempted for the management of select patients with LARC who have achieved a good response to neoadjuvant CRT. If a pCR is achieved after neoadjuvant CRT and trans-anal excision, a “watch and wait” treatment strategy is adopted. 5 There is a concern that the mesorectal lymph nodes remain unresected. Despite complete regression of the primary rectal wall tumor (yield pathologic T0, ypT0), residual lymph node metastasis has been reported in a few cases and is a possible cause of tumor relapse. 6 Evidence indicates that remnant lymph node metastases after neoadjuvant CRT and surgery in patients with ypT0 rectal cancer indicate poor survival and are an important prognostic factor.7 –11 Previous studies have been hampered by two major limitations: (1) a small sample size, which may have undermined the statistical power and generalizability of the findings and (2) the focus on CRT, which potentially overlooks other neoadjuvant therapy regimens. The present study focuses on the incidence and long-term outcomes of lymph node metastasis in patients with ypT0 rectal cancer who had received different neoadjuvant treatments through a large-scale retrospective analysis.
Materials and methods
Design
This was a retrospective cohort study. It conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 12
Patients
Patients with LARC who received neoadjuvant CRT, short-course radiotherapy, chemotherapy with or without targeted therapy, or a combination of radiotherapy and immunochemotherapy followed by radical surgery and were pathologically confirmed as ypT0 (also called tumor regression grade 0, TRG 0) at the Fudan University Shanghai Cancer Center (FUSCC) between December 2012 and September 2022 were enrolled. Patients who had (1) histologically confirmed adenocarcinoma, mucinous adenocarcinoma, or signet ring cell carcinoma diagnosed before neoadjuvant therapy; (2) magnetic resonance imaging (MRI)-confirmed LARC without distant metastasis; (3) radical surgery; (4) postoperative pathology confirmed as ypT0; and (5) a follow-up of >1 year after neoadjuvant therapy were included. Patients were excluded if they had pathologically confirmed high microsatellite instability, squamous cell carcinoma, or neuroendocrine tumors. The following clinicopathological features were extracted from our database: age at diagnosis, sex, pretreatment carcinoembryonic antigen (CEA) level, histological type, interval between the initiation of neoadjuvant therapy and surgery, type of procedure, surgical approach, TRG score, cT stage, cN and pN stage, distance from the anal verge, MRI-based mesorectal fascia and extramural venous invasion status, number of lymph node harvests, adjuvant chemotherapy, and survival information. The initial clinical staging was based mainly on the MRI findings for rectal cancer.
Surgery
The surgeries followed standard procedures for total mesorectal excision. All surgeries were performed by colorectal surgeons who held the professional title of an associate chief physician or higher.
Statistical analysis
All statistical analyses were performed using SPSS (version 24.0; SPSS, Chicago, IL, USA). The Chi-square test was used to compare the categorical variables of the ypT0N0 and ypT0N1–2 groups. Survival analyses were performed using Kaplan–Meier analysis, and the log-rank test was used for univariate comparisons. Multivariate Cox regression analysis included variables with p < 0.1 in the univariate analysis. p < 0.05 was considered statistically significant.
Results
Patient characteristics
In total, 457 patients with ypT0 LARC were recruited for this study. Among them, 413 (90.4%) had ypT0N0 and 44 (9.6%) had ypT0N1–2 (Figure 1). Among those with ypT0N1–2, 37 (84.1%) had ypN1 and 7 (15.9%) had ypN2 disease. Patients with ypT0N1–2 had more signs of signet ring cell histology (p = 0.009), more lymph node harvest (p = 0.002), and showed marginal evidence of a higher probability of elevated pretreatment CEA levels and receiving adjuvant chemotherapy (p = 0.076, p = 0.077) than those with ypT0N0. No significant differences were observed in any other baseline characteristics (Table 1).
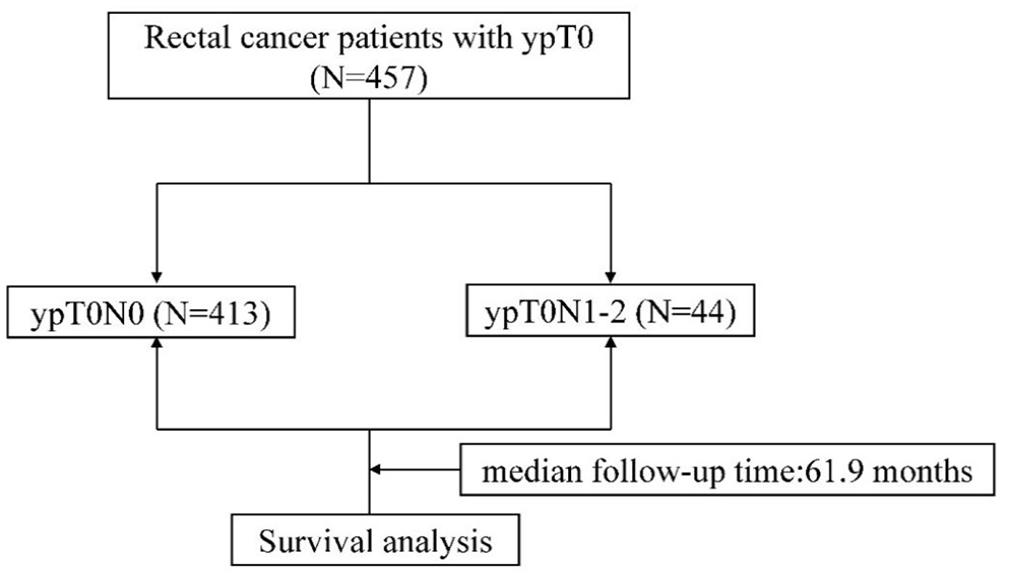
Workflow diagram.
Basic clinicopathological characteristics of patients with ypT0 rectal cancer.

Surgical interval: interval between the initiation of neoadjuvant therapy and surgery.
CEA, carcinoembryonic antigen; EMVI, extramural venous invasion; MRF, mesorectal fascia; ypT0, a yield pathological T0 classification.
Oncological outcomes
The median follow-up time was 61.9 months (range: 14–143 months). Tumor recurrence was observed in 76/457 patients (16.6%). A total of 33 patients died, of whom 32 died of tumor recurrence and 1 of pneumonia. The 5-year disease-free survival (DFS) rate was 84.8% for patients in the ypT0N0 group and 68.4% in the ypT0N1–2 group (p = 0.016; Figure 2(a)). However, no significant difference between the two groups was observed for overall survival (OS; 93.9% vs 88.8%, p = 0.602; Figure 2(b)). Univariate analysis showed that DFS was significantly associated with residual lymph node status and histological type in patients with ypT0 LARC. Multivariate analysis revealed that residual lymph node status and adjuvant chemotherapy were independent prognostic factors for DFS (hazard ratio (HR): 2.285; 95% confidence interval (CI): 1.246–4.192, p = 008; HR: 0.588, 95% CI: 0.353–0.977, p = 0.040; Table 2).

Kaplan–Meier survival curve for survival analysis in patients with ypT0 colorectal cancer treated with neoadjuvant treatment according to residual lymph node status. (a) Disease-free survival. (b) Overall survival.
Uni- and multivariate Cox analyses of the clinicopathological factors for DFS in ypT0 rectal cancer patients.

APR, abdominoperineal resection; CEA, carcinoembryonic antigen; CI, confidence interval; DFS, disease-free survival; EMVI, extramural venous invasion; HR, hazard ratio; MRF, mesorectal fascia; NI, not included; ypT0, a yield pathological T0 classification.
Discussion
pCR resulting from neoadjuvant CRT confers excellent survival in patients with rectal cancer. 4 Nonsurgical management is a valuable alternative to radical surgery in patients who achieve a clinically complete response. 13 However, the pCR of the primary tumor alone cannot accurately reflect the therapeutic response to neoadjuvant therapy. Primary tumors and mesorectal lymph nodes may respond differently to neoadjuvant CRT.14,15 In some cases, cancer cells remain in the lymph nodes even after complete response of the primary tumor. This can lead to recurrence if a watch-and-wait strategy is adopted.
In previous studies, lymph node metastasis was observed in 5%–16% of patients with rectal cancer who achieved pCR of the primary tumor.7 –11 Our study showed residual lymph node metastasis in 9.6% (44/457) of patients with primary tumors that completely regressed after neoadjuvant therapy, which is in accordance with previous findings. Unlike in previous studies, the neoadjuvant treatments used in our study were diverse.
Although more intensive adjuvant treatment was used in patients with ypT0N1–2 disease (86.4% vs 71.7%), the DFS was still lower than that in patients with ypT0N0 disease. In addition, a positive ypN status was an independent prognostic factor for DFS. This finding is consistent with those of previous studies emphasizing the prognostic value of nodal status in ypT0 rectal cancer after neoadjuvant treatment. By contrast, residual nodal involvement in patients with ypT0 disease often indicates poor lymph node regression. A few previous studies have reported that lymph node regression is associated with DFS in rectal cancer.16,17
Interestingly, no significant difference was observed in the OS of the two groups. This result contradicts previous reports in which OS was affected by residual lymph node status. Elshami et al. 18 reported that the development of ypT0N+ was associated with a lower 5-year OS than that of ypT0N0. Similarly, Erkan et al. 11 found that ypT0N+ status was independently associated with lower OS. Nevertheless, a notable shortcoming of their research was the failure to compare the DFS disparities between the two groups. In our study, the difference in DFS did not translate into a difference in OS. We speculate that patients who achieve complete regression of the primary rectal wall tumor may have better inherent biological tumor behavior and a good response to treatment. Even if recurrence or metastasis occurs, they remain sensitive to subsequent treatments, and OS is unaffected. Moreover, patients who achieve complete regression of primary rectal wall tumors have a high 5-year OS rate, and a longer follow-up period may be needed to observe differences in OS. As in our study, a study in the Republic of Korea 8 showed that ypN+ was a significant independent risk factor for recurrence, but no factors were associated with the 5-year OS.
The current study had certain limitations. First, as this was a retrospective study, it was inherently susceptible to selection bias, which may influence the generalizability of the findings. Second, the study encompassed a diverse array of neoadjuvant therapy regimens and lacked a focused exploration of any particular type of neoadjuvant therapy. This lack of concentration may have hindered a more in-depth analysis of specific effects and outcomes associated with a single well-defined neoadjuvant treatment regimen.
Residual lymph node metastasis may indicate poor DFS, but not OS, in patients with pathological T0 disease who have received neoadjuvant therapy followed by radical surgery for LARC.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251340494 – Supplemental material for Prognostic value of residual lymph node status in patients with pathological T0 rectal cancer after neoadjuvant therapy
Supplemental material, sj-docx-1-tag-10.1177_17562848251340494 for Prognostic value of residual lymph node status in patients with pathological T0 rectal cancer after neoadjuvant therapy by Dakui Luo, Zhen Wang, Yufei Yang, Qingguo Li and Xinxiang Li in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.