
Abstract
Background:
Clostridioides difficile infection (CDI) has emerged as a prevalent and recurrent antibiotic-associated infection. Fecal microbiota transplantation (FMT) is the most effective treatment for recurrent CDI (rCDI). Despite high success rates, FMT is ineffective in 5%–20% of cases. Factors associated with failure have not been clearly defined.
Objectives:
In this study, we seek to identify factors predictive of FMT failure.
Design:
Retrospective cohort study.
Methods:
A retrospective chart review was conducted on adult patients who were screened at the Complicated C. difficile Clinic at the University of Virginia Health System and received FMT for rCDI between 2013 and 2022. The primary outcome was failure of FMT, defined as either rCDI or all-cause death within 1 year.
Results:
In total, 240 patients underwent FMT: 70.4% were female, the median age was 68, and the median episode of CDI was 4. A total of 24.6% experienced failure within 1 year (18.3% had rCDI and 7.1% died). Age 70 or older (odds ratio (OR) = 2.66 (1.29–5.67)), ⩾4 episodes of CDI (OR = 3.13 (1.47–7.09)), and diabetes mellitus (OR = 2.82 (1.25–6.50)) were associated with failure on multivariate analysis.
Conclusion:
Our study shows that FMT remains an effective treatment for rCDI. We highlight several factors associated with FMT failure, such as older age, ⩾4 episodes of CDI, and diabetes mellitus, and the need for additional research to clearly define causality.
Plain language summary
Clostridioides difficile infection (CDI) is a common diarrheal infection associated with antibiotic use. It is commonly treated with antibiotics, and in patients with recurrent CDI (rCDI), fecal microbiota transplantation (FMT) is the most effective treatment. Despite high success rates, FMT is ineffective in 5–20% of cases. Factors associated with failure have not been clearly defined. In this study, we seek to better understand factors predictive of FMT failure. We conducted a retrospective chart review, looking at electronic medical records of 240 adult patients. All patients were screened at the Complicated C. difficile Clinic at the University of Virginia Health System and received FMT for rCDI between 2013 and 2022. The primary outcome was failure of FMT, defined as either rCDI or all-cause death within one year. Of the 240 patients who underwent FMT: 70.4% were female, median age was 68, and median episodes of CDI was 4. 24.6% experienced failure within the year (18.3% had rCDI and 7.1% died). Age 70 or older, ≥4 episodes of CDI, and diabetes mellitus were significantly associated with FMT failure. Our study shows that FMT remains an effective treatment for rCDI. We highlight several factors associated with FMT failure and the need for additional research to clearly define causality.
Introduction
Clostridioides (formerly Clostridium) difficile infection (CDI) has emerged as a common antibiotic-associated infection in the United States. With nearly 500,000 American patients diagnosed with CDI annually, implications extend beyond individual health, significantly impacting infection control and healthcare expenditures.1–4 5%–45% of patients with CDI experience recurrence, and in patients with recurrence, the risk of future recurrent CDIs (rCDI) increases to 60%.5–7 The main mechanism of rCDI is thought to be through decreased microbiome diversity leading to increased susceptibility to relapse or reinfection with C. difficile. 8 Fecal microbiota transplantation (FMT), which aims to restore the physiologic diversity of intestinal microbiota and resist colonization, has emerged as the most effective therapy for rCDI. 9 With success rates of 80%–95%, FMT has revolutionized rCDI treatment; guidelines recommend offering FMT to patients with rCDI who have failed antibiotic treatment.6,10–13 We have utilized FMT in our dedicated C. difficile clinic, which has outperformed antibiotic treatment, especially in patients who had three or more recurrent episodes. 14
Despite FMT’s high efficacy, FMT remains ineffective in 5%–20% of cases.5,10 Prior studies have highlighted potential associations between antidepressant use,15,16 cholecystectomy, 17 inpatient status, pseudomembranes, immunocompromised status, 18 and FMT failure, but definitive risk factors for FMT failure remain poorly understood. 10 In this study, we evaluate the efficacy of FMT in the treatment of rCDI and identify factors that may contribute to FMT failure.
Methods
The research protocol was approved by the Institutional Review Board at the University of Virginia (IRB-HSR#23045, FMT). As this is a descriptive study of patients who are undergoing treatment recommended by IDSA guidelines, no hazardous procedures or chemicals are involved. The privacy rights of human subjects have been observed. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 19 The study flow diagram is outlined in Figure 1.

Study flow diagram.
Study setting, study design, and data collection
We conducted a retrospective cohort study of patients aged 18 or older evaluated for rCDI at the Complicated C. difficile Clinic (CCDC) at the University of Virginia Health System and treated with FMT between 2013 and 2022. The CCDC is a referral clinic attended by a multidisciplinary team including gastroenterologists and infectious diseases physicians. 20 The interdisciplinary team held conferences, as needed, to review criteria and discuss patients who were immunocompromised or medically complex. Initial evaluation included an extensive history and comprehensive laboratory testing, detailed in Table 1, regardless of symptomatology or medical history. We had no clinical exclusion criteria; patients with underlying gastrointestinal (GI) disorders, such as inflammatory bowel disease and irritable bowel syndrome (IBS), were not excluded if CDI episodes were appropriately documented. All eligible patients who received FMT at the CCDC were included in the study. Electronic medical records were reviewed for demographic information, GI medical history, other medical history, surgical history, CDI history, labs within 1 month before FMT, and follow-up data. Data were entered into a secure REDCap (Research Electronic Data Capture) database.
Laboratory studies ordered at the initial visit.

FMT procedure and patient follow-up
Patients were eligible for FMT if they had experienced three or more CDI episodes despite appropriate treatment, or severe, complicated CDI. Donor stool was obtained from either a directed donor (family and friends, n = 45; first cohort of patients) or a universal donor (prescreened and purchased from OpenBiome, n = 195 (Boston, MA, USA)). FMT was performed by depositing donor stool in the colon via colonoscopy, and biopsies were obtained at the discretion of the gastroenterologist. If the patient had pseudomembranes, colonoscopy with FMT was repeated until no pseudomembranes (indicative of CDI) were visualized on colonoscopy as previously recommended 21 (Figure 2). After FMT, patients were instructed to contact the clinic if they had recurrent diarrhea or concern for rCDI.
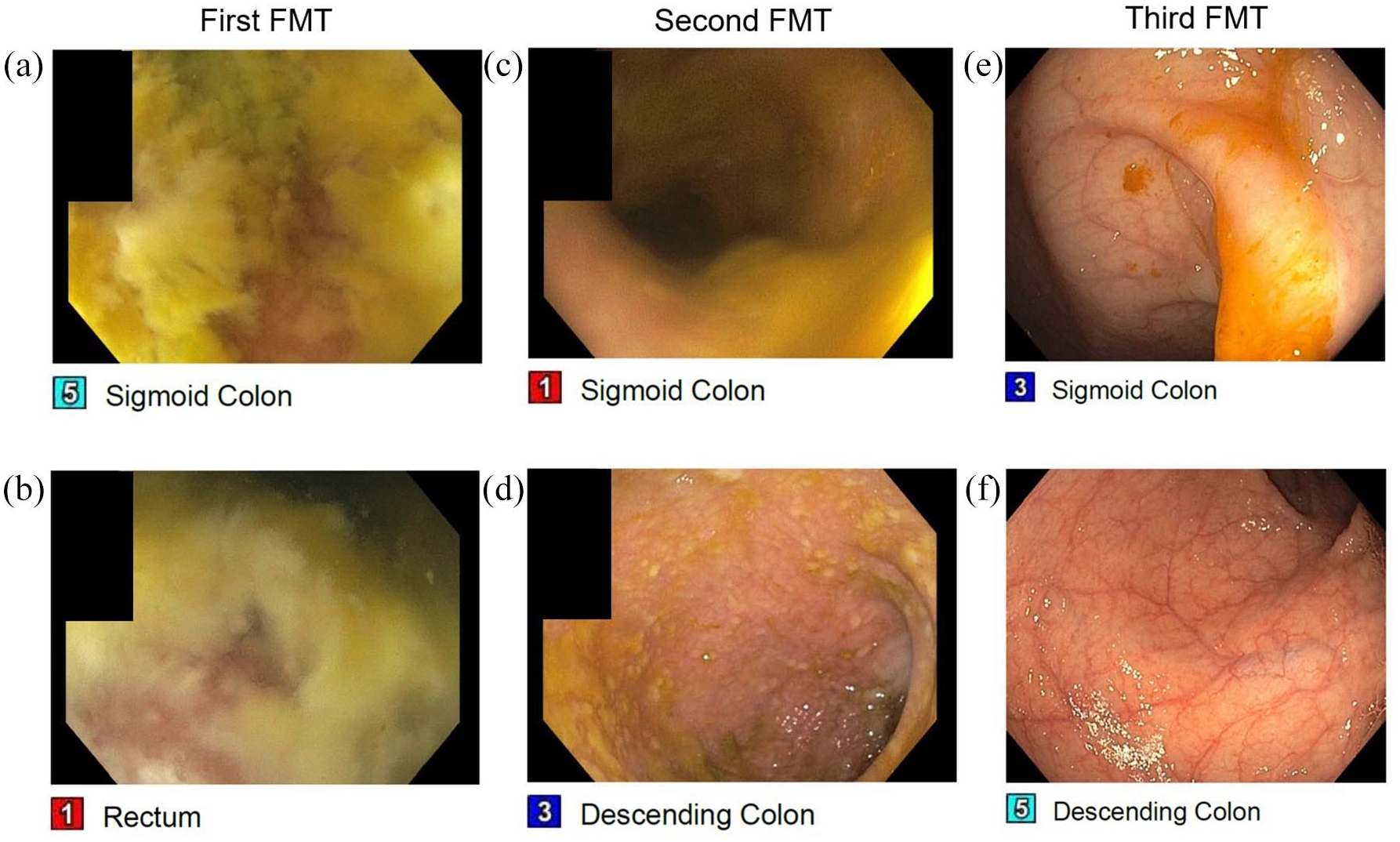
Colonoscopic findings from one patient show edematous mucosa and pseudomembranes present throughout the sigmoid colon (a) and rectum (b) during the first FMT. On the second FMT (5 days after the first FMT), there is some improvement in the sigmoid colon (c) and the scope was advanced to the descending colon which revealed still significant pseudomembranes (d). On the third FMT (2 weeks after the first FMT), except for a congested proximal rectum, the rest of the examined colon, including both the sigmoid colon (e) and the descending colon (f) exhibited resolution of pseudomembranes and healthy intestinal epithelium.
Study outcomes
The primary outcome was FMT failure, defined as recurrence of CDI or death from any cause within 1 year of FMT (or both outcomes in series). Recurrence was defined as the return of diarrhea (liquid/loose stool ⩾3 per day) with a stool sample testing positive for C. difficile. Though recurrence may occur multiple times, only the first instance was counted. Prior to February 2020, testing for C. difficile at our institution was initially done by toxin B gene polymerase chain reaction (PCR; Xpert Cepheid, Sunnyvale, CA, USA); it was subsequently changed to a stepwise testing protocol consisting of multistep toxin B gene PCR with reflex, if PCR positive, to C. difficile toxin B enzyme immunoassay, with both results submitted to the treating clinician. Testing outside our institution was not uniform, but CDI episodes were recorded based on the documented clinical diagnostic decision of the treating physician. Recurrence and death were divided into early (<3 months after FMT) and late (3–12 months after FMT).
Statistical analysis
Chi-square analysis and t-test were used for univariate analysis, and a multivariate binomial logistic regression model was used for multivariate analysis. Variables analyzed were age, sex, CDI, psychiatric conditions, use of biologics, prior cholecystectomy, hypertension, diabetes mellitus, gastroesophageal reflux disease (GERD), hyperlipidemia, malignancy, immunosuppression, IBS, Crohn’s disease, ulcerative colitis, and diverticulitis. Laboratory values were not included in the multivariate model due to incomplete documentation. All tests were two-tailed, and a p-value cutoff of 0.05 was used. Statistical analyses were performed with R, version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
In total, 240 patients with rCDI were treated with FMT at our facility from 2013 to 2022. Baseline characteristics of patients are reported in Table 2. A total of 70.4% of patients were female and the median age was 68 years (range: 20–96), with 47.5% of patients 70 or older. The median number of reported CDIs was 4 (range: 1–25), with 62.1% of patients experiencing four or more infections. 14.8% of patients had more than one FMT. 24.6% of patients experienced FMT failure, 18.3% of patients experienced recurrence, and 7.1% of patients died within 1 year of FMT (Figure 3(a)). Of the 18 patients who died, 8 had a documented cause of death: failure to thrive (2), end-stage renal disease (2), infection (2), malignancy (1), and ileus (1).
Demographics, comorbidities, and labs of patients by outcome.

CDI, Clostridioides difficile infection; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Hgb, hemoglobin; TSH, thyroid-stimulating hormone; WBC, white blood cell count.
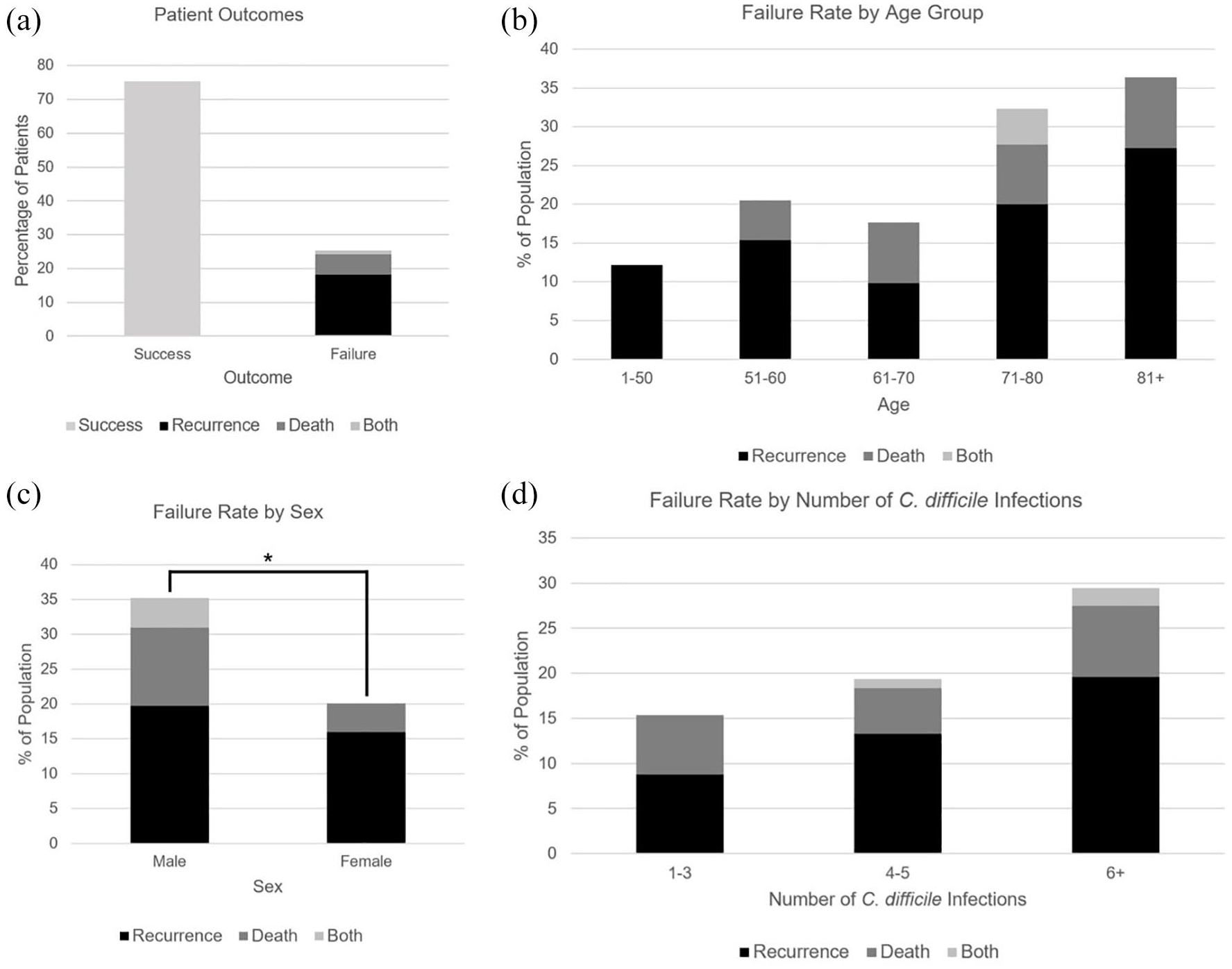
Rate of success and each adverse outcome (a), recurrence, death, and failure rate by age group (b), recurrence, death, and failure rate by sex compared with univariate analysis (c), and recurrence, death, and failure rate by number of Clostridioides difficile infections (d). No comparison was performed across groups in (a), (b), and (d).
In univariate analysis (Table 3), age 70 or older (Figure 3(b), 32% vs 17%, p = 0.007), male sex (Figure 3(c), 35% vs 14%, p = 0.013), and four or more CDIs (Figure 3(d), 30% vs 15%, p = 0.010) were significantly associated with FMT failure. Regarding comorbidities, hypertension (29% vs 14%, p = 0.010), diabetes mellitus (40% vs 20%, p = 0.0025), and malignancy (34% vs 21%, p = 0.034) were associated with FMT failure, while GERD (p = 0.31), hyperlipidemia (p = 0.94), and immunosuppressive conditions or medications (p = 0.13) were not (Figure 4(a)). Ethnicity (p = 0.24), psychiatric conditions (p = 0.097), use of GABAergic psychiatric medications (p = 0.97), use of non-GABAergic psychiatric medications (p = 0.58), biologic treatments (e.g., monoclonal antibodies; p = 0.47), and prior cholecystectomy (p = 0.43) were also not associated with FMT failure. Regarding lab values, we found that high thyroid-stimulating hormone (TSH, 82% vs 23%, p = 2.70e), low hemoglobin (Hgb, 39% vs 19%, p = 0.0024), and low zinc (37% vs 21%, p = 0.025) were associated with FMT failure (Figure 4(b)).
Univariate analysis of the association between clinical, demographic, and laboratory factors and recurrence, death, and failure.

p-Values (*p < 0.05, **p < 0.01) and ORs with 95% confidence intervals are listed in the table.
Value could not be computed as zero patients experienced recurrence with low IgA.
CDI, Clostridioides difficile infection; CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; GERD, gastroesophageal reflux disease; IBS, irritable bowel syndrome; OR, odds ratio; TSH, thyroid-stimulating hormone; WBC, white blood cell count.

(a) Recurrence, death, and failure rate by presence versus absence of comorbidities compared with univariate analysis. (b) Recurrence, death, and failure rate by abnormal versus normal lab values compared with univariate analysis.
When breaking down failure into recurrence and death, recurrence was associated with age 70 or older (25% vs 13%, p = 0.018), four or more CDI (24% vs 9%, p = 0.0028), hypertension (22% vs 10%, p = 0.021), and high TSH (63% vs 19%, p = 6.35e−4). Death was associated with male sex (15% vs 4%, p = 0.0023), diabetes mellitus (16% vs 5%, p = 0.0045), high TSH (27% vs 5%, p = 0.0032), low Hgb (17% vs 3%, p = 0.00097), and low zinc (15% vs 3%, p = 0.0039). No association was seen between recurrence or death and ethnicity, psychiatric conditions, cholecystectomy, GERD, or immunosuppression.
In total, 17% of patients experienced FMT failure early (within 3 months; 13.8% recurrence, 3.8% death). Of the 44 patients who recurred, 33 recurred early (75%) and 11 recurred late (25%). Age 70 or older (p = 0.046), four or more CDI (p = 0.03), hypertension (p = 0.014), and high TSH (p = 2.83e−4) were associated with early recurrence (compared to patients who recurred late or did not recur). Four or more CDI (p = 0.029) continued to be associated with late recurrence (compared to patients who did not recur).
Multivariate analysis (Table 4) revealed that age 70 or older (odds ratio (OR) 2.66 (1.29–5.67)), four or more CDI (OR 3.13 (1.47–7.09)), and diabetes mellitus (OR 2.82 (1.25–6.50)) were associated with failure while age 70 or older (OR 2.34 (1.08–5.24)) and four or more CDI (OR 3.63 (1.57–9.40)) were associated with recurrence.
Multivariate analysis of the association between clinical and demographic factors and recurrence, death, and failure.

p-Values (*p < 0.05, **p < 0.01, ***p < 0.001) and ORs with 95% confidence intervals are listed in the table.
CDI, Clostridioides difficile infection; CI, confidence interval; GERD, gastroesophageal reflux disease; IBS, irritable bowel syndrome; OR, odds ratio.
Discussion
rCDI remains a formidable challenge in clinical practice. Our cohort of 240 patients experienced an FMT success rate (i.e., no recurrence or death) of 83% over 3 months and 75% over 1 year, with a no-recurrence rate of 86% over 3 months and 82% over 1 year. This is in line with documented success rates (80%–95%) when taking into account that most prior studies examined recurrence only (not death), and most only recorded recurrence within 1–3 months.10,15,22,23 By expanding the study window and accounting for both recurrence and death, our study captures multiple factors that may not be seen with one outcome or a shorter study window. Nonetheless, our overall FMT success rate highlights the consistency and high efficacy of FMT in rCDI. Expanding on our prior study’s findings, 20 our study found the following factors to be associated with either failure, recurrence, or death: age 70 or older, male sex, four or more CDI, hypertension, diabetes mellitus, malignancy, high TSH, low hemoglobin, and low zinc. Compared to our prior work, this study features a larger patient cohort, an analysis of both recurrence and death as endpoints (independently and together), and a comprehensive analysis of many demographic, clinical, and laboratory risk factors.
Age over 70 is a well-documented risk factor for CDI and FMT failure, possibly due to comorbidities, including immunosuppression.22,24,25 However, even when controlling for comorbidities, age was an independent risk factor for FMT failure, a finding that has been corroborated in other studies. 14 Two hypotheses for this finding include the following: (1) age-related microbiome changes (shown to resemble antibiotic use in younger patients),16,23,26 decreasing microbiome resistance to colonization and engraftment of the beneficial FMT microbiome and (2) deficient host immune response to FMT. Studies have shown that FMT can induce a global host immune response, possibly explaining its efficacy in treating rCDI. 15 This is mediated by innate lymphoid cell type 2 16 and regulatory T cells (Treg) 23 through interferon-gamma 27 and Th17 responses. 28 Although an age-related deficiency in these mechanisms has not been demonstrated, analysis of immune responses in older patients in response to FMT would help elucidate these potential mechanisms.
Male sex was also associated with FMT failure in our cohort, particularly death. Previous studies have shown associations between female sex and FMT failure, 29 female sex and initial CDI,11,30 female sex and rCDI, 31 and male sex and death and severe complicated CDI. 31 Although only the last finding was seen in our cohort, it is notable that the proportion of women in the cohort was high (70.4%) and in line with previous studies (62%). 29 Future directions include further analysis of potential confounders (e.g., increased antibiotic use in women due to more frequent urinary tract infections 32 ) and bench studies regarding the mechanism of sex-related differences.
Medical comorbidities associated with FMT failure on univariate analysis included hypertension, diabetes mellitus, and malignancy, the first of which is a novel finding. On the other hand, diabetes mellitus has been shown to increase the risk of initial CDI 33 and rCDI. 34 While diabetes is associated with many infections, the association of both hypertension and diabetes mellitus may suggest an underlying metabolic contributor to FMT failure. Western diet, which is high in fat, has been associated with worse outcomes with CDI in animal models, 24 while a diet high in fiber was associated with a lower risk of CDI. 35 An exploration of diet in association with the success or failure of FMT may be informative. Regarding malignancy, its primary contribution to failure was through increased deaths, although few malignancy-related deaths were explicitly documented. Malignancy has previously been associated with rCDI 36 and death from CDI.37–39 Decreased immunity is thought to be an important contributor to this association, 40 but an alteration of the microbiome by chemotherapy is also considered a possible mechanism. 41 Interestingly, we found a negative association between recurrence and history of diverticulitis (4.8% prevalence in patients with recurrence, 14.1% in patients without recurrence), but relatively few patients (30/240) had a history of diverticulitis and this association did not extend to death or failure. In addition, while psychiatric conditions 39 and immunosuppression (conditions or medications)33–35 have previously been associated with FMT failure, 42 we did not observe these associations in our cohort. We also unexpectedly observed a moderate protective association between psychiatric conditions and death (5.0% prevalence in patients who died, 12.0% in patients who did not die), though we did not observe an association between psychiatric conditions and FMT recurrence or failure. However, the associations between FMT outcomes and diverticulitis and psychiatric conditions did not persist following multivariate adjustment.
A number of CDI episodes independently predicted FMT failure; specifically, patients with four or more episodes were more likely to have an unsuccessful FMT. While this may be reflective of a greater degree of dysbiosis in patients with more episodes of CDI, 8 it also suggests that recurrence may be driven by factors not cured by FMT. Although it is unclear whether a higher number of CDI episodes directly contributes to FMT failure (as opposed to there being a different underlying cause for both increased CDI episodes and FMT failure), this finding suggests that lowering the threshold for switching from antibiotic treatment to FMT may be beneficial in some patients. 43
In addition to comorbidities, we studied lab values within 1 month prior to FMT. Low Hgb has been linked to FMT failure, a trend reaffirmed in this study. 9 Elevated erythrocyte sedimentation rate (ESR), an inflammatory marker, was numerically higher in patients in our cohort with FMT failure. The combination of low Hgb and high ESR may suggest the presence of anemia of chronic disease, a potential indicator of chronic inflammation. Chronic inflammation may be either a symptom of dysbiosis 44 or the cause of dysbiosis, 45 or both, which may contribute to FMT failure.
Previous studies have indicated a correlation between zinc deficiency and FMT failure, which was seen in our cohort. 46 Patients afflicted with rCDI are susceptible to zinc deficiency due to diarrhea and anorexia associated with active CDI. Zinc has been shown to have antidiarrheal effects due to its ability to enhance water and electrolyte absorption, which aids in mucosal integrity, brush border enzyme activity, and immunity. Zinc has also been shown to play a potentially important role in sustaining a diverse microbiome. 46 Finally, decreased zinc levels may be a marker of intestinal inflammation, which may contribute to FMT failure.
A novel finding that emerged from this study is the association between elevated TSH and FMT failure. It is unclear whether elevated TSH reflects true clinical hypothyroidism, as reflex-free T4 levels were rarely obtained in our cohort. In the existing literature, case reports have shown an association between CDI and decreased TSH, but not increased TSH.31,47 We present several hypotheses for this association. First, hypothyroidism is known to decrease gut motility. While this may be beneficial after FMT to increase the effects of treatment and maximize interaction between the donor stool and the recipient microbiota, 30 it may worsen CDI and contribute to recurrence by retaining bacteria and toxins. Second, it is possible that elevated TSH reflects a hypothyroid phase in thyroiditis, although this is less likely due to its transient nature (while patients receiving FMT are chronically ill). Third, elevated TSH may be a manifestation of other underlying conditions associated with FMT failure. Finally, advanced age may contribute to elevated TSH; in our cohort, patients with normal or low TSH had a median age of 68, while patients with high TSH had a median age of 75.
Strengths of this study include the following: (1) consistent and standardized procedures and documentation, as all patients received FMT and an infectious diseases consultation at our institution, (2) easily quantifiable endpoints, such as recurrence and death, and (3) relatively long follow-up period of 1 year. Limitations of this study include the following: (1) possible confounding bias, stemming from unrecognized factors not controlled for, (2) clinically subjective indications for FMT and no documentation of CDI severity, leading to within-cohort differences that may be difficult to quantify, (3) incomplete documentation (i.e., not all patients received all pre-FMT blood tests), (4) non-uniform post-FMT management (e.g., no documentation on suppressive antibiotics), and (5) limitations of retrospective cohort studies, including this one, to generating hypotheses rather than making definitive conclusions or determining causality. Given the focus on clinical parameters that are more readily available for clinicians in the real-world setting, microbial or metabolic biomarkers that may predict FMT outcomes were not studied in this paper. The complexity of the gut microbiota and its variability across both healthy and disease–host conditions remain challenging but warrant further studies to identify potential biomarkers that could indicate either the success or failure of microbiota transplantation in the future.
Conclusion
Our study has identified several factors that may be associated with failure of FMT in the treatment of rCDI, including age over 70, four or more CDIs, and diabetes mellitus. FMT remains a highly efficacious treatment for rCDI; at 1-year follow-up, about three in four patients who underwent FMT did not have rCDI or death. Awareness of demographic and comorbid factors associated with FMT success can better inform care for patients undergoing FMT for rCDI. Future directions include expanding the cohort, prospective studies evaluating causality, and exploring mechanisms underlying the associations uncovered in this study.