
Abstract
Background:
Despite its significant health burden, there is a lack of national-level temporal patterns in gastrointestinal bleeding (GIB) mortality.
Objectives:
To comprehensively decipher the annual and monthly trend of GIB-related mortality in the United States.
Design:
Cross-sectional study.
Methods:
We analyzed the National Vital Statistic System database, which documents more than 99% of the annual deaths in the United States for GIB-related deaths from January 2010 to May 2023. Annual and monthly age-standardized mortality rates were estimated and categorized by age, sex, and bleeding site. Joinpoint regression was performed for trend analysis. Prediction modeling was conducted to determine the GIB-associated excess mortality.
Results:
A total of 529,094 and 210,641 GIB-associated deaths occurred before and after 2020, respectively. Following a stably decreasing trend between 2010 and 2019, there was an excess mortality rate during the pandemic which peaked in 2021. The monthly mortality trend showed spikes corresponding to the outbreak of variants. Importantly, excess GIB-related mortality resolved in 2023, with the convergence of predicted and observed mortality rates. Subgroup analysis showed that young males (aged 19–44 years) were affected the most during the pandemic, with excess mortality rates of 35.80%, 52.77%, and 31.46% in 2020, 2021, and 2022, respectively. While the increasing trend of upper GIB was accentuated during the pandemic, lower GIB showed a reversal of the pre-pandemic decreasing trend.
Conclusion:
Our findings demonstrate the trend of GIB-related mortality, underscoring an increased excess death during the pandemic followed by a resolution in 2023. We identify subpopulations vulnerable to the pandemic.
Plain language summary
Why was the study done? While the COVID-19 pandemic has incurred substantial gastrointestinal (GI)-related excess mortality, the detailed temporal trends throughout the pandemic’s duration remain unclear. What did the researchers do? Using a nationwide mortality database, we identified deaths related to GI bleeding that occurred between January 2010 and May 2023. What did the researchers find? A total of 529,094 and 210,641 GI bleeding-associated deaths occurred before and during the pandemic, respectively. The annual excess mortality rate peaked in 2021 and declined in 2022. The monthly mortality trend showed spikes corresponding to the outbreak of new variants. Importantly, excess GI bleeding-related mortality resolved in 2023, with the convergence of predicted and observed mortality rates. Subgroup analysis showed that young males (aged 19-44 years) were affected the most during the pandemic, with excess mortality rates of 35.80%, 52.77%, and 31.46% in 2020, 2021, and 2022, respectively. While the increasing trend of upper GI bleeding was accentuated during the pandemic, lower GI bleeding showed a reversal of the pre-pandemic decreasing trend. What do the findings mean? Our findings demonstrate the resolution of excess GI bleeding-related mortality in 2023 and identify subpopulations vulnerable to the pandemic. It has implications for policymakers in addressing the current pandemic and preparing for future pandemics.
Keywords
Introduction
The COVID-19 pandemic has left an indelible mark on healthcare worldwide and the United States. 1 Extensive evidence has underscored the significance of not only the direct morbidity and mortality attributable to the virus but also the indirect, multifaceted consequences of the pandemic on a broad range of medical conditions.2–4 There has been systematic evolution of the healthcare system to enhance resilience and sustain this impact. Although the United States has declared the end of public health emergency in May 2023, there is a dearth of up-to-date evidence to assess how far we have achieved.
Gastrointestinal bleeding (GIB), a medical emergency, has a 28-day case fatality rate of 7% for upper GIB and 0.4% for lower GIB. 5 A delay in care would likely have a negative impact on patient prognosis. During the COVID-19 pandemic, a myriad of factors conspired that may have impacted the incidence and outcomes of patients with GIB. Foremost among these is the susceptibility of the gastrointestinal system to SARS-CoV-2 infection given the presence of critical molecules, including ACE2 receptors, TMPRSS2, and Furin, throughout the gastrointestinal tract. 6 Observational studies have also revealed a proclivity for GIB among patients hospitalized with COVID-19.7,8 The research indicates a combined prevalence of 3.05% for COVID-19 and GIB, while the estimated overall prevalence of patients undergoing anticoagulant or antiplatelet therapy is 6.2%. 9 Hypothesized mechanisms include the formation of stress ulcers, hemorrhagic colitis possibly secondary to SARS-CoV-2, medication-induced bleeding from the use of anticoagulants and corticosteroids, and/or bleeding secondary to disseminated intravascular coagulation. 10 Indirect effects, such as the stay-at-home mandates, reallocation of medical resources, and cancellation of outpatient clinics and endoscopic procedures, also played a substantial role. 11
There is heterogeneity in the reported incidence of GIB among COVID-19 patients, with figures ranging from 0.47% to 19% in a systematic review. 9 Further confounding this association is the conflicting data regarding the mortality associated with GIB in the context of COVID-19, which is also limited by small sample sizes derived from hospitalized patients.12,13 Additionally, despite considerable adaptive strategies being implemented to improve the use of endoscopy and patient triage, the trend of GIB-related mortalities through May 2023 remains unclear. In light of this, an up-to-date population-based study examining the trends of GIB-related mortality is warranted.
In this study, we aimed to evaluate the trends in mortality associated with GIB, particularly focused on data through the end of the public health emergency, May 2023, to provide insights into the evolving pandemic and its bearing on conditions that require immediate attention such as GIB. Using a nationwide, population-based database and robust categorization, we aimed to provide a comprehensive overview of mortality trends and identify vulnerable subpopulations.
Methods
Study design and data source
We conducted a cross-sectional, observational study analyzing de-identified death data sourced from the National Vitals Statistics System (NVSS), encompassing January 1, 2010 through May 30, 2023. The NVSS, an initiative of the Centers for Disease Control and Prevention (CDC), collates and processes death certificate data from all 50 states as well as the District of Columbia, capturing information pertaining to >99% of decedents in the United States.
The provided data include demographic information (i.e., age, sex, and race/ethnicity) as well as the cause of death, which is documented using the record axis and the entity axis. The NVSS employs two distinct axes for cause-of-death documentation, namely the record axis and the entity axis. For the purposes of this study, causes of death were ascertained from the record axis, which constitutes a synthesized and refined iteration of the entity axis, thus providing a more unequivocal categorization. 14
Given the public availability and de-identified nature of the dataset under analysis, an exemption was sought from Institutional Review Board approval. This study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental Material). 15
Definitions
International Classifications of Diseases-Tenth Revision (ICD-10) codes were used in defining the diagnoses associated with the causes of death (Supplemental Table 1). Diagnosis of GIB was categorized based on the anatomical position of the bleeding. Upper and lower GIBs were defined using the ligament of Treitz. As many patients with GIB at the initial presentation may eventually die from other causes of death, we defined all decedents with GIB diagnoses listed as either primary or other causes of death on the death certificate as GIB-related deaths.
Temporal and demographic stratification
We defined the beginning of the pandemic as April 2020. To better assess the temporal trends of mortality during the pandemic, the pandemic epoch was segmented into distinct intervals reflecting the prevailing SARS-CoV-2 variant. Accordingly, the period from March 2020 through December 2020 was designated as “Wildtype,” succeeded by “Alpha” from December 2020 to June 2021, “Delta” from June 2021 to November 2021, and “Omicron” from November 2021 to May 2023.
Age stratification was operationalized using predefined categories: 19–44 years, 45–64 years, and 65 years or above. Categorization according to type (upper and lower GI tract) was defined using the ICD-10 code.
Statistical analysis
The demographic characteristics of decedents with GIB were analyzed and presented as frequencies along with their respective percentages. The crude mortality rate was computed by dividing the annual number of GIB-related deaths by the total U.S. population for the corresponding year.
To account for the differences in age distribution among the population, we calculated the age-standardized mortality rates (ASMRs). The ASMR, shown as per 100,000 persons, was computed using the direct standardization method. This method involves multiplying the age-specific mortality rates by the number of persons in each age group of the standard population, and then summing these products to get the total number of “expected” deaths in the standard population. The ASMR is then calculated by dividing the total expected deaths by the total standard population and multiplying by 100,000. The 2000 U.S. Census Standard Population was used as the reference population for the calculation of ASMR.
We performed a forecast analysis to predict annual and monthly GIB-associated ASMRs during and after the pandemic. Pre-pandemic data were used as the reference for these predictions. Several models, including Autoregressive Integrated Moving Average Model, Autoregressive Moving Average Model, polynomial linear regression, and Prophet, were tested to select the one with the best fit for the pre-pandemic data. Excess mortality was calculated as the percentage difference between the observed and predicted ASMRs. This measure provides an estimate of the additional mortality associated with GIB during the pandemic, beyond what would have been expected based on pre-pandemic trends.
Joinpoint analysis was used to identify points in time where the trend in GIB-associated ASMR changed significantly. This method fits a series of connected straight lines to the ASMRs. A permutation test is used to identify “joinpoints,” or points where the trend changes significantly. The test iteratively adds joinpoints to the model until no more statistically significant joinpoints are detected, resulting in a model that accurately represents the trend over time, including significant shifts.
Subgroup analyses were conducted by age, sex, and location of GIB (upper and lower). We also performed stratified analyses by age and sex groups to further explore potential interactions between these factors.
Results
Study population and characteristics
Between 2010 and 2022, a total of 713,570 GIB-associated deaths occurred in the United States (Supplemental Table 2). The majority were elderly (73.0%). Death rates were evenly distributed between both sex groups. Deaths associated with lower GIB (70%) outnumbered those with upper GIB (30.0%). There were 26,165 GIB-related deaths that occurred between January 1 and May 31, 2023. This cohort was included in the analyses of monthly but not annual mortality.
Overall analysis of GIB-related mortality
Prior to the pandemic, between 2010 and 2019, there was no significant change in GIB-related ASMR (Figure 1(a); Supplemental Figure 1). During the pandemic, however, GIB-related mortality significantly increased. In 2020, the observed ASMR (16.84 per 100,000 persons) was 13.33% higher than the predicted (14.86) (Table 1, upper panel). The excess mortality increased to 27.96% in 2021 and then decreased to 21.02% in 2022. Importantly, the proportion of COVID-19-associated deaths among all excess deaths gradually decreased from 45.8% in 2020 to 32.0% in 2022 (Supplemental Figure 2(A)).

Temporal trend for ASMRs of gastrointestinal bleeding-related death in the United States. (a) Annual ASMR. Shaded areas denote the difference between the observed and predicted ASMRs for 2020–2022. (b) Monthly ASMR. Periods of outbreaks secondary to wild-type SARS-CoV-2 and its variants were denoted as different color-shaded areas.
Excess death and APC in ASMRs of gastrointestinal bleeding-related death in the United States 2010–2022, total, by age, sex and location.

Joinpoint analysis identifies points in the trend where significant changes occur, suggesting the optimal segmentation (length and number of segments) to explain the observed data pattern. Therefore, if an increasing trend happened before the pandemic, the joinpoint suggested by the analysis would not be at the beginning of the pandemic.
The formula of this proportion is (Observed ASMR – Predicted AMSR)/Predicted AMSR.
p < 0.05. **p < 0.01.
APC, annual percentage changes; ASMRs, age-standardized mortality rates; CI: confidence interval.
When monthly data were analyzed, overall ASMR persistently increased from the onset of the pandemic until late 2022, with intermittent surges that corresponded to outbreaks of new variants, especially early outbreaks secondary to the alpha and omicron variants (Figure 1(b)). Notably, after the initial increase in ASMR in January and February of 2022, excess deaths down trended the remainder of 2022, except for an increase in summer and the end of the year. In 2023, excess mortality trends reversed to negative values. (Supplemental Table 3).
GIB-related mortality by age and sex
Despite no statistical significance, the pre-pandemic trend of GIB-related mortality in the older adults experienced a gradual decline, while the mortality trends in groups 19–44 years and 45–64 years exhibited a slight upward trend (Figure 2(a); Supplemental Figure 3(A)–(C)). During the pandemic, the increase in GIB-related mortality was most profound among young adults (19–44 years), with a 46.17% excess death in 2021, followed by a drop to 24.81% in 2022 (Table 1, middle panel). The annual percentage change (APC) between 2018 and 2022 was the highest among the young adults, at 16.3% (95%CI: 7.7%–25.6%), compared to 7.0% (95%CI: 3.0%–11.1%) among adults aged 45–64 years. There was a nonsignificant APC among the elderly. While the proportion of COVID-19-related mortality reduced in 2022 among decedents aged 45 years and older, the 19-to-44-year-old group experienced an increased proportion of COVID-19-related deaths throughout the pandemic (Supplemental Figure 4(A)–(C)).

Annual trend for ASMRs of gastrointestinal bleeding-related death in the United States. The shaded area in yellow color in both panels denotes the pandemic. (a) By age. Shaded areas in orange, red, and green colors denote the difference between the observed and predicted ASMRs for age groups 19–44 years, 45–64 years, and ⩾65 years, respectively. (b) By sex. Shaded areas in blue and red colors denote the difference between the observed and predicted ASMRs for males and females, respectively.
The male population exhibited higher GIB-related ASMR than females during 2010–2022 (Figure 2(b); Supplemental Figure 5(A)–(B)). While both sex groups demonstrated similar fluctuation in trends during the pandemic, male decedents with GIB exhibited higher excess mortality rates than their female counterparts (16.16%, 32.33%, and 23.19% in males vs 10.73%, 24.56%, and 20.65% in females; Table 1, bottom panel). For both sexes, the proportion of COVID-19-related mortality among the excess deaths decreased each year (Supplemental Figure 6(A)–(B)).
When stratified by both age and sex, males aged 19–44 years were most affected, with 35.80%, 52.77%, and 31.46% excess deaths in 2020, 2021, and 2022, respectively. (Supplemental Figures 7 and 8(A)–(D); Supplemental Table 4). Despite a decrease in the proportion of COVID-19-related deaths of excess mortality from 15.5% in 2021 to 14.2% in 2022 (Supplemental Figure 9(A)–(F)), this subgroup presented the highest APC between 2018 and 2022 (17.4%, 95%CI: 8.3%–27.1%). By contrast, females aged ⩾65 years saw a decreasing trend before the pandemic, followed by significantly increased mortality during the pandemic (Supplemental Table 4). Elderly females experienced high proportions of COVID-19-related death of excess mortality during the pandemic (64.5%, 36.0%, and 31.9% in 2020, 2021, and 2022, respectively; Supplemental Figure 9(A)–(F)).
GIB-related mortality by location
With a nonsignificant change before the pandemic, upper GIB-related death trends increased significantly during the pandemic (Figure 3; Supplemental Figure 10(A) and (B)), as evidenced by an excess mortality of 8.34%, 12.92%, and 11.42% in 2020, 2021, and 2022, respectively (Table 1, lower panel). By contrast, lower GIB-related mortality trends experienced a significant decrease before the pandemic, with an APC of −2.0% (95%CI: −2.8 to −1.2%, p < 0.001) between 2010 and 2018. During the pandemic, there was a deviation from the decreasing trend. The ASMR increased and the proportions of excess mortality increased from 1.21% in 2020 to 11.37% in 2021, followed by a reduction to 5.63% in 2022.

Annual trend for ASMRs of gastrointestinal bleeding-related death in the United States by the location of bleeding. The shaded area in yellow color in both panels denotes the pandemic. Shaded areas in orange and blue colors denote the difference between the observed and predicted ASMRs for the upper and lower gastrointestinal tracts, respectively.
GIB-related mortality by causes of death
The excess mortality for all etiologies of GIB increased from 2020 to 2021 (Figure 4; Supplemental Table 5). Diverticular diseases appeared to be the conditions with the highest excess mortality, followed by peptic ulcer disease, inflammatory diseases, and vascular disorders. Notably, the etiology of the majority of GIB-related mortality was not specified.
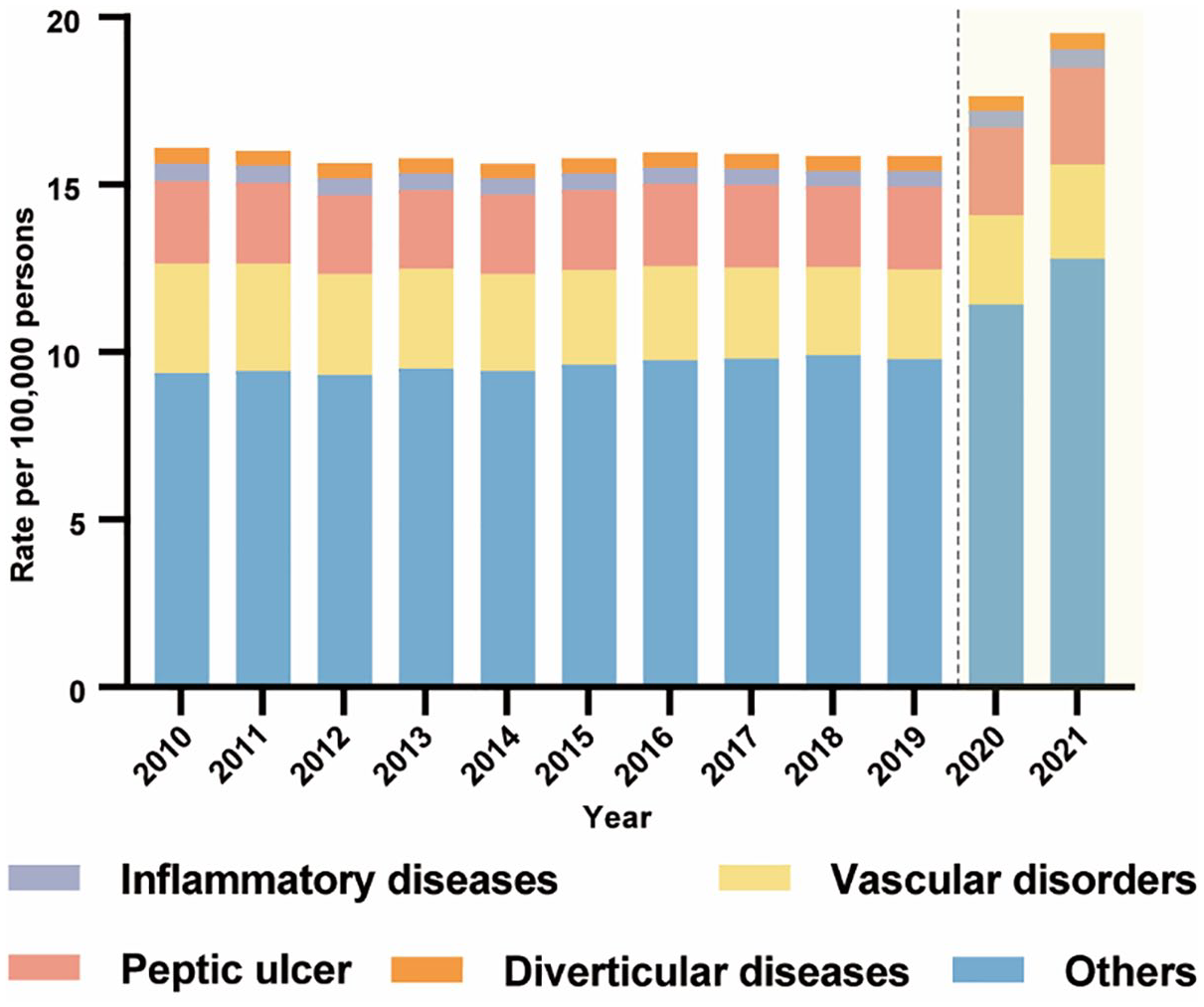
Annual trend for ASMRs of gastrointestinal bleeding-related death in the United States by the etiologies of bleeding. The shaded area in yellow color in both panels denotes the pandemic. The definition of each etiology is elucidated in Supplemental Table 1.
Discussion
In this study, we examined GIB-related mortality trends before and through the end of the COVID-19 pandemic. Our findings revealed a temporal association between the surge in GIB-related mortality and the outbreak of different COVID-19 variants during the early stages of the pandemic. Notably, the termination of the federal COVID-19 public health emergency declaration in May 2023 resulted in negligible GIB-related excess mortality. Our comprehensive categorizations revealed that males aged 19–44 years were the most affected demographic, with the highest excess deaths from 2019 through 2022. Interestingly, while upper GIB saw an even greater increase following a decade-long up trend before the pandemic, lower GIB experienced a reversal of longstanding pre-pandemic decreasing trend.
Our results showing the rise of GIB-related mortality during the pandemic align with prior studies, which showed the pandemic led to a decrease in the number of hospital visits due to interruptions in transport and fear of infection exposure, potentially leading to delayed care and poorer outcomes. A nationwide study from the United States reported a 9.5% reduction in total GIB-related admissions but a 13% increase in mortality among these patients in 2020. 16 Two cohort studies reported lower hemoglobin among patients with GIB compared to those in the pre-pandemic period.17,18 Similarly, another study reported fewer emergency department visits for GIB during the pandemic, but with a higher proportion of inpatient admissions and severe GIB among these patients. 19 Additionally, our findings are consistent with the broader impacts of the pandemic on healthcare systems worldwide. The fear of contracting the virus, coupled with the policies and restrictions imposed to curb the transmission, led to a significant reduction in hospital visits for non-COVID-19-related conditions. 20 This is particularly concerning for conditions such as GIB, which require timely intervention to prevent worse outcomes.
Furthermore, the diminished probability of receiving timely endoscopic hemostasis intervention could potentially lead to increased mortality. The nature of the virus and its modes of transmission have rendered GI endoscopy, an essential tool in managing GIB, a high-risk procedure.13,21 This categorization, along with competition for resources such as personal protective equipment, may have prompted a trend toward more conservative initial management, potentially leading to delayed treatment and poorer outcomes.16,22
The decrease in excess death late in the pandemic may be attributed to the evolution of the medical system’s response to the pandemic. The restructuring of public healthcare systems, implementation of protective protocols for patients and healthcare staff, increasing uptake of vaccinations, provision of effective drugs and equipment, and expansion of ICU capacity and staffing pool have all played a role. 23 For patients with GIB, the strategies to enhance the chance of receiving an endoscopy are crucial. Vanella et al. highlighted the importance of maintaining COVID-free environments, systematic testing and triage of patients, and prioritizing procedures based on urgency. The authors also emphasized the need for minimal standard protective equipment and re-evaluation of trainee involvement in procedures. 24 Moreover, Nguyen et al. presented a model for reopening endoscopy suites using a tier-based system for the safe reintroduction of elective procedures while minimizing transmission to patients and staff. 25 The adoption/modification of such models and measures may have contributed to the recovery of excess death observed in our study.
Another potential reason for the decrease in excess mortality observed in our study is the reduced severity of GIB as we approached the end of the pandemic. This could be attributed to the mitigated fear of exposure to the SARS-CoV2 infection and the digital transformation in healthcare, which included the upgrade of health record systems and registries, and the evolution of telemedicine. The increased volume of telemedicine has allowed for early-stage care of diseases. 26 For instance, patients with mild peptic ulcer disease or esophageal varices could be treated promptly with conservative medical interventions, thereby reducing the risk of developing GIB.
Immunization coverage has also made significant contributions to the decrease in excess mortality rates. Newly emerged variants like Delta or Omicron demonstrate strong immune evasion capabilities against neutralizing antibodies induced by initial vaccination or prior infections.27,28 Many countries are offering COVID-19 booster shots, which have significantly reduced hospitalizations and deaths related to COVID-19, thereby enhancing protection against the disease. 29
Our study found that males, especially those aged 19–44 years, were most affected. This aligns with a nationwide study that reported a 15.8% increase in mortality among men (p = 0.007), compared to a 4.7% increase among women (p = 0.059). 16 The higher baseline prevalence of GIB in males and the likelihood of young males delaying seeking medical attention could explain this disparity. 30 Consistently, males also demonstrated vulnerability to other acute diseases that required immediate treatment during the pandemic. For example, a prior nationwide study showed that young males had the highest increasing trends of acute myocardial infarction-related death. 31 In most countries, males account for a higher proportion of confirmed COVID-19 cases and deaths compared to females. It is possible that females possess an advantage in their immune system, exhibiting stronger innate and adaptive immune responses than males. This could potentially be attributed to the high concentration of immune-related genes located on the X chromosome. 32 The COVID-19 pandemic has significantly impacted mental health. Studies indicate that men face a higher risk of mental disorders compared to women, and young people are more prone to developing psychopathological disorders compared to other age groups. This may be attributed to factors such as income, education level, knowledge about the pandemic, and confidence in combating the pandemic.33,34 Social support can help reduce the risk of psychological distress. In order to alleviate the impact of the pandemic on vulnerable populations, society should be ready to take supportive actions including efforts to improve social integration, reduce loneliness, and assist isolated individuals in maintaining contact with the outside world. Other strategies can also include investment in remote mental health interventions to provide high-quality remote counseling for those suffering from depression and anxiety under home confinement orders.
Limitations
Our study leveraged a nationwide dataset comprising of greater than 99% of all deaths in the United States with comprehensive and up-to-date information on GIB-related mortality. The relatively long period included in the study prior to the pandemic allowed us to develop predictive models with high accuracy, which facilitated the estimation of excess mortality. Furthermore, the large sample size allowed for extensive subgroup analyses and yielded information to determine subpopulations or clinical conditions that were vulnerable. We also acknowledge the limitations of this study. First, the mortality data from NVSS lack certainty regarding the direct attribution of GIB mortality to the COVID-19 pandemic and lack laboratory and procedural data. Therefore, the scope of this study focused on the epidemiology but not the clinical management of GIB-related mortality. Death certificate data essentially reflect the priorities and subjectivity of healthcare professionals, who are prone to making errors in recording, coding, and incorrectly attributing potential and contributing causes of death. Although NVSS is robust, there are still potential biases in discussing data related to death certificate data, which limit the fidelity of our data and require us to interpret the results with caution. Second, subgroup information for 2023 mortality data is not available at the time of analysis. Updated analysis of the trends in 2023 is warranted. Third, this database contained a limited number of variables, which makes performing in depth analysis of factors associated with these trends not possible. Hence, additional research is essential to identify and assess potential risk factors contributing to high mortality rates in young men, including stress-related factors such as economic stress, poor mental health, and social influences. Finally, this database did not provide discharge diagnosis; thus, the focus of this study is on the mortality burden and excess death, but not incidence of GIB during the pandemic.
Conclusion
In conclusion, our study provides an encouraging trend of GIB-related mortality through the end of the pandemic. The study also highlights the need for targeted interventions for vulnerable groups, such as young males. Lessons learned from the comprehensive analyses of these trends can help adapt healthcare strategies to mitigate the impact of future health crises.
Supplemental Material
sj-docx-1-tag-10.1177_17562848241311006 – Supplemental material for Increased gastrointestinal bleeding-related mortality during the COVID-19 pandemic
Supplemental material, sj-docx-1-tag-10.1177_17562848241311006 for Increased gastrointestinal bleeding-related mortality during the COVID-19 pandemic by Xu Gao, Yee Hui Yeo, Fan Lv, Xinyuan He, Justin Park, Jamil Samaan, Yunyu Zhao, Wee Han Ng, Jinhai Wang, Fanpu Ji and Gil Y. Melmed in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.