
Abstract
Background:
Acute variceal bleeding (AVB), a life-threatening complication of liver cirrhosis, can be effectively treated by endoscopy, but there is a risk of early rebleeding after endoscopic variceal treatment (EVT). Thrombocytopenia is the most common hemostatic abnormality in liver cirrhosis. However, it is still unclear about whether thrombocytopenia increases the failure of EVT in cirrhotic patients with AVB.
Objectives:
We investigated the association between thrombocytopenia and the failure of EVT in cirrhotic patients with AVB.
Design:
International multicenter, retrospective study.
Methods:
Overall, 2467 cirrhotic patients with acute gastrointestinal bleeding who were enrolled into an international multicenter study between September 30, 2020 and June 30, 2023 were retrospectively screened. Thrombocytopenia was defined as platelet count below 150 × 109/L and further classified as mild (100 × 109/L–150 × 109/L), moderate (50 × 109/L–100 × 109/L), and severe (<50 × 109/L). A 1:1 propensity score matching (PSM) analysis was performed. Five-day failure to control bleeding was evaluated.
Results:
Overall, 1079 patients were included, of whom 923 (85.5%) had thrombocytopenia, including mild (n = 241), moderate (n = 445), and severe (n = 237) thrombocytopenia. PSM analysis demonstrated that the rate of 5-day failure to control bleeding was not significantly different between patients with and without thrombocytopenia (mild: (12/153) 7.8% vs (7/153) 4.6%, p = 0.236; moderate: (9/155) 5.8% vs (7/155) 4.5%, p = 0.608; or severe: (5/132) 3.8% vs (7/132) 5.3%, p = 0.555).
Conclusion:
Thrombocytopenia may not influence the efficacy of EVT in cirrhotic patients with AVB.

Plain language summary
Introduction
Acute variceal bleeding (AVB) is a common and life-threatening complication of liver cirrhosis, which accounts for approximately 70% of acute gastrointestinal bleeding (AGIB) events.1,2 AVB is attributed to the rupture of gastroesophageal varices secondary to portal hypertension. 3 In spite of advances in diagnosis and treatment, the 6-week mortality of cirrhotic patients with AVB remains 15%–20%. 4 Additionally, recurrent bleeding is frequent, ranging from 30% to 40% within the subsequent 6 weeks after an initial AVB episode, especially the first 5 days. 5 Currently, endoscopic variceal treatment (EVT), together with medical therapy, is the golden standard for the management of AVB, 6 but the incidence of failure to control bleeding within the initial 5 days after EVT is as high as 10%–15%.7,8
Thrombocytopenia is the most common hemostatic abnormality occurring in cirrhosis. The pathogenesis of thrombocytopenia is multifactorial, including decreased synthesis of thrombopoietin, splenic sequestration of platelets secondary to portal hypertension, myelosuppression, and increased destruction of platelets. 9 The prevalence and degree of thrombocytopenia is in parallel with the severity of cirrhosis. Approximately 80% of cirrhotic patients with Child-Pugh class B and C have thrombocytopenia, with a majority presenting with moderate thrombocytopenia. 10
Current evidence remains very scarce about the association of thrombocytopenia with treatment failure of EVT in cirrhotic patients with AVB. To the best of our knowledge, only three previous studies have explored the association between platelet (PLT) count and short-term outcomes of cirrhotic patients with AVB after EVT. A prospective cohort study found that PLT was not significantly different between patients who failed to control bleeding after endoscopy and those who did not. 11 But the confounding factors were not adjusted in this study, which may influence the statistical validity of the results. Similarly, another two previous studies also demonstrated that PLT was not significantly different between patients who developed early rebleeding and those who did not.12,13 However, the number of patients included in a study by Chau et al. 12 was very limited. Furthermore, all of them did not stratify the patients according to the severity of thrombocytopenia.11 –13
Herein, we aimed to further explore the association of thrombocytopenia with 5-day failure to control bleeding after EVT in cirrhotic patients with AVB, based on the data from an international multicenter study.
Methods
Study design
We retrospectively screened the data of cirrhotic patients with AGIB who were enrolled into an international multicenter observational study between September 30, 2020 and June 30, 2023 (NCT04662918). 14 Exclusion criteria were as follows: (i) patients who did not undergo endoscopy; (ii) patients who were not diagnosed with variceal bleeding on endoscopy; (iii) patients who did not undergo EVT; and (iv) patients who underwent splenectomy, liver transplantation, or transjugular intrahepatic portosystemic shunt. The study protocol was approved by the Medical Ethical Committee of the General Hospital of Northern Theater Command with an ethical approval number (Y (2024) 139) and was carried out following the rules of the 1975 Declaration of Helsinki. Patients’ informed consents were waived. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 15
The following baseline data were collected: demographics, etiology of liver cirrhosis, decompensated complications at admission, and laboratory tests (i.e., white blood cell (WBC), PLT, prothrombin time (PT), and international normalized ratio (INR)). Child-Pugh score and Model for End-Stage Liver Disease (MELD) score at admission were calculated. According to the data collected in this study, EVT primarily included endoscopic variceal ligation (EVL), endoscopic cyanoacrylate glue injection (ECGI), and endoscopic injection sclerotherapy (EIS). Drugs mainly included vasoactive drugs (i.e., octreotide, somatostatin, and terlipressin), proton pump inhibitors, and antibiotics. Blood transfusions mainly included PLT, red blood cell (RBC), and fresh frozen plasma (FFP).
Patients were divided according to the presence of thrombocytopenia. Thrombocytopenia was defined as PLT <150 × 109/L and further classified as mild (100 × 109/L–150 × 109/L), moderate (50 × 109/L–100 × 109/L), and severe (<50 × 109/L).10,16 The outcome of interest in this study was the rate of 5-day failure to control bleeding, which was defined according to the Baveno VII consensus. 6
Statistical analyses
All statistical analyses were performed with IBM SPSS 25.0 (IBM Corp., Armonk, NY, USA) and Stata/SE 12.0 (Stata Corp., College Station, TX, USA). Continuous variables were expressed as mean ± standard deviation and median (range) and compared using the independent sample t-test or nonparametric Mann–Whitney U test. Categorical variables were expressed as frequency (percentage) and were compared using the Chi-squared test or Fisher’s exact test. Logistic regression analyses were conducted to explore whether thrombocytopenia was significantly associated with the risk of 5-day failure to control bleeding after EVT. Crude odd ratios (cORs) with their 95% confidence intervals (CIs) were calculated in univariate analyses. Adjusted odd ratios (aORs) with their 95% CIs were calculated in multivariate analyses after adjusting for age, gender, blood transfusions (i.e., PLT, RBC, and FFP), Child-Pugh score, and MELD score. A 1:1 propensity score matching (PSM) analysis was performed to match baseline characteristics between patients with and without thrombocytopenia. Matching factors included age, gender, blood transfusions (i.e., PLT, RBC, and FFP), Child-Pugh score, and MELD score. A two-tailed p < 0.05 was considered statistically significant.
Results
Patients
A total of 1079 patients were included (Figure 1), of whom 923 (85.5%) had thrombocytopenia, including mild (n = 241), moderate (n = 445), and severe (n = 237) thrombocytopenia. Patient characteristics are summarized in Table 1. The median age was 57 years (range: 19–92), and 762 (70.6%) patients were male. Hepatitis B virus infection (52.9%) was the most common etiology of liver cirrhosis followed by alcohol abuse (16.6%). Among them, 684 (63.4%) patients had ascites at admission, and 635 (58.9%) had history of variceal bleeding. The median Child-Pugh score and MELD score were 7.00 (range: 5.00–15.00) and 12.14 (range: 6.43–40.00), respectively. The rate of 5-day failure to control bleeding was 5.2% (n = 56/1079).
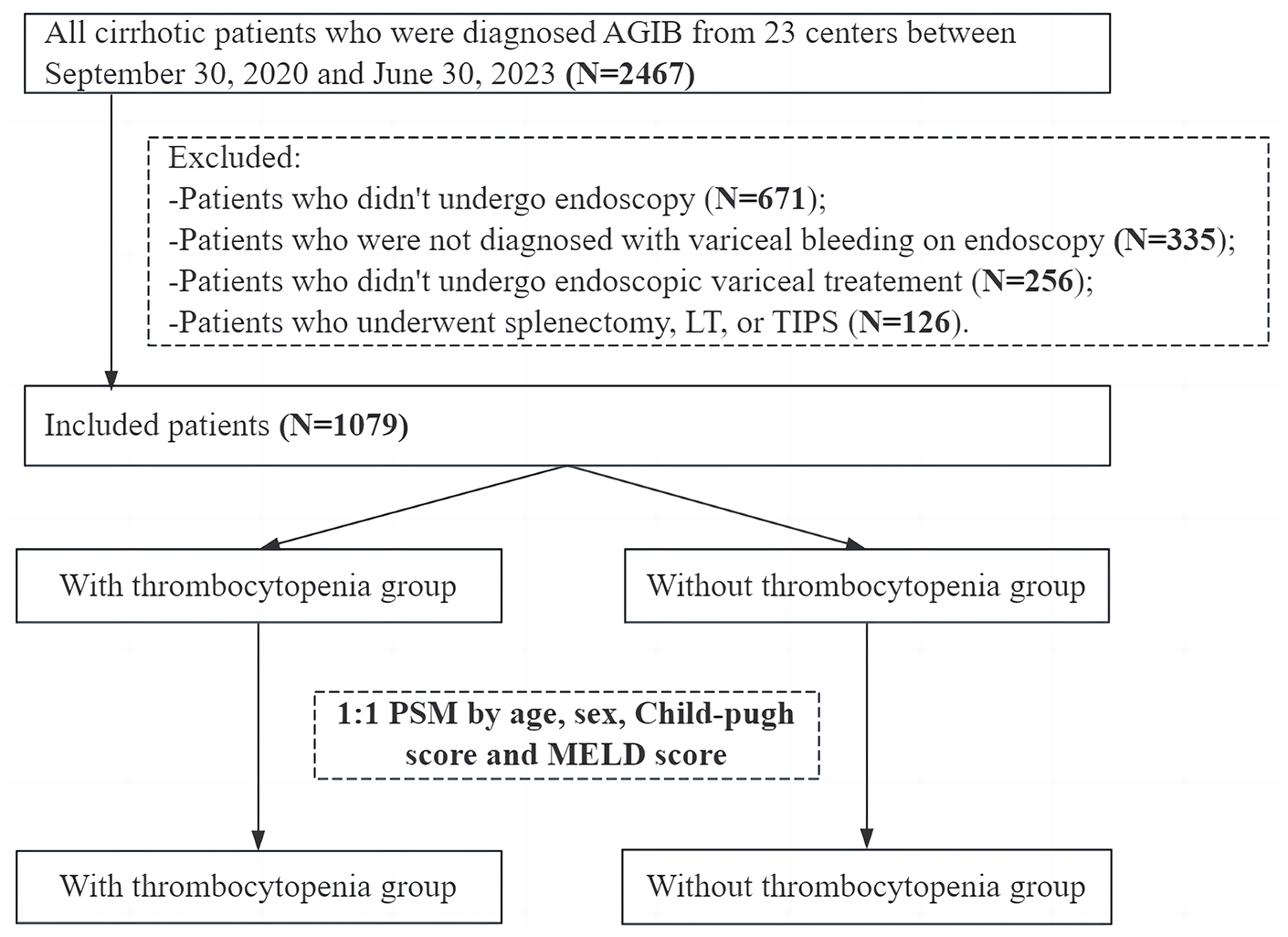
Flowchart of patients’ screening and grouping.
Baseline characteristics of the study cohort.

ACLF, acute-on-chronic liver failure; ALB, albumin; ECGI, endoscopic cyanoacrylate glue injection; EIS, endoscopic injection sclerotherapy; EV, esophageal varices; EVL, endoscopic variceal ligation; FFP, fresh frozen plasma; GV, gastric varices; HB, hemoglobin; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HE, hepatic encephalopathy; INR, international normalized ratio; MELD, model for end-stage liver disease; No. Pts, number of patients; PLT, platelet; PPIs, proton pump inhibitors; PT, prothrombin time; RBC, red blood cell; Scr, serum creatinine; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell.
Mild thrombocytopenia versus normal PLT
In the overall analysis, patients with mild thrombocytopenia had significantly higher prevalence of esophageal varices (EV) (98.3% vs 94.9%, p = 0.049), but lower WBC (7.06 × 109/L vs 9.44 × 109/L, p < 0.001) than those with normal PLT. However, the rate of 5-day failure to control bleeding was not significantly different between the two groups (5.4% vs 4.5%, p = 0.687; Table 2). Univariate logistic regression analysis showed that the presence of mild thrombocytopenia was not independently associated with the rate of 5-day failure to control bleeding (cOR = 1.214, 95% CI = 0.473–3.112, p = 0.687). Multivariate logistic regression analysis showed that the presence of mild thrombocytopenia was not independently associated with the rate of 5-day failure to control bleeding (aOR = 1.713, 95% CI = 0.618–4.748, p = 0.300).
Overall analysis and PSM analysis between patients with mild thrombocytopenia and normal PLT.

The values in bold mean statistically significant.
ACLF, acute-on-chronic liver failure; ALB, albumin; ECGI, endoscopic cyanoacrylate glue injection; EIS, endoscopic injection sclerotherapy; EV, esophageal varices; EVL, endoscopic variceal ligation; FFP, fresh frozen plasma; GV, gastric varices; HB, hemoglobin; HBV, Hepatitis B Virus; HCC, hepatocellular carcinoma; HCV, Hepatitis C Virus; HE, hepatic encephalopathy; INR, international normalized ratio; MELD, model for end-stage liver disease; No. Pts, number of patients; PLT, platelet; PPIs, proton pump inhibitors; PSM, propensity score matching; PT, prothrombin time; RBC, red blood cell; Scr, serum creatinine; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell.
In the PSM analysis, 153 patients were matched to each group. Patients with mild thrombocytopenia had significantly lower WBC (7.42 × 109/L vs 9.46 × 109/L, p < 0.001) than those with normal PLT. However, the rate of 5-day failure to control bleeding was not significantly different between the two groups (7.8% vs 4.6%, p = 0.236; Table 2).
Moderate thrombocytopenia versus normal PLT
In the overall analysis, patients with moderate thrombocytopenia had significantly higher total bilirubin (TBIL) (35.53 μmol/L vs 29.72 μmol/L, p < 0.001), PT (15.98s vs 15.39 s, p = 0.023), INR (1.39 vs 1.34, p = 0.011), prevalence of EV (98.0% vs 94.9%, p = 0.044), and gastric varices (GV) (73.9% vs 59.0%, p < 0.001), but lower WBC (5.35 × 109/L vs 9.44 × 109/L, p < 0.001) than those with normal PLT (Table 3). However, the rate of 5-day failure to control bleeding was not significantly different between the two groups (5.8% vs 4.5%, p = 0.522). Univariate logistic regression analysis showed that the presence of moderate thrombocytopenia was not independently associated with the rate of 5-day failure to control bleeding (cOR = 1.321, 95% CI = 0.562–3.107, p = 0.524). Multivariate logistic regression analysis showed that the presence of moderate thrombocytopenia was not independently associated with the rate of 5-day failure to control bleeding (aOR = 1.384, 95% CI = 0.567–3.380, p = 0.476).
Overall analysis and PSM analysis between patients with moderate thrombocytopenia and normal PLT.

The values in bold mean statistically significant.
ACLF, acute-on-chronic liver failure; ALB, albumin; ECGI, endoscopic cyanoacrylate glue injection; EIS, endoscopic injection sclerotherapy; EV, esophageal varices; EVL, endoscopic variceal ligation; FFP, fresh frozen plasma; GV, gastric varices; HB, hemoglobin; HBV, Hepatitis B Virus; HCC, hepatocellular carcinoma; HCV, Hepatitis C Virus; HE, hepatic encephalopathy; INR, international normalized ratio; MELD, model for end-stage liver disease; No. Pts, number of patients; PLT, platelet; PPIs, proton pump inhibitors; PSM, propensity score matching; PT, prothrombin time; RBC, red blood cell; Scr, serum creatinine; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell.
In the PSM analysis, 155 patients were matched to each group. Patients with moderate thrombocytopenia had significantly higher TBIL (40.05 μmol/L vs 29.87 μmol/L, p = 0.004), prevalence of GV (70.3% vs 59.4%, p = 0.043), but lower WBC (5.48 × 109/L vs 9.44 × 109/L, p < 0.001) than those with normal PLT. However, the rate of 5-day failure to control bleeding was not significantly different between the two groups (5.8% vs 4.5%, p = 0.608; Table 3).
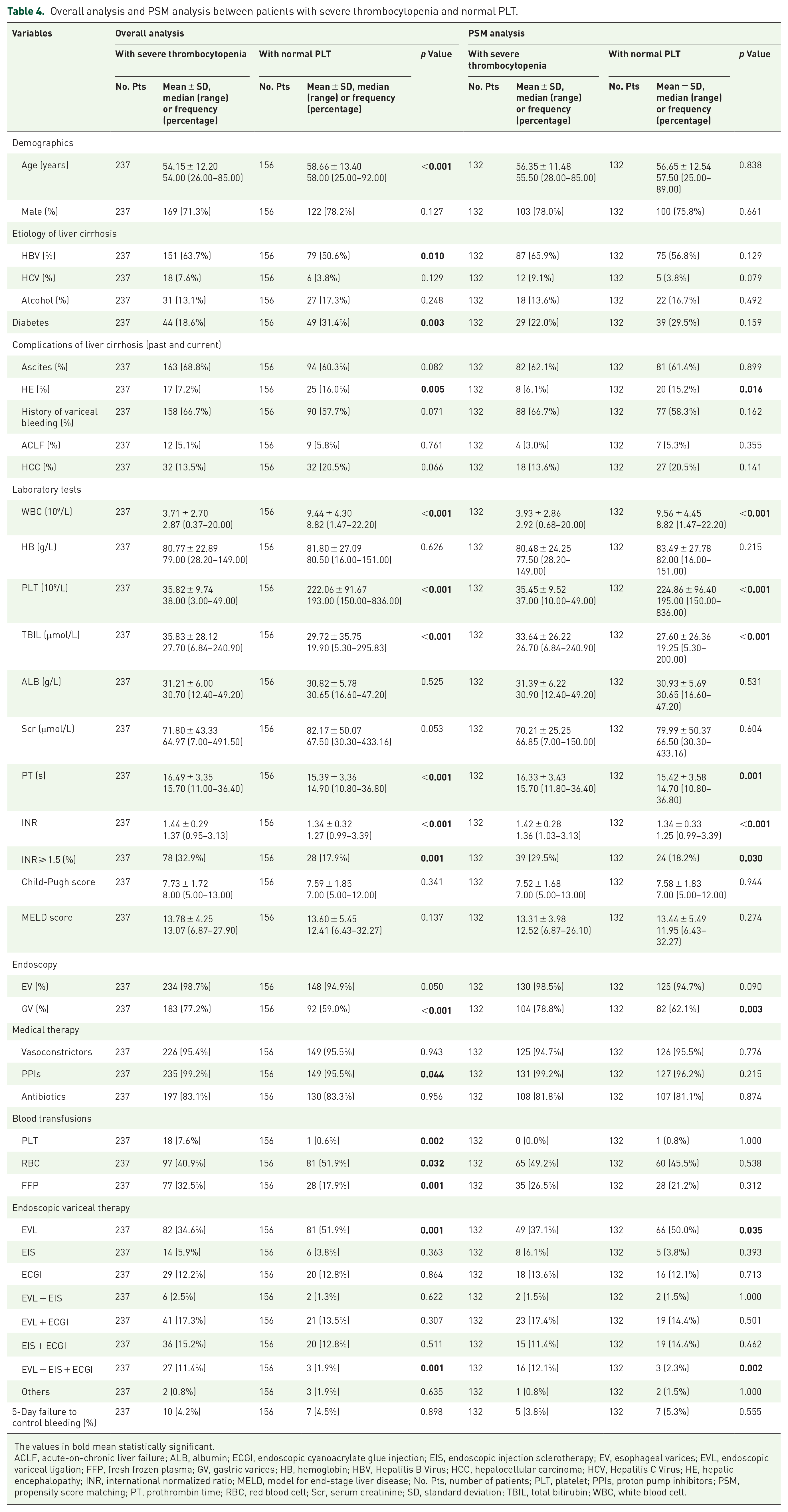
Severe thrombocytopenia versus normal PLT
In the overall analysis, patients with severe thrombocytopenia had significantly higher TBIL (35.83 μmol/L vs 29.72 μmol/L, p < 0.001), PT (16.49s vs 15.39s, p < 0.001), INR (1.44 vs 1.34, p < 0.001), and prevalence of GV (77.2% vs 59.0%, p < 0.001), but lower WBC (3.71 × 109/L vs 9.44 × 109/L, p < 0.001). However, the rate of 5-day failure to control bleeding was not significantly different between the two groups (4.2% vs 4.5%, p = 0.898; Table 4). Univariate logistic regression analysis showed that the presence of severe thrombocytopenia was not independently associated with the rate of 5-day failure to control bleeding (cOR = 0.938, 95% CI = 0.349–2.518, p = 0.898). Multivariate logistic regression analysis showed that the presence of severe thrombocytopenia was not independently associated with the rate of 5-day failure to control bleeding (aOR = 0.771, 95% CI = 0.256–2.315, p = 0.642).
Overall analysis and PSM analysis between patients with severe thrombocytopenia and normal PLT.
The values in bold mean statistically significant.
ACLF, acute-on-chronic liver failure; ALB, albumin; ECGI, endoscopic cyanoacrylate glue injection; EIS, endoscopic injection sclerotherapy; EV, esophageal varices; EVL, endoscopic variceal ligation; FFP, fresh frozen plasma; GV, gastric varices; HB, hemoglobin; HBV, Hepatitis B Virus; HCC, hepatocellular carcinoma; HCV, Hepatitis C Virus; HE, hepatic encephalopathy; INR, international normalized ratio; MELD, model for end-stage liver disease; No. Pts, number of patients; PLT, platelet; PPIs, proton pump inhibitors; PSM, propensity score matching; PT, prothrombin time; RBC, red blood cell; Scr, serum creatinine; SD, standard deviation; TBIL, total bilirubin; WBC, white blood cell.
In the PSM analysis, 132 patients were matched to each group. Patients with severe thrombocytopenia had significantly higher TBIL (33.64 μmol/L vs 27.60 μmol/L, p < 0.001), PT (16.33s vs 15.42s, p = 0.001), INR (1.42 vs 1.34, p < 0.001), and prevalence of GV (78.8% vs 62.1%, p = 0.003), but lower WBC (3.93 × 109/L vs 9.56 × 109/L, p < 0.001) than those with normal PLT. However, the rate of 5-day failure to control bleeding was not significantly different between the two groups (3.8% vs 5.3%, p = 0.555; Table 4).
Discussion
Hepatic venous pressure gradient (HVPG) >20 mmHg is the most widely recognized predictor of 5-day failure after EVT. 7 However, the applicability of HVPG measurement in patients with AVB is limited, because it is invasive and only available in specialized centers.17,18 By comparison, low PLT serves as a convenient noninvasive predictor for the presence of large gastroesophageal varices,19 –21 which are a consequence of high portal pressure and more prone to cause variceal rupture. 22 Our previous study found that PLT was significantly lower in cirrhotic patients with AVB than those without, indicating a close association of PLT with portal hypertension-related bleeding in cirrhosis. 23 Recent studies have further investigated the association of PLT with the outcomes of cirrhotic patients after EVT.24 –26 Most of them focused on patients who underwent prophylactic EVT and found that the risk of bleeding after prophylactic EVT was not associated with PLT.24 –26 But there are very limited data on the association between thrombocytopenia and failure to control bleeding within 5 days after EVT. A previous Italian study by Amitrano et al. 11 prospectively evaluated the risk factors of 5-day failure in 185 cirrhotic patients with AVB after EVT, and showed that Child-Pugh class C, WBC count over 10 × 109/L, and portal vein thrombosis were independent predictors of the 5-day failure, but not PLT (89 × 109/L vs 105 × 109/L, p = 0.184). Besides, a Chinese nationwide study by Huang et al. 13 retrospectively included 1399 cirrhotic patients with AVB to explore the risk factors of rebleeding within 5 days after emergency endoscopy, and showed that PLT was not significantly associated with the risk of rebleeding within 5 days after EVT. Another study conducted by Chau et al. 12 in the United Kingdom prospectively included 20 cirrhotic patients with AVB to explore the predictors of rebleeding within 1–7 days after EVT and found that PLT was not significantly different between patients who developed early rebleeding and those who did not after therapeutic endoscopy (42 × 109/L vs 71 × 109/L, p = 0.60). Similarly, the main finding of our study was that thrombocytopenia may not be associated with failure to control bleeding within 5 days after EVT in cirrhotic patients with AVB. A major explanation for our finding should be that PLT function was often preserved in cirrhotic patients with thrombocytopenia, possibly due to elevated levels of von Willebrand factor.27 –29 Another potential explanation could be that multiple risk factors for 5-day failure to control bleeding after EVT, such as hepatic encephalopathy, more severe cirrhosis, and presence of hepatocellular carcinoma,30,31 were not significantly different between cirrhotic patients with and without thrombocytopenia in our patients. There is a seemingly counterintuitive phenomenon that the Child-Pugh score and MELD score were not significantly different between the patients with and without thrombocytopenia. Thus, thrombocytopenia may reflect an acute consumption of PLT in the setting of AGIB, but not sufficiently indicate the severity of liver cirrhosis.
As compared to previous studies, our study has several advantages in terms of study design. First, in our study, the data of cirrhotic patients with AGIB were prospectively and consecutively collected at 23 hospitals from 8 countries. Thus, such a large sample size in our study enhanced the credibility of our conclusions, and multiple sources of the included data allows for the generalizability of our conclusions. Second, the PSM analyses were performed to balance the severity of liver cirrhosis between the two groups. Notably, previous studies have demonstrated that the severity of liver cirrhosis evaluated by Child-Pugh class or MELD score was a strong predictor of 5-day failure in cirrhotic patients with AVB.7,31 Accordingly, our statistical results should be more reliable to reflect the impact of thrombocytopenia on the outcomes of cirrhotic patients with AVB. Third, we stratified the severity of thrombocytopenia and further explored the association between different grades of thrombocytopenia and the rate of failure to control bleeding within 5 days.
Our study also had several limitations. First, our study was retrospective with selection bias. Second, EVT was performed at different hospitals. The difference in the levels of endoscopists’ skills could potentially influence the patients’ outcomes. Third, the long-term outcomes of cirrhotic patients with AVB were not evaluated. Fourth, the data regarding liver stiffness value, HVPG, and portal vein thrombosis had not been collected in our multicenter study. Thus, their impact on the failure of treatment could not be further explored.
Conclusion
In conclusion, the short-term outcomes of cirrhotic patients with AVB after EVT might not be dependent upon the presence and grade of thrombocytopenia. Thus, it seems that the correction of thrombocytopenia by platelet infusion and use of thrombopoietin before EVT, an invasive procedure, is not warranted.
Footnotes
Appendix
Acknowledgements
We are indebted to the colleagues from 23 participating centers of the V-CAGIB study, who are not listed as the authors of this paper, for their great contributions to establish and verify this prospective international multicenter database, including Zhaohui Bai, Yuhang Yin, Wentao Xu, Sijia Zhang, Xiaotong Li, Guo Lin, Di Sun, Yao Xiao, Xu Gao, Shoujie Zhao, Zhenhua Liu, Qinghe Cheng, Yunxin Wang, Hao Jiang, Yan Feng, Yaning Zhang, Botao Ning, Na Sun, Jinling Dong, Wenming Wu, Jian Zhang, Emine Mutlu, Stephany Castillo-Castañeda, Giuseppe Butera, and Alberto Maringhini.
Author’s note
Number of patients enrolled from 23 participating centers for the present sub-study is listed as follows: (1) Bimin Li: The First Affiliated Hospital of Nanchang University, Nanchang, China (N = 212); (2) Lei Liu: Tangdu Hospital, The Fourth Military Medical University, Xi’an, China (N = 193); (3) Su Lin: The First Affiliated Hospital of Fujian Medical University, Fuzhou, China (N = 97); (4) Fernando Gomes Romeiro: Botucatu Medical School, São Paulo State University, Botucatu, Brazil (N = 82); (5) Xingshun Qi: General Hospital of Northern Theater Command, Shenyang, China (N = 82); (6) Mingyu Sun: Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, China (N = 70); (7) Fanpu Ji: The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China (N = 53); (8) Qiang Zhu: Shandong Provincial Hospital affiliated to Shandong First Medical University, Jinan, China (N = 51); (9) Yingli He: The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China (N = 43); (10) Dapeng Ma: The Sixth People’s Hospital of Dalian, Dalian, China (N = 40); (11) Shanshan Yuan: Xi’an Central Hospital, Xi’an, China (N = 40); (12) Xiaofeng Liu: The 960th Hospital of Chinese PLA, Jinan, Shandong, China (N = 29); (13) Cyriac Abby Philips: The Liver Institute, Center of Excellence in GI Sciences, Rajagiri Hospital, Kerala, India (N = 18); (14) Metin Basaranoglu: Bezmialem Vakif University, Istanbul, Turkey (N = 15); (15) Nahum Méndez-Sánchez: Medica Sur Clinic, National Autonomous University of Mexico, Mexico City, Mexico (N = 13); (16) Kanokwan Pinyopornpanish: Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand (N = 12); (17) Yiling Li: The First Affiliated Hospital of China Medical University, Shenyang, China (N = 11); (18) Yunhai Wu: The Sixth People’s Hospital of Shenyang, Shenyang, China (N = 6); (19) Ling Yang: Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China (N = 4); (20) Lichun Shao: Air Force Hospital of Northern Theater Command, Shenyang, China (N = 4); (21) Andrea Mancuso: Azienda di Rilievo Nazionale ad Alta Specializzazione Civico-Di Cristina-Benfratelli, Palermo, Italy (N = 3); (22) Yu Chen: Beijing You’an Hospital Affiliated to Capital Medical University, Beijing, China (N = 1); (23) Frank Tacke: Charité—Universitätsmedizin Berlin, Berlin, Germany (N = 0).