
Abstract
Background:
Microbiota restoration is highly effective to treat recurrent Clostridioides difficile infection (CDI) in observational studies (cure rates >90%) but efficacy in controlled clinical trials appears to be lower.
Objectives:
To perform an updated meta-analysis to assess the efficacy of microbiota restoration for recurrent CDI in open-label registered prospective clinical trials compared to randomized controlled trials (RCTs).
Design:
A systematic review and meta-analysis was conducted.
Data Sources and Methods:
A systematic search of various databases was performed up to July 2022 to identify studies of interest. Clinical trials of microbiota restoration for recurrent CDI with clinical resolution with one dose were included. We calculated weighted pooled rates (WPRs) with 95% confidence intervals (CIs).
Results:
In all, 19 clinical trials with 1176 recurrent CDI patients were included. Of the patients treated with microbiota restoration, 897 experienced a clinical cure with a single microbiota restoration therapy (WPR, 78%; 95% CI, 71–85%). There was significant heterogeneity among studies with an I2 of 88%. Analysis of trials with a control arm (non-microbiota restoration) revealed CDI resolution in 373 of 523 patients (WPR, 72%; 95% CI, 60–82%) with microbiota restoration. Among the nine open-label clinical trials, CDI resolution was seen in 524 of 653 patients after initial microbiota restoration (WPR, 84%; 95% CI, 74–92%). Comparison of resolution rates between RCTs and open-label trials revealed a lower cure rate in RCTs compared to open-label trials (WPR, 73 versus 84%, p < 0.0001).
Conclusions:
Microbiota restoration in a randomized controlled setting leads to lower resolution rates compared to open label and observational settings, likely due to stricter definitions and inclusion criteria. Resolution rates in open-label studies were similar to observational studies.
Keywords
Introduction
Clostridioides difficile infection (CDI) is the most common healthcare-associated infection in the United States with over 50% of patients developing recurrences after two or more episodes. Microbiota replacement therapy (MRT) is used to treat recurrent CDI by restoring a healthy gut microbiome. Guidelines from the Infectious Diseases Society of America and Society of Healthcare Epidemiology of America recommend MRT after appropriate antibiotic treatment after two or more CDI recurrences in patients who have failed appropriate antibiotic treatments. 1
The efficacy of MRT for recurrent CDI in observational studies is more than 85% but efficacy in controlled clinical trials appears to be lower. 2 Our 2017 meta-analysis showed an overall cure rate of 76% in clinical trial settings with efficacy being lower (67%) in trials with a comparator group compared to open-label trials. 3 Most trials included in that meta-analysis had different methodologies including recurrent CDI diagnostic and inclusion criteria, MRT preparations, and comparator group leading to a significant heterogeneity. These inconsistencies have resulted in limiting the generalizability of these results and pose a caution in positioning MRT as a therapy for CDI.
Since the earlier systematic review and meta-analysis, more evidence from trials regarding use of MRT has emerged. These have included phase III trials of fecal microbiota transplantation (FMT) and standardized live biotherapeutics for recurrent CDI. We performed an updated meta-analysis with the latest evidence to reassess the efficacy of microbiota restoration in clinical trials.
Methods
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines to conduct this meta-analysis. 4
Selection criteria and data search
A systematic search of electronic databases including Ovid MEDLINE In-Process & Other Non-Indexed Citations, Ovid MEDLINE, Ovid Embase, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, Web of Science, and Scopus, along with abstracts and press releases from major gastroenterology and infectious diseases conferences, was performed up to July 2022. The search strategy was designed and conducted independently by Mayo Clinic library staff and two study investigators (S.K. and R.T.). A controlled vocabulary supplemented with keywords was used to search for studies that used FMT for CDI. Main keywords used in the search were the following: Clostridium difficile, C diff, C difficile, Clostridium difficile infection, CDI, Clostridium difficile–associated diarrhea or CDAD, AND faecal or faeces or fecal or feces or stool or microbiota, with infusion or transplant or transfer or instill or reconstitute or donor or bacteriotherapy. The search was limited to English-language publications.
Studies considered in this meta-analysis were prospective clinical trials that included a study population of patients with recurrent CDI who were treated with microbiota restoration via any delivery modality.
Data abstraction
Two investigators independently abstracted data to a predetermined collection form (S.K. and R.T.). Data collected for each study included study setting and design, year of publication, number of patients, patient characteristics, indication for FMT, FMT route, type of donor used for FMT, duration of follow-up, and outcomes. Discrepancies in data collection were resolved by consensus, referring to the original article.
Outcomes assessed
In our primary analysis, we calculated the clinical resolution rate with single microbiota restoration treatment with stool transplant or a live biotherapy in a controlled setting. We did not include patients treated with multiple MRTs after clinical failure with initial MRT in our primary analysis.
Statistical analysis
Our primary outcome of the pooled analysis was clinical cure rates. The random-effects model described by DerSimonian and Laird was used to calculate the weighted pooled rate (WPR). 5 We calculated WPRs with corresponding 95% confidence interval (CI) for the overall analysis as well as subgroup analyses. Data were weighted on sample size in each trial to calculate WPR. We assessed heterogeneity within groups with the I2 statistic, which estimates the proportion of total variation across studies that is due to heterogeneity in study patients, design, or interventions rather than chance; I2 values > 50% suggest substantial heterogeneity. All p values reported are two-tailed. For all tests (except for heterogeneity), a p value of <0.05 was considered statistically significant. Calculations were performed and graphs constructed with MetaXL meta-analysis software (version 5.3; EpiGear International Pty Ltd, Sunrise Beach, Queensland, Australia).
Risk of bias assessment
We use the Cochrane collaboration risk of bias tool to assess the methodologic quality of the included trials. 6 The Cochrane risk of bias tool consists of fixed domains of bias that focus on aspects of trial design, reporting, and conduct. The items assessed using this tool included methods used to generate the randomization schedule and conceal allocation, blinding, completeness of outcome data, and evidence of selective outcome reporting.
Results
Search results
We found a total of 1677 unique studies using the described search strategies. The titles and abstracts were screened for all the studies and a total of 44 relevant articles were selected. Of the 44 relevant articles, we excluded 26 for various reasons and included a total of 18 studies in the final meta-analysis (Figure 1).

Detailed search strategy for inclusion of studies.
Characteristics of the included studies
In all, 19 clinical trials reported in 18 studies with 1176 recurrent CDI patients were included.2,7–23 Of the included trials, 10 had a control arm and for the remaining 9, all patients received a microbiota restoration therapy as open label. For trials with a control arm, six trials used antibiotics followed by placebo and three used standard antibiotics (vancomycin or fidaxomicin) only. Data from two RBX2660 trials have been presented as a combined report and was included as a single study. Follow-up ranged from 8 to 24 weeks. The characteristics of the included studies are described in Table 1.
Characteristics of the included studies.

CDI, Clostridioides difficile infection; NA, not applicable.
Risk of bias
The risk of bias assessment for all included studies is described in Table 2. All trials had appropriate reporting and incomplete outcome data assessment. All randomized controlled trials (RCTs) used appropriate methods for random sequence generation. All open-label trials were considered as moderate bias due to lack of blinding and random sequence generation (Table 2).
Risk of bias assessment in the included studies.
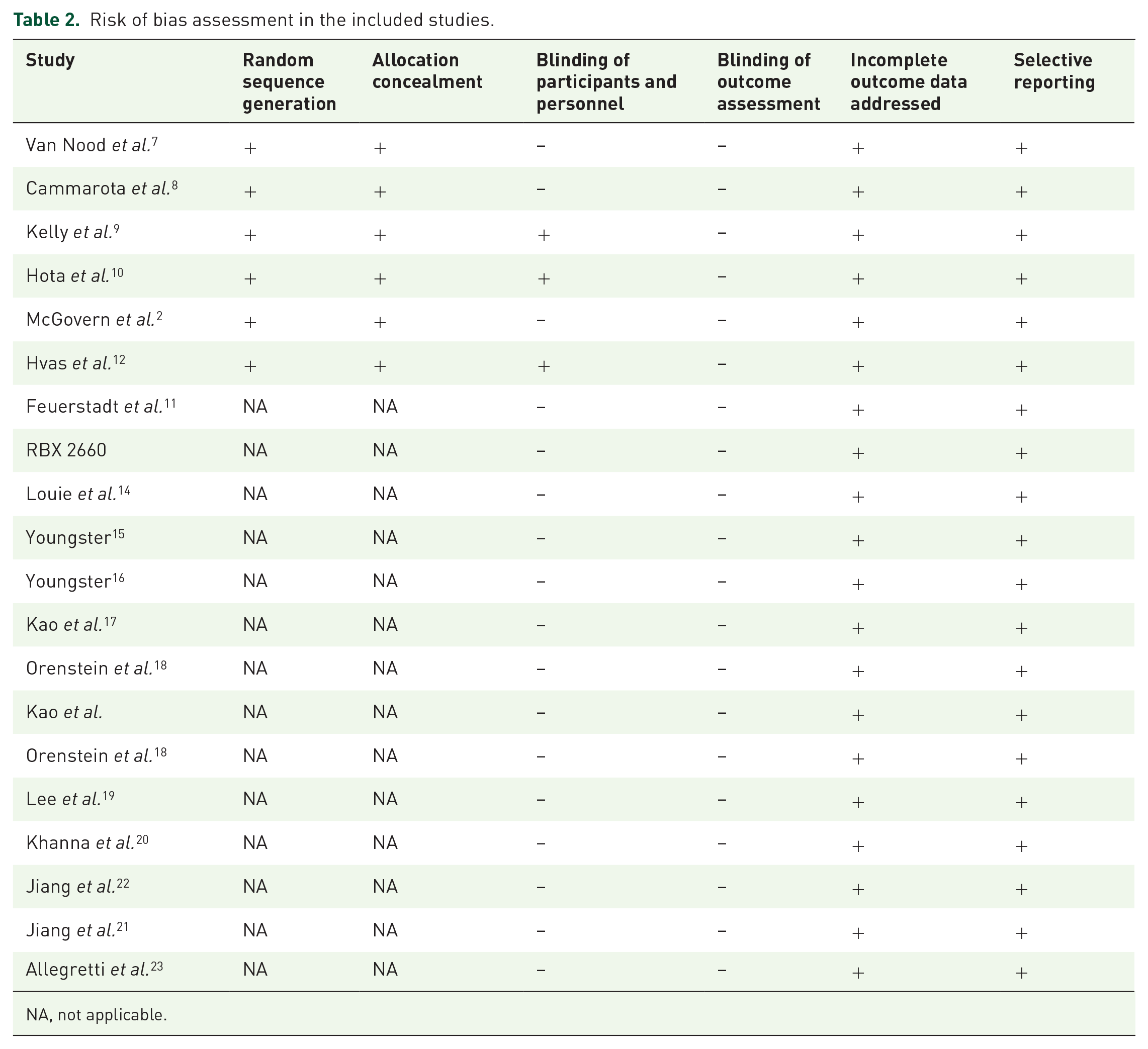
NA, not applicable.
Clinical cure with single MRT
In the 19 trials reporting on 1176 patients treated with a single microbiota restoration therapy, 897 experienced a clinical cure overall (WPR, 78%; 95% CI, 71–85%). There was significant heterogeneity among studies with an I2 of 88% (Figure 2).
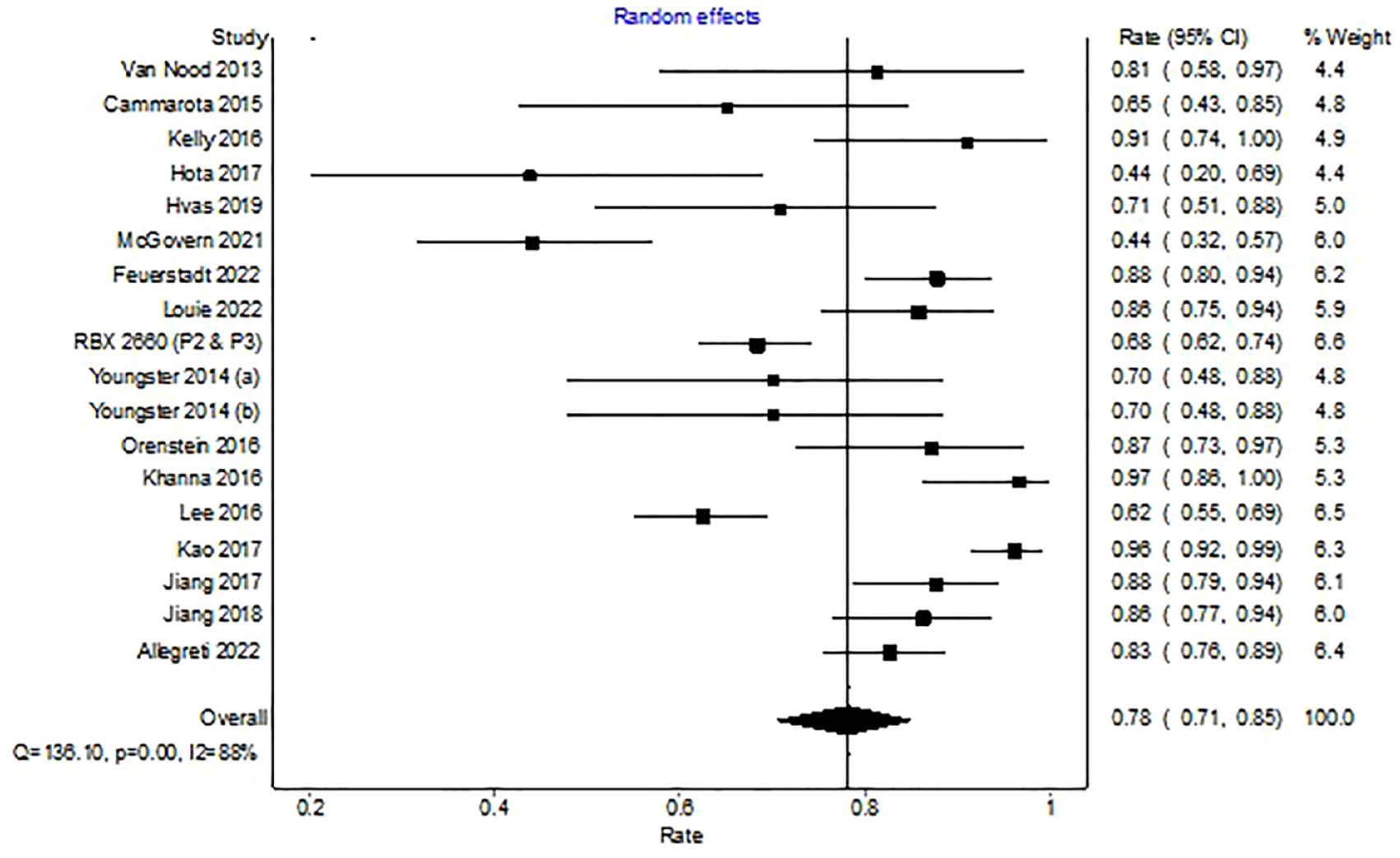
Forest plot depicting clinical resolution with microbiota replacement among clinical trials.
Clinical cure with MRT in trials with a control arm
Analysis of 10 trials with a control arm (non-microbiota restoration) revealed CDI resolution in 373 of 523 patients (WPR, 72%; 95% CI, 60–82%) with microbiota restoration. There was significant heterogeneity among the included studies with an I2 of 84% (Figure 3).
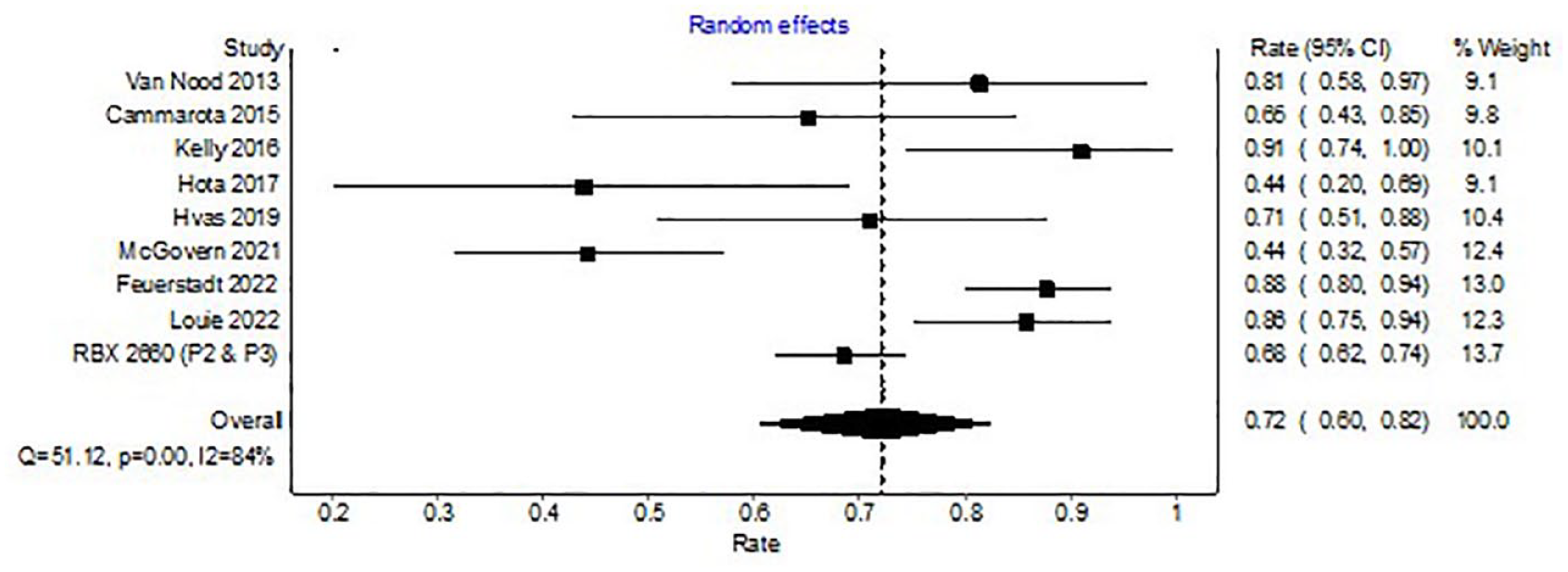
Forest plot depicting clinical resolution with microbiota replacement among clinical trials with control arm.
Clinical cure in control arm
Analysis of the 10 trials with non-microbiota restoration revealed CDI resolution in 201 of 397 patients with antibiotics (WPR, 52%, 95% CI, 43–60%). There was significant heterogeneity among the included studies with an I2 of 61%.
Comparison of cure rates with microbiota restoration versus antibiotics showed higher cure rate with microbiota restoration [WPR 72%, (95% CI, 60–82%) versus 52% (95% CI, 43–60%); p < 0.0001].
Clinical cure with MRT in open-label trials
Among the nine open-label clinical trials, CDI resolution was seen in 524 of 653 patients after initial microbiota restoration (WPR, 84%, 95% CI, 74–92%). There was significant heterogeneity among the included studies with an I2 of 89% (Figure 4).

Forest plot depicting clinical resolution with microbiota replacement among open-label trials.
Comparison of cure rates between clinical trials with a control arm and those without revealed a lower cure rate in trials with a control group [WPR; 72% (95% CI, 60–82%) versus 84% (95% CI, 74–92%); p < 0.0001].
Discussion
In this study, we demonstrate that the efficacy of microbiota restoration for recurrent CDI was lower in trials with a comparator group compared to open-label trials of MRT. Among the included trials, there was a noteworthy variation in methodology, control group, route of administration, and type of microbiota restoration therapy used. The cure rate in the control group receiving antibiotics only was significantly lower compared to microbiota restoration.
The low-efficacy rate noted in clinical trials with a comparator group likely stems from strict inclusion and exclusion criteria and strict definition of cure in controlled trials. A recent meta-analysis, including both observational studies and clinical trials (n = 45), found the efficacy of MRT to be 84% following a single dose and reported high-cure rates both in observational and controlled settings. However, it may be noted that the efficacy in subgroup analysis of clinical trials (open label and RCT) was noted to be 72% likely from lower cure rates in RCT. 24 Our pooled analysis with updated literature shows similar results.
We also found significant heterogeneity among the included trials. One study evaluated the heterogeneity among randomized clinical trials for MRT and found significant differences in study methodology, control groups, prior antibiotic treatment, number of FMT administrations, and time to clinical outcomes assessed. 25 All these heterogeneous aspects lead to differences in estimated efficacy rates as well as limiting the generalizability of the results.
Trials included in our study are foundational studies to access the efficacy of MRT in recurrent CDI. Future studies may consider accessing the use of MRT for severe and fulminant CDI. There have been studies regarding the use of FMT in severe and fulminant disease and a recent meta-analysis including 10 studies (8 case series, 1 case–control, and 1 randomized study) suggested that FMT was safe and effective for severe fulminant CDI. 26 In addition, there have been prior studies looking at the predictors of FMT failure from real-world data and found several predictors including old age, poor quality of bowel preparation, concurrent inflammatory bowel disease (IBD), and peri FMT use of non-CDI antibiotics. Given that most of the trials have excluded patients with concurrent IBD and patients taking antibiotics, it would be interesting to access the efficacy of MRT among these high-risk patients. 27
The strength of our study includes comprehensive literature review with large population from clinical trials. Our study has several limitations. There was lack of microbiome data in most of the trials; hence, we were not able to explore the effect of donor and recipient microbiome. Other factors that may have affected FMT include antibiotic exposure and prior hospitalizations. Those were not reported uniformly and calls for more uniform reporting of FMT trials.
Conclusion
In conclusion, data from open-label trials and observational studies suggest that while MRT is an effective option for recurrent CDI, results vary based on the study design. Newer data from clinical trials are extremely promising for the use of MRT for recurrent CDI. There are still opportunities for optimization of future trials which include boarder patient population, more consistent approach for the inclusion of patients with standardization of products, and universal follow-up durations.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231174293 – Supplemental material for Resolution rates in clinical trials for microbiota restoration for recurrent Clostridioides difficile infection: an updated systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848231174293 for Resolution rates in clinical trials for microbiota restoration for recurrent Clostridioides difficile infection: an updated systematic review and meta-analysis by Raseen Tariq, Darrell S. Pardi and Sahil Khanna in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.