
Abstract
Background:
We previously reported that antofloxacin-based bismuth quadruple therapy was safe and effective for Helicobacter pylori (H. pylori) eradication. It is not clear whether the addition of Saccharomyces boulardii (S. boulardii) to antofloxacin-based quadruple therapy can improve the eradication rate of H. pylori and reduce adverse events.
Objective:
To investigate the effect of adding S. boulardii to antofloxacin-based quadruple therapy on the eradication rate of H. pylori and the adverse events.
Design:
Single-center, prospective randomized controlled study.
Methods:
A total of 172 patients with H. pylori infection were randomly assigned to the test and control groups. Patients in the control group (n = 86) received antofloxacin-based bismuth quadruple therapy for 14 days. On this basis, cases in the test group (n = 86) received S. boulardii 500 mg b.i.d. The eradication rate of H. pylori and adverse events were observed 4 weeks after the treatment.
Results:
There were no statistically significant differences in the eradication rates of H. pylori and frequency of diarrhea between the test group and control group (p > 0.05). The duration of diarrhea in the test group was significantly shorter than in the control group (p < 0.001). In addition, the two groups exhibited similar adverse event rates for epigastric pain, abdominal distention, dizzy, vomiting, and rash (p > 0.05). The severity of adverse reactions was similar between the two groups (p > 0.05), and most of them had mild adverse events.
Conclusion:
Although the addition of S. boulardii to antofloxacin-based quadruple therapy could not improve the eradication rate of H. pylori, it could shorten the time of antibiotic-associated diarrhea and reduce the incidence of diarrhea.
Trial registration number:
ChiCTR2200056931.
Keywords
Introduction
Helicobacter pylori is a gram-negative bacterium that colonizes the gastric mucosa. Currently, the infection rate of H. pylori in China is about 50%. 1 H. pylori infection is a chronic, persistent infection that is not only closely related to a variety of digestive system diseases, but also induces a series of immune responses in other systems and may lead to extragastrointestinal diseases such as vitamin B12 deficiency, Alzheimer’s disease, iron deficiency anemia of unknown cause, atherosclerosis, and idiopathic thrombocytopenic purpura. Eradication of H. pylori at an early stage can significantly reduce the risk of gastric cancer.2,3 However, the eradication rate of H. pylori has been declining due to the increasing resistance of H. pylori and the influence of the host CYP2C19 gene polymorphism.4,5
To improve the eradication rate of H. pylori infection, many scholars have done a lot of research in recent years. Antofloxacin is the fourth generation of fluoroquinolones, independently developed in China. In June 2009, the China Food and Drug Administration approved antofloxacin for the market, which has become one of the drugs of choice for clinical anti-infection treatment. 6 In 2019, we first analyzed the safety and efficacy of antofloxacin-based therapy for H. pylori eradication. 7 Our findings suggested that eradication rates of H. pylori in the antofloxacin-based bismuth quadruple therapy were significantly higher than those in the levofloxacin-based bismuth quadruple therapy. According to the proposed report card grading scheme proposed by Graham, the intention-to-treat (ITT) eradication rate in our clinical trials was grade B, which could probably be further improved by changes in dose, duration, or drugs. 8 Besides, the adverse reactions, including diarrhea, nausea, abdominal pain, headache, and abdominal distension during the course of the medication, should not be ignored. 7
The Italian guidelines and the Maastricht VI/Florence consensus report in the management of H. pylori infection both recommended that certain probiotics, including S. boulardii, Lactobacillus, Bifidobacterium spp, etc., may have a beneficial effect on H. pylori eradication therapy through reduction of antibiotic-related side effects,9,10 which have been suggested as an adjuvant treatment for H. pylori eradication.11–13 Current studies indicated that S. boulardii was genetically similar to the model yeast Saccharomyces cerevisiae and had unique physiological properties, such as optimal growth temperature (37°C), being naturally resistant to antibiotics, gastric acidity, and proteolysis. 14 Some meta-analysis showed that the addition of S. boulardii to H. pylori eradication could improve the eradication rate of H. pylori and reduce adverse reactions.15–17 The guidelines have mentioned that the effect of probiotics on the eradication rate still remains controversial due to inconsistent data (such as probiotic species or strains, length of therapy, dosages, risk, etc.).9,10,18 In addition, we also found that previous clinical trials mainly discussed the efficacy of triple therapy in combination with S. boulardii, and few studies focused on S. boulardii combined with quadruple therapy. Recently, Yu et al. proposed adding S. boulardii to quadruple therapy, which relieved H. pylori eradication-induced antibiotic-associated side effects but did not improve the eradication rate of H. pylori. 19 Based on the outcomes of current studies, S. boulardii did reduce treatment-associated side effects for H. pylori eradication, especially gastrointestinal symptoms, but whether S. boulardii could improve the eradication rate of 14-day quadruple therapy for H. pylori was still lack of adequate evidence and has to be discussed further, just as what the guidelines have mentioned. In this study, we aimed to demonstrate the efficacy and safety of S. boulardii supplementation on antofloxacin-based bismuth quadruple therapy for H. pylori eradication.
Materials and methods
Subjects
In all, 172 patients aged 18–70 years who were diagnosed with H. pylori infection through 13/14C-urea breath test (13/14C-UBT) or histological evaluation at 900TH Hospital of Joint Logistics Support Force between January 2020 and December 2020 were enrolled. Patients with severe liver, renal, or heart dysfunction; malignant tumors; a history of gastrectomy; pregnancy or lactation; allergies to quinolone and penicillin drugs; or those who had previously received H. pylori eradication therapy were excluded. All patients agreed to take part in the study and signed informed consent. The reporting of this study conformed to the Consolidated Standards of Reporting Trials (CONSORT) statement.
Research methods
The subjects were assigned randomly to two groups in 1:1 ratio using a computer-generated random number, which was stored in opaque and sequentially numbered envelopes. The eligible patients were blinded to their own group assignment and the conditions of other participants. Patients in control group received antofloxacin-based bismuth quadruple therapy consisting of colloidal bismuth pectin (North China Pharmaceutical Co. Ltd., 50 mg/capsule) 200 mg t.i.d., antofloxacin (Anhui Global Pharmaceutical Co., Ltd., 100 mg/tablet) 200 mg, q.i.d., esomeprazole (AstraZeneca Pharmaceutical Co., Ltd., 20 mg/tablet) 20 mg, b.i.d., amoxicillin (Harbin Pharmaceutical Co., Ltd., 250 mg/capsule) 1000 mg, b.i.d. for 14 days, while patients in test group received the same antofloxacin-based bismuth quadruple therapy combined with S. boulardii (Biocodex, 250 mg S. boulardii/sachet) 500 mg b.i.d. for 14 days. The number of the viable yeast probiotic S. boulardii CNCM I-745 in 1 sachet of powder was not less than 5 billion colony forming unit, which has been confirmed in the manufacturer’s report. The S. boulardii was isolated from litchis and mangosteen, and was prepared, packaged, and controlled as lyophilized form, which ensured the adequate activity and stability of the strain. 20
Outcomes and post-therapy follow-up
The primary outcome was the eradication rates of H. pylori after 14-day quadruple therapy for H. pylori. The secondary outcomes were the rates of adverse events and the severity of adverse drug reactions. The details of outcomes and post-therapy follow-up were described below.
Patients were advised to take esomeprazole, colloidal bismuth pectin, and S. boulardii 30 min before meals, while the amoxicillin and antofloxacin were taken 1.5–2 h after meals. S. boulardii should not be taken with food or drinks which temperature were higher than 50°C. Patients were informed of possible side effects during the medication, such as nausea, vomiting, stomach pain, diarrhea, loss of appetite, headache, dizziness, rashes, bitter mouth, black stools, and so on. We provided questionnaires to patients to record drug compliance and adverse reactions. Adverse drug reactions were classified into three categories: mild (patient has mild symptoms that do not affect daily activities), moderate (patient’s symptoms affect some daily activities, but are tolerable), and severe (patient’s symptoms are unbearable and affect normal life; patient needs symptomatic treatment and withdrawal of medication).13C-UBT or 14C-UBT was performed at least 4 weeks after the withdrawal of all drugs. Negative results were considered successful eradication of H. pylori.
Sample size estimation
The eradication rate of antofloxacin-based bismuth quadruple therapy was 93.8% based on our previous study. 7 Calculations assumed the eradication rates of the control and test groups of 93%, a bilateral significance level of 0.05, a power of 0.90, and a presumed withdrawal rate of 10%, at least 61 patients were needed for each group.
Statistical analysis
The analysis was conducted using SPSS 26.0 statistical software. Eradication rates were evaluated by ITT and per-protocol (PP) analyses. The ITT analysis requires all the assigned participants to be included; the PP analysis excluded patients who have not dropped out for any reason and who received less than 90% of the therapeutic dose. Categorical variables were expressed as numbers and percentages, while continuous variables were expressed as mean ± standard deviation. Student’s t test, chi-square test, Fisher exact tests, and Mann–Whitney U test were applied wherever appropriate. For all statistical analyses, a p value < 0.05 (two-tailed) was considered a significant difference.
Results
Characteristics of the study groups
After excluding the 47 patients, a total of 172 patients with H. pylori infection were enrolled in our study. There were no significant differences in gender, age, smoking, alcohol consumption, or H. pylori infection diagnostic methods between the two groups (Table 1).
Demographic clinical characteristics of patients assigned to two regimens.

Data are represented as the mean ± SD or number of the patients (%) using the student’s t test and c2 test, respectively.
SD, standard deviation; 13/14C-UBT, 13/14C-urea breath test.
Eradication rates
One patient in the control group and one patient in the test group were lost in follow-up; treatment was discontinued due to diarrhea in two patients, vomiting in one patient in the control group, and abdominal distension in two patients in the test group. Ultimately, 82 and 83 patients were included in the PP analysis in the control and test groups, respectively (Figure 1).

Consolidated Standards of Reporting Trials flowchart of patients throughout the study.
In the ITT analyses, H. pylori was eradicated in 78/86 cases (eradication rate: 90.7%) in the control group and 80/86 cases (eradication rate: 93.0%) in the test group, the eradication rates were no statistical differences between the two groups (p = 0.781). In the PP analyses, the control group had similar eradication rates compared with the test group (95.1% versus 96.4%), and the eradication rates were no statistical differences between the two groups (p = 0.720) (Table 2).
Comparison of the H. pylori eradication rates in two groups.

Adverse events
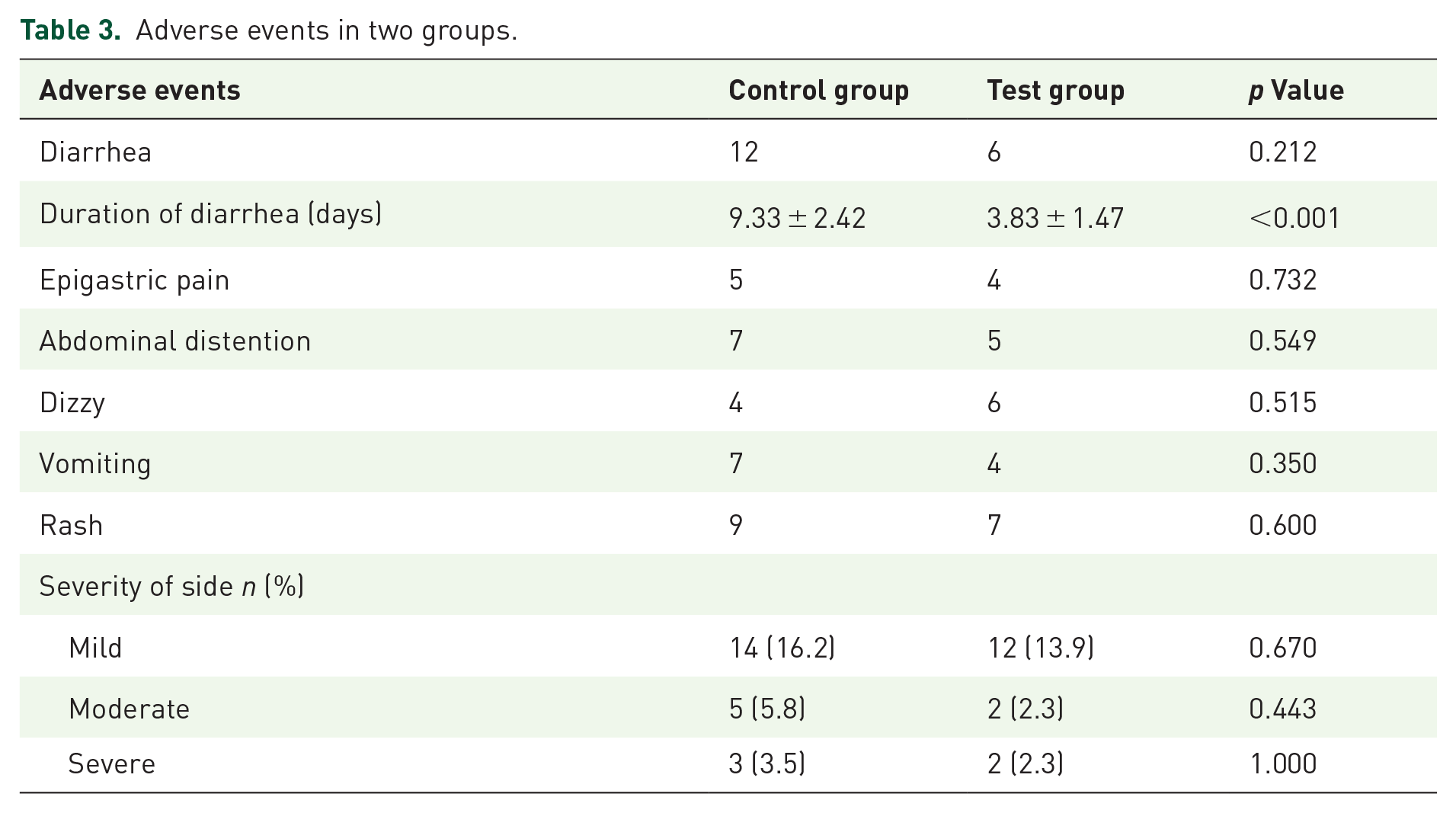
The major adverse reactions in both groups included diarrhea, epigastric pain, abdominal distention, dizzy, vomiting, and rash. The frequencies of diarrhea were lower in the test group (6/86, 7.0%) compared with the control group (12/86, 14.0%), but we found no significant difference between the two groups (p = 0.212). The duration of diarrhea in the test group was significantly shorter than in the control group (3.83 ± 1.47 versus 9.33 ± 2.42 days; p < 0.001). In addition, two groups exhibited similar adverse event rates for epigastric pain, abdominal distention, dizzy, vomiting, and rash (p > 0.05). The severity of adverse reactions was similar between the two groups (p > 0.05), and most of them had mild adverse events (Table 3).
Adverse events in two groups.
Discussion
At present, the eradication rate of H. pylori is mainly related to the increase in antibiotic resistance rate (20–50% for clarithromycin, 40–70% for metronidazole, and 20–50% for levofloxacin in China).21,22 Standard triple therapy for eradicating H. pylori does not meet clinical needs, and guidelines recommend bismuth quadruple therapy as the initial treatment.10,23 In recent years, we have found that the use of antofloxacin-based bismuth quadruple therapy can effectively eradicate H. pylori, 7 but the eradication rates of therapy have not achieved grade A eradication rate (eradication rate > 95%). 8 However, some adverse reactions are inevitable in the course of treatment, such as diarrhea, epigastric pain, abdominal distention, dizzy, vomiting, and rash, which can reduce patient compliance to a certain extent.
Our study found that the addition of S. boulardii could significantly shorten the time of antibiotic-associated diarrhea. Moreover, the incidence of diarrhea was reduced by 7% with S. boulardii plus antofloxacin-based bismuth quadruple therapy compared with antofloxacin-based bismuth quadruple therapy alone, although this reduction was not significant. The possible mechanisms of S. boulardii alleviating diarrhea are as follows: S. boulardii can be combined with the digestive tract mucosa epithelial cells to promote the reconstruction of the damaged epithelial cells and maintain the integrity of the gastrointestinal epithelial mucus layer. 24 S. boulardii cell walls contain a glucan that stimulates the secretion of immunoglobulin IgA in the digestive mucosa, enhancing the mucosal barrier. 25 S. boulardii can block or inhibit the nuclear transport of mitogen-activated protein kinase, Smad7, nuclear factor, and other signaling pathways, which reduce the synthesis of pro-inflammatory factors such as interleukin (IL)-6, IL-8, tumor necrosis factor alpha, and inhibit the local mucosal inflammation caused by neutrophil chemotaxis and degranulation. 26 Furthermore, S. boulardii can help to restore the normal microbiome in patients with antibiotic-associated diarrhea as modulators of the normal microbiome through colonization during the susceptibility period.14,27,28
Several meta-analyses have shown that S. boulardii combined with triple or quadruple therapy can increase the eradication rate of H. pylori and reduce the incidence of adverse reactions.15,29,30 In addition, compliance may improve by lowering the frequency of side effects, which may potentially improve H. pylori eradication rates. In vitro experiments showed that the structure of H. pylori was greatly changed after the S. boulardii and H. pylori were cultured together, and the part of H. pylori close to the S. boulardii was vacuolated and gradually shriveled, suggesting that the S. boulardii could inhibit the growth of H. pylori. 31 S. boulardii can directly inhibit H. pylori by producing lactic acid, short-chain fatty acids, neuraminidase, bacteritin, hydrogen peroxide, and other substances. Lactic acid can reduce the pH value in the stomach and enhance the antibacterial activity of short-chain fatty acids. Both lactic acid and short-chain fatty acids can weaken urease activity and inhibit the colonization and growth of H. pylori in the stomach. 32 Neuraminidase eliminated surface α (2-3) sialic acid, a ligand binding to H. pylori adhesin, which, in turn, inhibited H. pylori adhesion to duodenal mucosal epithelial cells. Bacteriocin and hydrogen peroxide can directly inhibit H. pylori. 31 In addition, S. boulardii can tolerate gastric proteolytic enzyme, gastric acid, bile salt, and other local pressures, which is 10 times the volume of common bacteria probiotics (1 μm). The large surface area of bacteria can better adhere to pathogenic bacteria and inhibit the colonization of H. pylori in gastric mucosa. 32
However, some studies found that adding S. boulardii to triple or sequential therapy did not improve H. pylori eradication rates.33,34 The synergetic effect of S. boulardii on H. pylori eradication was still controversial, even for low-efficacy triple therapy.19,35 Due to the high antimicrobial resistance and decreasing efficacy of triple therapy, bismuth quadruple therapy, concomitant therapy, and hybrid sequential-concomitant therapy (all of a 14-day course) have been suggested as the most effective treatment regimens.16,36 A new study has demonstrated that adding S. boulardii to bismuth-quadruple therapy has no important effect on the eradication of H. pylori. 19 Our study also noticed that S. boulardii combined with antofloxacin-based quadruple therapy failed to improve the eradication rate of H. pylori. Hence, the supplementation of S. boulardii seemed to have little influence on the quadruple therapy for H. pylori eradication. The reason may be that the amoxicillin and antofloxacin in this study have low drug resistance rates in the local population, so the antofloxacin-based quadruple therapy for 14 days has a high eradication rate. Research on primary antibiotic resistance of H. pylori in Chinese patients has shown that the resistance rate of amoxicillin and levofloxacin was about 3.4%, and 19.2%, respectively. 37 And a previous study in our center has shown that the minimum inhibitory concentration (MIC) against all local isolates for levofloxacin was 16 times higher than that for antofloxacin (16.0 µg/ml versus 1.0 µg/ml), and levofloxacin-resistant strains were found in 46.1% of the patients when the MIC of levofloxacin for the strains was ⩾1 µg/ml. 38 We observed that the susceptibility testing of H. pylori as per the gastric biopsy specimen showed antofloxacin resistance of only 2.7% compared to levofoxacin resistance of 32.44%. 7 Besides, the duration of H. pylori therapy must be taken into account. In fact, 14 days of H. pylori eradication therapy has been identified as superior to 7 days or 10 days. Some studies observed that probiotics adding to quadruple therapy for 14 days did not reduce the rate of side effects, while triple therapy for 7 days significantly increased eradication rates and reduced the rate of adverse reactions.11,39 We supposed that S. boulardii supplementation for triple therapy of H. pylori eradication might have a positive effect on the selection of a short course.
There still has some limitations in our studies. First, we did not investigate whether S. boulardii mitigated the gastric microbiome disruption caused by H. pylori eradication. Second, in our previous study, 38 the resistance of antibiotics such as antofloxacin to H. pylori was tested, so the resistance of antibiotics related to antofloxacin-based quadruple therapy was not tested again in this study, which may affect the analysis of the H. pylori eradication rate. Third, considering that the effect of S. boulardii adding to treatment for H. pylori eradication is still unclear, further study on this question should be desired, such as the duration of H. pylori therapy, doses and duration of S. boulardii, etc. At last, the study included a small sample of patients in a single center, and there was a selection bias.
Conclusion
In summary, although the addition of S. boulardii to antofloxacin-based quadruple therapy could not improve the eradication rate of H. pylori, it could shorten the time of antibiotic-associated diarrhea and reduce incidence of diarrhea. Due to the small sample size of this study, its effectiveness and safety still need to be verified by further large-scale and high-quality randomized controlled trials in China.