
Abstract
Pregnant patients with short bowel syndrome (SBS) and chronic intestinal failure (CIF) can successfully reach to term their pregnancies while on parenteral nutrition (PN) but with high rates of complications. The combination of rehabilitation surgery, combined with the use of novel treatment with enterohormones, especially semisynthetic glucagon-like peptide 2 (sGLP-2), has increased the chances to achieve intestinal sufficiency. Here, we report the case of a 33-year-old female with SBS/CIF (anatomy type 2), weaned off PN using sGLP-2 for 3.7 years, discontinued when she became pregnant. She was able to carry the pregnancy to term without any additional PN support. Considering that, we queried if the endogenous GLP-2 (eGLP-2) levels in this SBS patient, during the pregnancy and breastfeeding period, could be like those presented in healthy pregnant women and in non-pregnant SBS patients. Also, we inquired if there was any passage or increase in the plasmatic eGLP-2 from the fetus to the mother. Thus, we determined eGLP-2 levels in paired neonatal (cord blood) and maternal plasma samples from the SBS pregnant patient (n = 1), healthy pregnant women (controls, n = 2), and non-pregnant SBS patients (n = 12). The results indicated that the SBS pregnant patient showed higher eGLP-2 levels than non-SBS pregnant patients and healthy pregnant women along all the period studied. Furthermore, we found that the maternal sample had higher eGLP-2 levels than the neonatal sample, suggesting that fetal contribution to maternal eGLP2 levels would be minor. In conclusion, this study not only reports for the first time a case of a patient with SBS that was able to achieve intestinal adaptation after combining the use of autologous reconstructive surgery and sGLP-2, but also enlightens the possibility of carrying out an uneventful pregnancy and lactation without any nutritional support and remaining independent of sGLP-2.
Introduction
Intestinal failure (IF) patients suffer a reduction of gut function below the minimum necessary for the absorption of macronutrients and/or water and electrolytes, requiring intravenous supplementation to maintain health and/or growth. 1 Recently, this definition has change to pediatric population in which ‘Pediatric intestinal failure’ is defined as the reduction of functional intestinal mass below that which can sustain life, resulting in dependence on supplemental parenteral support for a minimum of 60 days within a 74 consecutive day interval. 2 There are three types of IF, type III (III-IF) is the chronic form of this disease. 3 Reports from existing registries, individual centers, and our own experience state that 75–80% of III-IF cases are due to short bowel syndrome (SBS). Surgical complications, intestinal ischemia, inflammatory bowel disease, and complications of bariatric surgery are among the most frequent etiologies. The physiological signals that influence intestinal adaptation are the presence of bile salts, peptides and enterohormones such as PYY, glucagon-like peptide 1 and 2 (GLP-1, GLP-2), and the presence of nutrients in the intestinal lumen. Endogenous GLP-2 (eGLP-2) is secreted by L cells of the distal ileum and proximal colon; among its main functions are delaying gastric emptying and decreasing secretions, increasing intestinal blood flow, maintaining adequate tropism of the mucosa, and decreasing epithelial apoptosis and membrane permeability. 4 A semisynthetic GLP-2 (sGLP-2) analogue resistant to degradation by serum dipeptidyl peptidase IV (DPPIV) (Teduglutide®) showed effectiveness and safety to rehabilitate patients with III-IF secondary to SBS.5,6 In our experience and in the medical literature, pregnant patients with SBS and chronic intestinal failure (CIF) can successfully reach term pregnancies while on parenteral nutrition (PN), but with high rates of complications. 7 To the best of our knowledge, no report has described the course, outcome, and behavior of SBS patients that became pregnant during long-term sGLP-2 treatment; therefore, we aim to describe the experience obtained as result of a comprehensive and translational approach in this matter.
Case report
We report the case of a 33-year-old female, with SBS-CIF due to a surgical complication that took place in April 2012. In September 2013, the patient underwent autologous reconstructive surgery (AGIRS) converting from type 1 to type 2 anatomy (the remaining anatomy was 60 cm of jejunum anastomosed to the left colon). PN was discontinued in December 2014. Nine months after this surgery, sGLP-2 analogue (Teduglutide®) was initiated. This treatment was administered for 3.7 years and suspended when the patient became pregnant.
During the pregnancy, no complication was reported, and there was no indication to reinitiate PN support. At 23 weeks of gestation, magnesium levels were altered (1.7 mg/dL) and immediately corrected by oral magnesium citrate supplements. The fetal echography was done at 27 weeks of gestation showing the absence of abnormalities and adequate growth. Urinary tract infection by Citrobacter spp. was detected at 31 weeks of gestation and was resolved with Ciprofloxacin treatment, without complications. Maternal weight was closely monitored and reached 7.15 kg (weight 66.150 kg; body mass index: 23.16 kg/m2) at the end of the third trimester. Because a mature placental appearance (grade 2–3) on ultrasonography by 30 weeks of gestation was observed, a cesarean section was performed at 35 weeks with the presence of the surgical staff and researchers to take cord and maternal samples. A healthy female fetus was delivered with appropriate weight (2.45 kg). Surgery and postoperative course were uneventful, and the patient was discharged on postoperative day 4. Breast-feeding was successfully initiated up to 6 months.
Considering the successful outcome, we questioned whether the eGLP-2 levels in this SBS pregnant patient during the pregnancy and breastfeeding period could be like those presented by non-pregnant SBS patients and healthy pregnant women. Furthermore, we queried if there was any passage or increase in the plasmatic eGLP-2 from the fetus to the mother.
To evaluate these hypotheses, blood samples were collected in tubes containing ethylenediaminetetraacetic acid and a specific DPPIV inhibitor. Plasma was immediately separated and stored at −80°C until analyzed by GLP-2 ELISA Kit (Abcam, Cambridge, MA, USA). Non-pregnant SBS patients followed at the IF and rehabilitation unit were included in the study (Tables 1 and 2 describe patients’ characteristics). The protocol was approved by the institutional review board (‘Comité de bioética de la Fundación Favaloro’) (IRB# 1537–1820). The patient details had de-identified and the patients gave his written informed consent to participate of the study as well as to the publication of the case. The case report was written following the case report guidelines (CARE), found at the https://www.equator-network.org/domain.
The demographic and clinical characteristics of the pregnant women.

SD, standard deviation; BMI, Body Mass Index.
The demographic and clinical characteristics of IF/SBS patients.

POC, postoperative complication.
Non-pregnant SBS patients showed lower eGLP-2 levels than the SBS pregnant patient (Figure 1). Considering that gender and anatomy type may have a strong influence in the eGLP-2 levels, we stratified patients according to gender (female or male) and the anatomy type (2 or 3); nevertheless, not differences in eGLP-2 levels between females and males, or in type 2 versus 3 anatomy group were found (Figure 1).

eGLP-2 levels from SBS pregnant versus non-pregnant SBS patients.
To determine whether there could be a contribution the eGLP2 levels from the fetus to the mother, eGLP-2 levels paired with neonatal (cord blood) and maternal plasma samples from the SBS pregnant patient (n = 1) and from healthy pregnant women (control, n = 2) were measured at delivery, and at two points during the breastfeeding period (1 and 6 months postpartum). We found that the maternal sample had higher eGLP-2 levels than neonatal sample (Figure 2), suggesting that fetal contribution to maternal eGLP2 levels would be minor. Moreover, we detected that eGLP-2 levels in samples from cord blood (neonatal) from the SBS patient were significantly inferior to those obtained from healthy pregnant women at the delivery (Figure 2). Finally, we observed that eGLP2 levels increased along lactation showing differences among groups at the sixth month postpartum. Interestingly, the pregnant SBS patient showed higher eGLP-2 levels than controls along the whole lactation period (Figure 2).
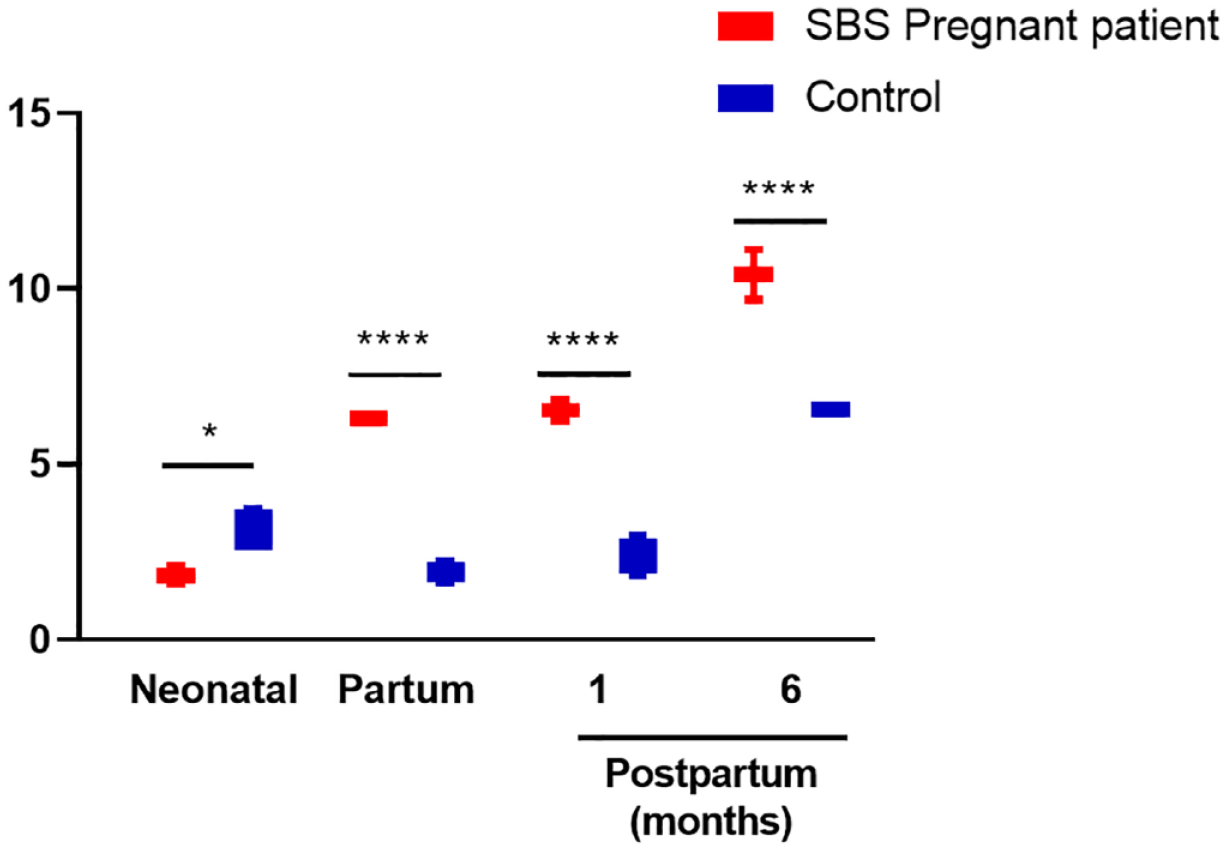
eGLP-2 levels paired with neonatal (cord blood) and maternal plasma samples from the SBS pregnant patient (n = 1) and from healthy pregnant women (without SBS, control, n = 2) at delivery (partum) and at two points during the breastfeeding period (1 and 6 months postpartum).
Discussion
To date, pregnancy can be carried out in patients on PN, but it can be associated with a high rate of complications related to the pregnancy itself (preeclampsia, postpartum hemorrhage, thrombosis), to the underlying disease, or to the PN support. 7 In this sense, the largest series of pregnancy in patients with IF estimates maternal complications in 67% of cases (mainly due to underlying disease or home PN complications).8,9 The present manuscript, not only reports a case of a patient with post-surgical SBS that was able to achieve intestinal adaptation with the combination of AGIRS and sGLP-2, 10 but also enlightens the possibility of carrying out an uneventful pregnancy and lactation without any nutritional support and remaining independent of sGLP-2.
In addition, this case shows for the first time, a higher eGLP2 plasma level at the time of delivery compared with non-pregnant SBS patients and with healthy pregnant women. This rise was independent of patients’ gender and anatomy type, suggesting that both variables did not influence the secretion of eGLP-2; therefore, a different source should be further studied.
Although much of the actual evidence was acquired from animal studies, it is known that pregnancy and lactation induce several changes in the intestine, including increase in bowel length, total absorptive mass due to increase in villous and crypt length, and optimization in several transporters and digestive functions.11,12 The molecular and hormonal basis of these changes is not completely established, but it is highly likely that eGLP-2 may participate in this path, which would be supported by the results showed in the present report.
The significant higher baseline eGLP-2 levels found in this pregnant SBS-patient, in comparison to the cohorts of healthy pregnant women and non-pregnant SBS-patients, together with the proportionally higher levels observed during breastfeeding, suggesting that long periods of sGLP-2 treatment could reach an effective intestinal rehabilitation sufficient not only to improve intestinal absorption, but also to probably increase the eGLP-2 production by neuro-entero-endocrine cells in others intestinal sites, or elsewhere. Further answers are required to better understand the source of eGLP-2 production in a patient like the one presented here, who lacks distal ileum and right colon. To our knowledge, there are no studies addressing the potential effects of sGLP-2 treatment on eGLP-2 levels once the treatment has concluded, the source of its production, or the potential hormonal effects caused by the breastfeeding as inductor of eGLP-2 production.
Notably, the strengths of this study involve the availability of matching pairs of maternal and neonatal plasma samples in the included study subjects. However, the low number of cases due to the infrequent events of pregnancy in IF patients represent a strong limitation. Thus, the results presented here should be reproduced in experimental models to be validated.
Footnotes
Acknowledgements
We thank Pablo and Osvaldo Stringa for their assistance with samples collection; we thank María de Luján Calcagno for her statistical assistance; and we would like to give a special thanks to Camilo Lis MD., former Takeda Southern Cone Medical Head, for helping to obtain funds for the reactive needed to measure eGLP-2.