
Abstract
Background:
Behçet’s disease (BD) is a relapsing systemic immune disorder, and intestinal BD is a significant cause of mortality in patients with BD. Conventional therapeutic strategies for intestinal BD showed unsatisfactory outcomes, especially in those patients with refractory subtypes. In recent years, biologic agents have exhibited promising results in this field. While the sample sizes of existing studies were limited, the results were heterogeneous.
Objectives:
This study aimed to observe the efficacy of different biologics in clinical symptomatic improvement and intestinal mucosal healing.
Design:
This is a study including the report of case series and meta-analysis.
Data sources and methods:
This meta-analysis was conducted following the PRISMA guidelines. Free-text words and subject terms, including ‘Behcet’s Syndrome’, ‘Biologics’, ‘Tumor Necrosis Factor Antagonist’, were used to systematically research the relevant studies in the electronic databases (PubMed, Web of Science, Embase, and Cochrane Library). All retrieved articles were from inception to July 2021, and the data from our institution were also included in this meta-analysis. A double arcsine transformation was performed to stabilize the variance of the original ratio. Heterogeneity was evaluated via Q-test and I2 statistics. Random-effects or fixed-effects model was used to calculate the pooled parameters, and the results were presented as forest plots with 95% confidence intervals.
Results:
Twelve studies were included, but only antitumor necrosis factor alpha (anti-TNF-α) agents were prescribed as biologicals for refractory intestinal BD. The symptom improvement rates at our institution ranged from 57.1 to 81.8%, and the mucosal healing rates were from 20 to 60% in different therapeutic periods. A total of 514 patients were enrolled in the meta-analysis, and the synthesized ratios showed that 59.8% (n = 377) and 73.7% (n = 317) of patients who received maintenance therapy with anti-TNF-α agents could achieve clinical symptomatic improvement during short-term (10–14 weeks) and long-term (48–54 weeks) periods, respectively. Furthermore, 77.8% (n = 229) of patients with intestinal BD maintained therapeutic efficacy for a longer time (100 weeks). In addition, 60.9% (n = 120) of the patients achieved sustained intestinal mucosal healing during a long-term follow-up (24–52 weeks).
Conclusion:
Anti-TNF-α treatment is effective in treating refractory intestinal BD but more studies are required to evaluate the effects of new biologics for intestinal BD in the near future.
Registration:
This study has been registered on PROSPERO, the ID is CRD42022329211.
Plain language summary
Behçet’s disease (BD) is a disease affecting several organs including the gastrointestinal tract. Nowadays, the efficacy of existing therapy strategies is still unsatisfactory and some patients are suffering from repeated attacks of the disease. We noticed that a new kind of medicine, called antitumor necrosis factor alpha (anti-TNF-α) agents, was applied to these patients recently. The therapeutic efficacy is not convincing enough to evaluate since the number of patients receiving this new medicine was small in every individual study. Regarding this, we conducted a research to learn about the efficacy of this medicine at our own institution. Besides, we composed the results of other studies in an appropriate way. Then, we drew a conclusion on the exact efficacy of anti-TNF-α agents after the data analysis. We unveiled that the anti-TNF-α agents appeared both effective and safe in the management of intestinal BD patients when the classical therapy failed. More than half of the patients could achieve discomfort remission when they got the therapy of the new medicine at our institution. We also found that intestinal ulcers in most patients improved after they received the treatment. All in all, it offered another foothold for getting relief in these patients who were caught in this mire.
Introduction
Behçet’s disease (BD) is a chronic relapsing inflammatory disease with a poorly understood etiology, and it is characterized by vasculitis with multisystem involvement including oral-genital-aphthous ulcers, ocular and neurological lesions.1–3 A diagnosis of intestinal BD is established when intestinal symptoms and typical gastrointestinal tract ulcers arise in the defined BD patients. 4 Besides, other typical oval-shaped large ulcers in the terminal ileum were contributory to the diagnosis after the exclusion of other diseases with similar manifestations. 5 Overall, intestinal BD accounts for only 5–10% of all BD patients. 6 The disease is prevalent in Asia and Mediterranean areas, but rare in western countries. 7 Inflammatory bowel disease is another relapsing autoimmune disease, and its pathogenesis and manifestations could mimic those of intestinal BD. Thus, therapeutic strategies for inflammatory bowel disease are generally prescribed for intestinal BD, including 5-aminosalicylic acids, steroids, and immunomodulators. 1 Nevertheless, not all patients obtain an alleviation from these conventional therapies, and some patients even deteriorate progressively or require surgery. It is reported that the cumulative 5- and 10-year surgery rates for intestinal BD have reached approximately 30 and 40%, respectively.8,9
In recent years, biologics have received attention for their high effectiveness in treating various inflammatory diseases.10–12 Multiple biologics have been applied as an alternative treatment for patients with BD, while the efficacy of biologics for intestinal BD is still indeterminate.13–15 Most of the published researches paid close attention to antitumor necrosis factor alpha (TNF-α) agents, but other biologics like interleukin-1 (IL-1) inhibitors, IL-6 inhibitors, or IL-17 inhibitors were rarely used. Although anti-TNF-α agents showed moderate effectiveness in intestinal BD, the relevant studies were single-arm retrospective observational studies with small sample sizes and the time periods of efficacy evaluation were highly heterogeneous. 7 As a result, variations among the recent evidence were remarkable and the exact efficacy of biologics for intestinal BD was inconsistent. 16
Currently, the therapeutic strategies for intestinal BD treatment have been just barely satisfactory and the evidence was mostly based on the findings of retrospective observational studies. To unveil the efficacy and safety of biologics for intestinal BD, we performed a retrospective study at our institution. Furthermore, a single-arm meta-analysis was performed and results from our institution were included. A better understanding of biologics in intestinal BD would be favorable to improve the therapeutic strategies and the prognosis, especially for those patients who failed to achieve alleviation in the conventional treatments.
Methods
Case series
Cases selection
A retrospective single-center case series was performed to indicate the efficacy of anti-TNF-α agents in intestinal BD at our institution. The information about patients with intestinal BD were screened from 1st January 2011 to 1st October 2021. Patients who received anti-TNF-α treatments were included and their electronic medical records were collected. These patients were mainly diagnosed according to the Japanese Behçet’s Disease Research Committee criteria and the discussions in multidisciplinary teams.
Data collection
We extracted data on the following clinical characteristics: sex, age, disease duration, clinical manifestations, biochemical and endoscopic examination findings, coinstantaneous medical treatments, and treatment history. The activity of BD was evaluated by Disease Activity Index for intestinal Behcet’s Disease (DAIBD), and this points-scoring system assesses general well-being, fever status, extraintestinal and intestinal manifestations. 17 Therapeutic efficacy was evaluated by the degree of improvement in clinical and endoscopic manifestations.
Meta-analysis
Search strategy
This meta-analysis was performed in accordance with the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ (PRISRM) guidelines. It has been registered on PROSPERO, the ID is CRD42022329211. We systematically searched published literatures in the PubMed (https://pubmed.ncbi.nlm.nih.gov), Web of Science (www.webofknowledge.com), Embase (https://www.embase.com), and Cochrane Library (http://www.cochranelibrary.com) databases. All databases were screened from inception to July 2021. The following free-text words and subject terms were included in our search strategies: ‘Behcet’s Syndrome’, ‘Biologics’, ‘Tumor Necrosis Factor Antagonist’, ‘Infliximab’, ‘Adalimumab’, ‘Etanercept’, ‘Tocilizumab’, ‘Golimumab’, ‘Canakinumab’, ‘Interleukin 1 Receptor Antagonist Protein’, and ‘Vedolizumab’. Furthermore, the reference lists of the selected articles were manually screened to avoid missing any qualified studies. (The search strategy for the PubMed database is provided in the Supplemental File 1.)
Study selection
After literature searching, we imported the bibliographies into EndNote X8 (Clarivate Analytics US LLC, Philadelphia, PA, USA) and removed duplicate records. The inclusion criteria were as follows: (a) patients were definitively diagnosed with intestinal BD; (b) they were treated with biologics; (c) effectiveness or safety assessment had been done with clearly reported results and estimating times. The following were excluded: (a) letters, editorials, expert opinions, reviews, or meeting abstracts; (b) articles written in a language other than English; (c) studies with duplicated patients and results; (d) studies with missing data. Two investigators (Zhan and Liu) independently screened the titles and abstracts of all retrieved information according to the inclusion and exclusion criteria. A flow diagram of the article selection process is presented in Figure 1.
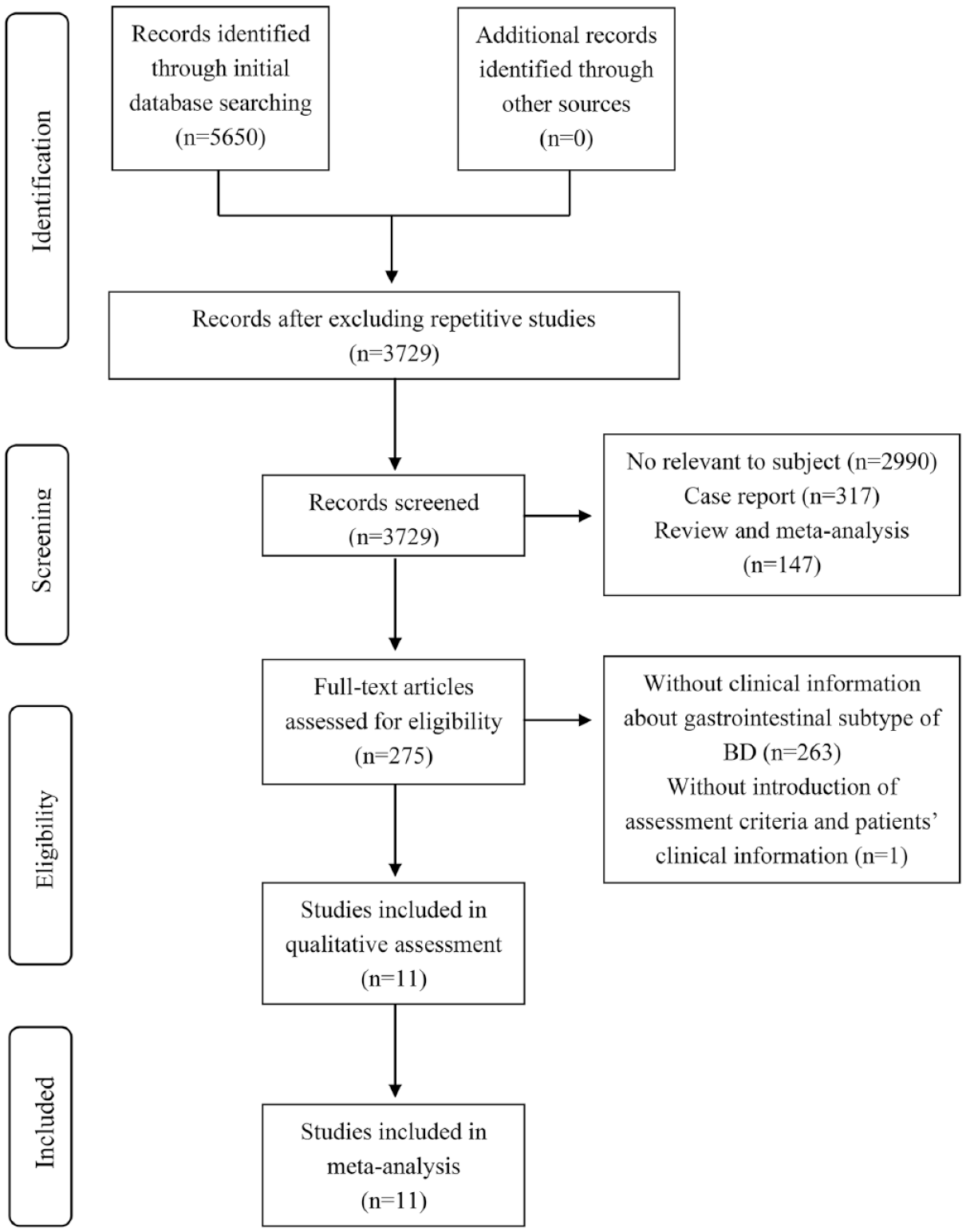
The flow diagram of this meta-analysis.
Data extraction
Two investigators (Zhan and Liu) independently extracted the data from the eligible articles, and disagreements were resolved through discussions with a third investigator (Zhuang). The following information was recorded from each study: first author, year of publication, types of biologics, age, clinical manifestations, criteria of disease evaluation, concurrent treatments, time of evaluation, total number of patients, and number of patients with intestinal symptoms/ulcers improved or disappeared after treatment. The diagnostic criteria across the included studies were similar. Almost all studies emphasized the existence of intestinal ulcers and other extraintestinal manifestations that allowed a BD diagnosis.5,18,19
In addition to DAIBD, the global gastrointestinal symptom score (GGISS) was also used to describe patients’ clinical conditions in the included studies.20,21 The GGISS is a ranking system that evaluates the influence of gastrointestinal symptoms on a patient’s daily life. This system includes the following items: ‘free of symptoms’, ‘did not affect daily life’, ‘slightly affected daily life’, ‘affected daily life’ and ‘critically affected daily life’, which are defined by patients themselves and score from 0 to 4 retrospectively. 22
Quality assessment
The quality assessment tool for case series studies developed by the Canadian Institute of Health Economics (IHE) was used to evaluate the research quality. 23 This tool comprised a total of 20 criteria, and studies that met 14 or more (70% or more) were considered to have an acceptable quality (Supplemental Table 1). 24
Data analysis and meta-analysis
All statistical analyses were performed using SPSS 20 (IBM, Armonk, NY, USA) and R version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria). Normally and non-normally distributed continuous variables were presented as means ± SE of the mean and medians (interquartile range), respectively. Categorical variables were presented as frequencies. If original data failed to meet a normal distribution in the meta-analysis, a double arcsine transformation was performed to stabilize the variance in the original ratio. In addition, heterogeneity was evaluated by Q-test and I2 statistics. When p < 0.05 or I2 > 50%, the combined proportions and 95% confidence intervals were calculated using a random-effects model; otherwise a fixed-effects model was used. 25 We also performed subgroup analyses on different types of TNF-α agents. The clinical characteristics of all patients in the meta-analysis are summarized in Table 1 and the results are presented as forest plots with 95% confidence intervals. We failed to peroform the bias assessment since the number of included studies was small.
Clinical characteristics of patients with BD in the included studies for meta-analysis.

ADA, adalimumab; AZ, azathioprine; BD, Behçet’s disease; Col, colchicine; DAIBD, disease activity index for intestinal Behçet’s disease; ETN, etanercept; GGISS, global gastrointestinal symptom score; GI, gastrointestinal; GLM, golimumab; IFX, infliximab; 6-MP: 6-mercaptopurine; MS, mesalazine; MTX, methotrexate; N/A, not available; SSZ, sulfasalazine; TNF-α, tumor necrosis factor alpha.
Means the data of a study in our own institution and was not published before.
The improvement rate was defined as the proportion of patients with gastrointestinal symptoms alleviation or intestinal ulcers decrease ⩾50%. The complete remission rate and healing rate were defined as the proportion of patients with symptoms and ulcers completely disappeared. 22
Different studies evaluated the efficacy at different time periods, and to minimize the influence of heterogeneity between different included studies, we synthesized the rates of gastrointestinal symptoms and intestinal mucosal ulcers at different time points during the therapeutic periods.22,28,30 The results are summarized in Table 2. According to the treatment strategy of anti-TNF-α agents, we evaluated efficacy of symptom improvement at different time points: induction therapy (0–6 weeks), short-term maintenance therapy (10–14 weeks), medium-term maintenance therapy (24–30 weeks), and long-term maintenance therapy (48–54 weeks). For endoscopic examination in intestinal mucosal ulcers, the time points were merged as following: short-term duration (0–24 weeks), long-term duration (24–52 weeks), and longer-term duration (52–104 weeks).
Synthesized therapeutic efficacy evaluation of included studies in meta-analysis.

Results
Case series
Patient characteristics
A total of 11 patients with intestinal BD received anti-TNF-α treatment at our institution (five men and six women). Most of the patients were young adults (mean age: 32.82 ± 13.01 years) and the median disease duration was 1.58 months (range: 0.25–10 months). All patients had intestinal ulcers and clinical manifestations included buccal ulcer and abdominal pain. The typical manifestation of BD (i.e., ulcers in the ileocecal region) was detected in 6 of the 11 patients. The detailed clinical data of the included patients are listed in Table 3.
Clinical characteristic of patients and therapeutic efficacy of anti-TNF-α agents in our institution.

DAIBD, disease activity index for intestinal Behçet’s disease; GI, gastrointestinal; TNF-α, tumor necrosis factor alpha.
Treatment and efficacy assessment
All patients in our case series received infliximab (IFX) treatment. One patient switched to adalimumab (ADA) due to the failure of IFX therapy, and the therapeutic effects were evaluated separately. IFX was administered at a standard dose of 5 mg/kg at 0, 2, and 6 weeks initially, and it was administered every 8 weeks as maintenance therapy. ADA was administered at standard doses of 160 and 80 mg at weeks 0 and 2, and then it was administered at a dose of 40 mg every other week. These biologics were prescribed to the included patients due to conventional therapies failure (n = 4), steroid-dependency (n = 4), and disease flares (n = 4). The mean duration of anti-TNF-α treatment was 48.30 ± 35.93 weeks. Three patients maintained this treatment at present, while others discontinued the treatment for the following reasons: failure to achieve remission at the initiation (n = 2), failure to maintain efficacy (n = 3), and treatment termination owing to symptoms improvement (n = 3).
The median follow-up time was 30.2 weeks (range: 2–149.3 weeks). However, not all patients were required to complete the follow up in every period. The clinical and endoscopic manifestations of patients with intestinal BD are shown in Table 3. No adverse events were reported and no patients discontinued the treatment due to drug-related adverse events.
Meta-analysis
Study selection
Totally 5650 articles were retrieved, and 3729 articles remained for further analysis after excluding duplicates. By screening the titles, abstracts, and article types, 275 clinical studies focused on therapeutic efficacies of anti-TNF-α agents against BD. The full texts of these articles were further analyzed, and 263 studies were excluded owing to insufficient data information. Additionally, one retrospective study that explored efficacy of etanercept was excluded because it failed to provide the assessment criteria and baseline data. 35 Finally, a total of 12 studies including 514 patients were used to perform the meta-analyses by adding the results from our institution.
Study characteristics
Of the 12 included studies, 8 were retrospective studies and 4 were prospective studies.21,22,26–34 Only one retrospective study made a comparison with the control group, 32 while the remaining 11 studies were single-arm type. The population of patients with ADA treatment reported by Inoue et al. 21 was the same as that reported by Tanida et al., 29 but the latter focused on a longer time. All anti-TNF-α agents in the included studies were given a standard dose. Four of these studies investigated IFX and five studied ADA, but the remaining two just referred to TNF-α inhibitors as a whole agent without specifying certain type. For the diagnostic criteria, nine studies were conducted according to the Japanese Behçet’s Disease Research Committee criteria, and other two studies were based on the International Study Group for Behçet’s Disease and the Korean Diagnostic Criteria for Intestinal Behçet’s Disease.5,18,19
The included patients were glucocorticoid-dependent or resistant, unresponsive to other biologics, refractory to conventional treatments (i.e., transient remission was achieved with the use of regular immunosuppressants, and symptoms or intestinal ulcers relapsed even with persistent immunosuppressant treatment). 7 Apart from the anti-TNF-α agents, all patients received other drugs at the same time. The characteristics of the included studies are summarized in Table 1. The quality of each study was assessed and the result was presented in Supplemental Table 1. The studies met 15–19 criteria in the IHE quality assessment tool, and thus, were deemed to have an acceptable quality for inclusion in the analysis.
Anti-TNF-α agents exert therapeutic efficacy in intestinal BD
Anti-TNF-α agents maintain clinical symptom remission during different therapeutic periods
Five studies with 383 patients were included in the evaluation of induction therapy (four studies focused on IFX and one studied ADA). Overall, 71.7% of the patients achieved clinical symptom improvement and 48.6% of them experienced a complete symptom relief. In subgroup analyses, improvement rate of IFX was 79.3% and the complete remission rates for IFX and ADA were 50.7 and 47.4%, respectively (Figure 2(a), Supplemental Figure 1A).

Pooled improvement proportion of clinical symptoms in patients treated by anti-TNF-α agents in induction period (a), short-term (b), medium-term (c), long-term (d), and a longer-term sustain period (100 weeks) (e).
Seven studies with 377 patients were included in the evaluation of short-term maintenance therapy; 59.8% of the patients showed improved clinical symptoms and 53.9% of them achieved complete remission. Moreover, the symptom remission rate of IFX (75%) was higher than ADA (58.6%) by further subtype analyses. However, the complete remission rates were similar between the two agents (Figure 2(b), Supplemental Figure 1B). In addition, 317 patients were observed in the medium-term maintenance therapy period. The overall symptom alleviation and complete remission rates in 317 patients were 73.8 and 60.6%, indicating the therapeutic efficacy could be sustained. In the patients treated with IFX, 77.5 and 66.3% achieved symptom improvement and complete remission, while the corresponding rates for patients treated with ADA were 67.6 and 65.1% (Figure 2(c), Supplemental Figure 1C).
Nine studies including 328 patients evaluated long-term maintenance therapy. The clinical-symptom-remission rate in this period was 73.7%, and 58.7% of these patients received complete resolution. The remission rates in patients who received IFX and ADA were 72.9 and 80.6%, respectively. Moreover, 65.6% of the IFX-treated patients and 58.2% of the ADA-treated patients achieved complete symptomatic remission (Figure 2(d), Supplement Figure 1D). Besides, the therapeutic effect over 100 weeks was also evaluated in 212 patients; 77.8 and 65.4% of the patients achieved remission and complete alleviation of the symptoms, respectively. Especially, the complete remission rate was 86.1% among 20 patients with IFX treatment, but the corresponding rate in patients receiving ADA was 43.7% (Figure 2(e), Supplemental Figure 1E).
Anti-TNF-α agents maintain intestinal ulcer remission during different periods
Nine studies containing 237 patients were included in the short-term period. The overall improvement rate of intestinal ulcers was 74.5%, showing IFX with 78.4% and ADA with 74.6%. The overall rate of intestinal mucosal healing was 46.9%, and IFX and ADA showed similar efficacies (78.4% versus 74.6%) (Figure 3(a) and (d)). During the long-term period, mucosal ulcers were alleviated in 77% of the 120 patients. Subtype analysis found that the improvement rates account for 89.2 and 84.7% in IFX and ADA treatment, respectively. The overall mucosal healing rate was 60.9% in the patents with long-term follow-up and the respective rates of IFX- and ADA-treated patients reached 82.1 and 56.8% (Figure 3(b) and (e)). Furthermore, 80.1% of the included patients (n = 119) showed ulcer improvement even in a longer therapeutic time of 52–104 weeks. Almost all included patients (n = 117) received ADA, and the subtype analysis showed that the rate of improvement in these patients was 80.4% (Figure 3(c)).

Alteration of intestinal ulcers for patients treated by anti-TNF-α agents: (a) pooled improvement proportion in short term, (b) pooled improvement proportion in long term, (c) pooled improvement proportion in longer term, (d) proportion of mucous healing in short term, and (e) proportion of mucous healing in long term.
Safety assessment of anti-TNF-α agents in intestinal BD
Seven studies (four about IFX, two about ADA and the other one without statement of specific subtype) with 153 patients reported adverse events. Briefly, 40 patients (26.1%) had mild infection, especially 2 (1.3%) had serious infection and they discontinued the treatment. Besides, 10 patients (6.5%) experienced infusion reactions and other 10 patients (6.5%) got mild adverse drug reactions.
Discussion
Our findings indicated that anti-TNF-α agents could effectively mitigate clinical symptoms in nearly 70% of the included patients, and the therapeutic efficacy could be sustained over a long period of time. Furthermore, anti-TNF-α agents also contributed to intestinal ulcer improvement, and almost 60% of the patients achieved complete mucosal healing during the long-term period. Further subtype analyses showed IFX exerted its effect within a short period of time, but ADA seemed to work at a slower rate and was likely to be less effective in the clinical symptom improvement during induction and early term periods. In terms of intestinal mucosal ulcer alleviation, ADA and IFX took effects comparably in every therapeutic period. Satisfactorily, only mild adverse events were reported in all included studies. As a whole, the results of our study with larger sample size were more credible than the previous single-arm studies.
This therapeutic effect could be illustrated in terms of the pathogenesis and pathophysiological mechanism of BD. BD arises from a dysregulation of the immune response of T-cells, especially the T helper type 1 (Th1) cells. Multiple cytokines related to Th1 cells have been reported to promote TNF-α production, which eventually results in mucosal damage and contributes to the progress of intestinal BD. 36 With respect to such a pathogenesis, it is conceivable to verify the effectiveness of anti-TNF-α agents against intestinal BD. In contrast to conventional immunosuppressors that extensively work on multiple molecular pathways, anti-TNF-α agents play a more specific and valid role. As a result, patients with intestinal BD unresponsive to conventional treatments might be treated effectively with anti-TNF-α agents.37,38
As IFX and ADA were two subtypes of anti-TNF-α agents which shared a common therapeutic mechanism in intestinal BD, they were mainly studied in most of the included studies. IFX is a chimeric monoclonal antibody, whereas ADA is a fully humanized. Nowadays, ADA has been approved as the standard treatment for intestinal BD in some east Asian countries.5,7,39 However, some discrepancies were noted in the outcomes of IFX and ADA treatments in this study. IFX exerted its effect within a short time from administration. Even in the induction period, almost 80% of the IFX-treated patients have shown improvement of clinical symptoms, and half of them achieved complete resolution. Moreover, the therapeutic effect of IFX was continuous in the middle- and long-term maintenance periods, and most patients (82.1%) sustained long-term mucosal healing. Conversely, ADA worked at a slower rate and appeared less effective in the induction and early term periods. The improvement rate of the clinical symptoms was approximately 50% in the middle- and long-term maintenance periods among the ADA-treated patients. While in terms of the efficacy of mucus ulcer alleviation, ADA seemed comparable to IFX, and there was little difference in the ulcer improvement rates between IFX- and ADA-treated patients in various therapeutic periods analyzed. Interestingly, the characteristics of these two subtypes that took effect in intestinal BD resembled those of inflammatory bowel disease.40,41
This study had some limitations. First, almost all included articles were single-arm studies, and most patients received anti-TNF-α treatment after they received conventional treatments. Thus, direct comparisons could not be made between the anti-TNF-α agents and other conventional medicines. Second, the sample sizes for ADA and IFX in the subgroup analyses were highly diverse. The efficacy of ADA was evaluated in a larger population, while that of IFX was evaluated in a smaller population. Therefore, the overall efficacy of IFX is prone to be affected by the extremely abnormal results of the included studies. Third, studies from different countries adopted multiple criteria to evaluate the disease severity, and the timing of therapeutic efficacy evaluation varied widely across the included studies. This could potentially be a source of significant bias.
A series of measures were taken to moderate the influence of these limitations. We set strict inclusion criteria; only patients diagnosed with intestinal BD according to the criteria definitively were included in this study. Moreover, our analyses only incorporated studies that clearly reported the efficacy evaluation times, then we integrated the heterogeneous estimation time into broad treatment periods according to the medicine administration regimen (Table 2).
This study indicated the effectiveness of anti-TNF-α agents for intestinal BD. To better understand the efficacy of biologics for intestinal BD, more studies about the first-line efficacy of other biologics in addition to anti-TNF-α are necessary, especially their comparison with conventional treatments.
Conclusions
According to this retrospective case series and meta-analysis, anti-TNF-α treatment is effective for clinical symptom remission and intestinal ulcer healing in intestinal BD. Data from our own institution and the results of the meta-analysis indicated that anti-TNF-α agents could alleviate the disease in approximately 70% of the patients who were refractory to conventional treatments. Furthermore, IFX exerted its effect on the clinical symptoms remission within a short period of time, while ADA worked at a slower rate. They took effects comparably in terms of intestinal mucosal ulcer alleviation. In addition, anti-TNF-α treatment was safe with few adverse side effects. In conclusion, anti-TNF-α agents could be another choice for patients with refractory intestinal BD to improve their prognosis. However, future studies should be conducted to investigate the roles of other biologics, especially their efficacy in the first-line treatment of intestinal BD.
Supplemental Material
sj-docx-1-tag-10.1177_17562848221116666 – Supplemental material for Anti-TNF-α agents for refractory intestinal Behçet’s disease: case series and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848221116666 for Anti-TNF-α agents for refractory intestinal Behçet’s disease: case series and meta-analysis by Shukai Zhan, Caiguang Liu, Na Li, Tong Li, Zhenyi Tian, Min Zhao, Dongxuan Wu, Minhu Chen, Zhirong Zeng and Xiaojun Zhuang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-2-tag-10.1177_17562848221116666 – Supplemental material for Anti-TNF-α agents for refractory intestinal Behçet’s disease: case series and meta-analysis
Supplemental material, sj-tif-2-tag-10.1177_17562848221116666 for Anti-TNF-α agents for refractory intestinal Behçet’s disease: case series and meta-analysis by Shukai Zhan, Caiguang Liu, Na Li, Tong Li, Zhenyi Tian, Min Zhao, Dongxuan Wu, Minhu Chen, Zhirong Zeng and Xiaojun Zhuang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.