
Abstract
Gastroesophageal reflux disease (GERD) is a common disease with increasing prevalence worldwide. However, the diagnosis of GERD is challenging because there are no definite gold standard criteria. Recently, a novel impedance parameter, namely mean nocturnal baseline impedance (MNBI), has been proposed, which reflects the burden of longitudinal reflux and the integrity of esophageal mucosa. MNBI has shown an immense promise for increasing the diagnostic rate of multichannel intraluminal impedance-pH (MII-pH) monitoring and predicting the response to proton pump inhibitor (PPI) or anti-reflux intervention in patients with reflux symptoms. The present paper reviews the association between baseline impedance and esophageal mucosal integrity, the acquisition of MNBI in 24-h MII-pH monitoring, the clinical utilization of MNBI in improving the diagnosis rate of GERD in patients with typical reflux symptoms, predicting the response to PPI or anti-reflux treatment in these patients, the utilization of MNBI in diagnosing patients with atypical symptoms or extra-esophageal symptoms, and the correlation between reflux burden and MNBI. MNBI should be routinely assessed using MII-pH monitoring.
Keywords
Introduction
The estimated worldwide prevalence of gastroesophageal reflux disease (GERD) is 8–33%. 1 The diagnosis of GERD is clinically challenging due to the multifactorial pathophysiology mechanisms of GERD, including esophageal mucosal integrity, competent esophagogastric junction, esophageal peristalsis, etc. Upper endoscopy and multichannel intraluminal impedance-pH (MII-pH) monitoring are usually performed to provide objective evidence for pathological reflux. However, 70% of the patients with heartburn have no macroscopic evidence of esophageal mucosal injuries. 2 In addition, the diagnostic sensitivity of conventional metrics [i.e. acid exposure time (AET), symptom association probability (SAP), and symptom index (SI)] in MII-pH monitoring is considered to be suboptimal.3–5 AET is the most useful conventional parameter to distinguish pathological reflux from physiological reflux, but it was normal in 19% of the patients with erosive esophagitis (EE) 3 and nearly 50% of the patients with non-erosive reflux disease (NERD),3,4 possibly due to the day-to-day variability of AET. 6 The diagnostic sensitivity of positive SI (SI > 50%), positive SAP (SAP > 95%), and concordant SAP/SI positivity (SAP > 95% and SI > 50%) for the diagnosis of GERD was 51.06%, 46.81%, and 36.17%, respectively. 5
Recently, the utilization of baseline impedance (BI), which is a surrogate marker of mucosal integrity and is resistant to circadian variations, 7 has been proposed for the diagnosis of GERD clinically. This application is mainly based on the following aspects. The barrier protection of the esophageal mucosa can be impaired by reflux, which may cause dilated intercellular spaces (DIS). In 2011, a seminal study by Farré et al. 8 found that esophageal perfusion with the acidic solution in rabbits induced a significant increase in DIS and a decrease in impedance. Moreover, biopsy specimens from patients with EE or NERD had significant DIS compared to patients with functional heartburn (FH)9–12 and healthy controls,9,10,12–14 indicating DIS was a significant histological abnormality of GERD patients and a known marker of esophageal mucosal integrity.7,11,13 However, the application of DIS is limited in clinical practice because of the complicated protocol and the need for a dedicated esophageal pathologist. Therefore, BI as a surrogate marker of mucosal integrity which is more applicable has been proposed for GERD diagnosis. DIS can increase the permeability of esophageal epithelium and the flow of ion-rich fluid around the cells, resulting in a decrease in the BI of GERD.7,8,11,13,15 In addition, BI is negatively correlated with DIS and AET in the distal esophagus (Table 1).11,13,15 In addition, lower BI can be improved by an effective anti-reflux surgery in patients with proton pump inhibitor (PPI) refractory typical GERD symptoms. 16
The association between BI and DIS.
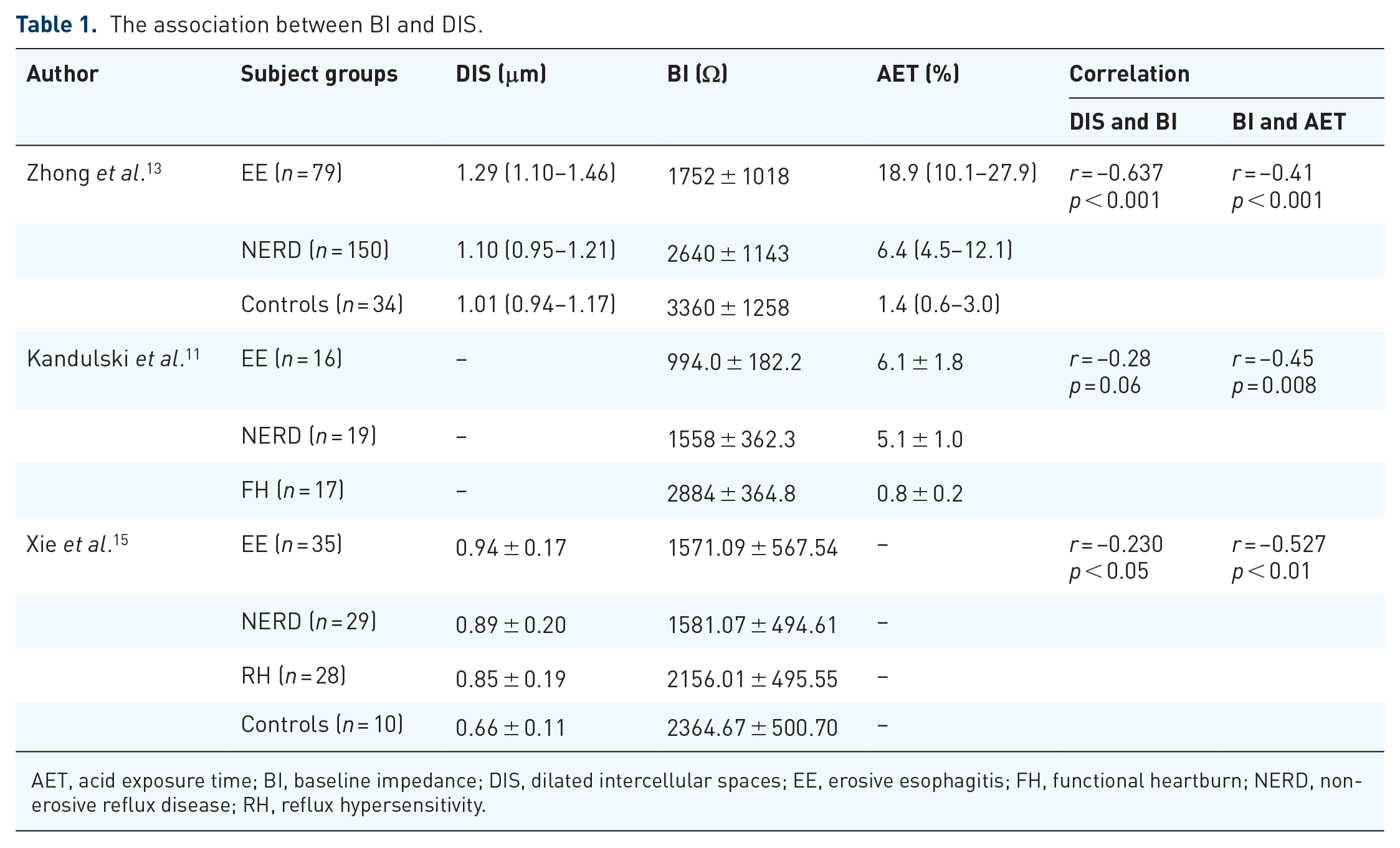
AET, acid exposure time; BI, baseline impedance; DIS, dilated intercellular spaces; EE, erosive esophagitis; FH, functional heartburn; NERD, non-erosive reflux disease; RH, reflux hypersensitivity.
Esophageal BI can be obtained by several ways. It can be determined by MII-pH monitoring during the night avoiding swallows as mean nocturnal BI (MNBI). Also, BI can be acquired from an impedance probe with a high-resolution impedance manometry (HRIM) as BI-HRIM or from a catheter-based probe during sedated endoscopy as mucosal impedance. The MII-pH monitoring technology is widely used clinically. In addition, MNBI as a novel impedance metric can be acquired from available information in an esophageal MII-pH study. Moreover, MNBI can reflect longitudinal reflux burden objectively and has a high inter-observer concordance rate. 4 Therefore, this article reviewed the utility of MNBI in GERD.
The acquisition of MNBI in 24-h MII-pH monitoring
There are six impedance channels (Z1–Z6) in MII-pH monitoring, located at 17, 15, 9, 7, 5, and 3 cm above the lower esophageal sphincter (LES), respectively [Figure 1(a)]. The standardized measurement of MNBI in MII-pH monitoring was obtained by calculating the BI of impedance channel at 3 cm above the LES, which was first proposed by Martinucci et al. 17 Three stable 10-min time periods (around 1 a.m., 2 a.m., and 3 a.m.) avoiding swallows, reflux episodes, artifacts, or pH drops were selected when the patient was in a supine position. Subsequently, the average BI for each time period was computed with the aid of the software [Figure 1(b)]. The BI values of the three time periods were averaged to get the MNBI, which can accurately reflect the BI of a 6-h nocturnal bedtime period. 17 Subsequently, this formula was widely used in most studies. However, there are subtle variations in the selected impedance channel in some other studies, such as the impedance channel at 5 cm above the LES15,18,19 or the distal four channels (mean MNBI value of Z3–Z6). 20

(a) Illustration of a 24-h MII-pH catheter with six impedance channels (Z1–Z6) (located at 17, 15, 9, 7, 5, and 3 cm above the LES, respectively) and an esophageal pH sensor. (b) The acquisition of MNBI. Three stable 10-min time periods (around 1 a.m., 2 a.m., and 3 a.m.) avoiding swallows, reflux episodes, artifacts, or pH drops are selected. The BI values of the three time periods are averaged to obtain the MNBI.
The utilization of MNBI in patients with typical reflux symptoms
Increasing the diagnostic rate of GERD
Previous studies have demonstrated that MNBI can improve the diagnostic rate of GERD in patients with typical reflux symptoms.4,5,15,16,18,19,21–28 Lower MNBI values have been found in EE, NERD, and reflux hypersensitivity (RH) compared with FH and healthy controls.4,15,16,18,19,21–23 Also, MNBI was significantly lower in patients with refractory reflux esophagitis than in those with healed reflux esophagitis and NERD, indicating that low MNBI could reflect the severity of esophageal mucosal damage. 16 In addition, it has been proved to be useful in distinguishing GERD from healthy controls,4,15,21 and distinguishing reflux-related patients (GERD16,18,19,22 and RH22,23) from reflux-unrelated patients (FH) with a high diagnostic accuracy (Table 2). Moreover, MNBI may be particularly useful in patients with inconclusive GERD.27,28
The utilization of MNBI in increasing the diagnostic rate of GERD and predicting the response to PPI or anti-reflux treatment in patients with typical reflux symptoms.

SAP < 95% and SI < 50%.
SAP ⩾ 95% and/or SI ⩾ 50%.
AET, acid exposure time; AUC, area under the curve; CI, confidence interval; EE, erosive esophagitis; FH, functional heartburn; GERD, gastroesophageal reflux disease; GSS, global symptom severity; HC, healthy controls; HRE, healed reflux esophagitis; LES, lower esophageal sphincter; MII-pH, multichannel intraluminal impedance-pH; MNBI, mean nocturnal baseline impedance; NERD, non-erosive reflux disease; PPI, proton pump inhibitor; RH, reflux hypersensitivity; RRE, refractory reflux esophagitis; SAP, symptom association probability; SI, symptom index.
Separating GERD from healthy controls
As far as we know, three studies evaluated the value of MNBI in distinguishing GERD from healthy controls.4,15,21 Frazzoni et al. 4 prospectively conducted a multicenter study on 289 GERD patients and 50 healthy controls in Italy who underwent 24-h MII-pH monitoring, showing that 2292 Ohm (Ω) could be used as the cutoff impedance values to discriminate GERD from healthy individuals. Subsequently, the fixed MNBI threshold (2292 Ω) was used by many studies16,20,27–30 and was mentioned in the Lyon Consensus. 32 Recently, a large multicenter cohort from Italy enrolled 488 patients with PPI-dependent heartburn and 70 healthy controls found that MNBI showed high efficiency in identifying patients with PPI-dependent heartburn with an area under the curve (AUC) of 0.89 at a cutoff value of 2000 Ω. 21 However, the normative MNBI thresholds may vary between ethnicities and regions. Another study from China suggested that 1764 Ω can be used as the MNBI threshold to distinguish patients from healthy individuals, which involved 92 patients with typical reflux symptoms and 10 healthy controls. 15 Given this, the cutoff value of pathological MNBI may be lower in Asia than in Europe. Future studies involving normative MNBI values of different ethnicities and regions are warranted.
Distinguishing NERD from FH
It is crucial to distinguish GERD from non-GERD for prescribing different treatments. The diagnosis of NERD may be missed if only based on the conventional pH-impedance metrics. MNBI analysis could complement conventional pH-impedance metrics in differentiating GERD from FH in patients with typical reflux symptoms, which was crucial for prescribing different treatments. Frazzoni et al. 4 showed that MNBI could improve the diagnostic rate of NERD classified by Rome III criteria. Abnormal MNBI can identify NERD patients who may not be confirmed by conventional metrics in MII-pH monitoring (AET and SAP/SI). 83% (183/216) of NERD patients can be confirmed using AET and SAP/SI. 4 When adding cases whose only abnormality was an abnormal MNBI, the proportion of diagnosed NERD was significantly increased. 4 Sun et al. 33 found that 16.67% (13/78) of FH diagnosed by conventional parameters in 24-h MII-pH monitoring may be GERD patients according to abnormal MNBI. If the MII-pH monitoring period prolongs to 48 h, 72 h, or 96 h, the 16.67% (13/78) patients who were classified as FH by conventional metrics in 24-h MII-pH monitoring can be re-classified as NERD. 33 Moreover, previous studies have demonstrated that MNBI can be useful for distinguishing NERD from FH with high AUC, high sensitivity, and specificity off PPI or on PPI therapy (Table 2).16,18,19,22
Separating RH from FH
It is important to differentiate RH from FH in the clinic because RH may also benefit from anti-reflux therapy. 34 Patients with RH and FH have no objective evidence of reflux (normal endoscopy and normal AET), but there is a positive reflux-symptom association (positive SAP or SI) in patients with RH. 35 However, a negative SAP/SI may not rule out RH. SI and SAP rely excessively on the accuracy of patients’ records and patients may not perceive symptoms during 24-h MII-pH monitoring. In addition, SAP and SI can be influenced by day-to-day variability, degree of reflux, and length of monitoring in patients with reflux symptoms. 36 Moreover, the positive reflux-symptom association may be influenced by low reflux events. 36
Even in the case of normal reflux events, MNBI as an objective metric can differentiate RH from FH.22,23,31 Recently, studies have found that MNBI was significantly lower in RH than in FH and it can separate RH from FH independently of SAP and SI (Table 2).22,23 In addition, the MNBI of PPI responders was significantly lower than that of PPI non-responders among patients with FH. 31 Also, the MNBI value of PPI responders in patients with FH was similar to that of patients with RH, indicating that PPI responders in FH patients may be classified as RH based on MNBI. 31 RH is characterized by DIS, which can explain the increased perception of reflux events and the positive response to anti-reflux treatment. 22 Therefore, the MNBI should be evaluated to help physicians to distinguish between RH and FH if reflux-symptom association afford uncertain results (i.e. poor accuracy in symptom recording, or discordant SAP and SI).
Acting as supportive evidence for inconclusive GERD
The Lyon Consensus has proposed stricter criteria for GERD diagnosis. MNBI has been proposed as an adjunctive evidence for patients with inconclusive GERD (AET 4–6%, Los Angeles A or B esophagitis, or reflux events 40–80) by the Lyon Consensus. 32 Several studies have demonstrated that MNBI may be particularly useful in patients with inconclusive results of traditional variables in MII-pH monitoring.21,27,28
A study involving two tertiary medical centers by Rengarajan et al. 27 demonstrated that inconclusive AET (4–6%) can be divided into two categories based on whether MNBI is abnormal. 91.8% (67/73) of patients had abnormal MNBI (<2292 Ω) among patients with inconclusive AET. Among patients with abnormal MNBI, 73.1% (49/67) of patients responded to anti-reflux therapy, which was comparable to that seen with pathological AET [75.7% (84/111)]. 27 However, among patients with normal MNBI (>2292 Ω), 33.3% (2/6) of patients responded to anti-reflux therapy, which was similar to patients with physiological AET (27/70, 38.6%). 27 Recently, Frazzoni et al. 21 conducted a large multicenter cohort of 488 patients with PPI-dependent heartburn and with 70 healthy controls, which found that the diagnosis of GERD was confirmed by MNBI in 75% of patients with inconclusive AET (4–6%), showing the high clinical value of MNBI for the diagnosis of GERD in such cases. Ribolsi et al. 28 performed a multicenter study that enrolled 233 patients with typical reflux symptoms in Italy, which showed that pathological MNBI (<2292 Ω) was significantly associated with PPI response in inconclusive GERD patients. In addition, MNBI can distinguish between PPI responders and PPI non-responders among inconclusive GERD patients with an AUC 0.89 at a cutoff value of 1916 Ω, with a sensitivity of 80% and a specificity of 91.4%. 28 All these studies demonstrated that abnormal MNBI can sway clinical impression toward conclusive GERD in patients with inconclusive GERD.21,27,28 Evaluation of MNBI may be especially crucial for inconclusive GERD patients if they are candidates for anti-reflux surgical or endoscopic interventions.
The use of MNBI in predicting the response to PPI or anti-reflux therapy
The currently available literature has demonstrated that MNBI was significantly lower in responders than in non-responders to PPI or anti-reflux therapy, and MNBI can predict the response to PPI or anti-reflux therapy in patients with typical reflux symptoms (Table 2).15,17,20,27–31 Some studies pointed out that abnormal MNBI (<2292 Ω) was independently associated with PPI response or anti-reflux therapy in patients with typical reflux symptoms.20,27,28 Likewise, some other studies found that MNBI > 2292 Ω 30 or MNBI > 1764 Ω 15 was associated with PPI failure in patients with typical reflux symptoms. Frazzoni et al. 29 found that MNBI can predict the symptomatic response to PPI treatment better than AET (AUC 0.742 versus AUC 0.687, p = 0.003). In addition, among FH patients, the MNBI was significantly lower in PPI responders than in PPI non-responders, and MNBI can also predict the response of these patients to PPI.17,31 Furthermore, MNBI may be of particular value in identifying patients who were responsive to PPI or anti-reflux therapy in patients with inconclusive GERD, which can help identify GERD patients among these patients.27,28
The use of MNBI in diagnosing patients with atypical symptoms or extra-esophageal symptoms
Few data are available concerning MNBI in patients with atypical symptoms or extra-esophageal symptoms (EES).37–42 Zhong et al. 37 demonstrated that in MII-pH monitoring, the BI (Z2–Z6) of GERD patients with chest pain syndrome and EES was significantly lower than that of healthy controls. Ribolsi et al. 38 studied 239 EES patients in Italy. They showed that distal MNBI (3 cm above the LES) was significantly lower in patients with PPI response than in those with PPI non-response. And abnormal MNBI (<2292 Ω) was associated with PPI response in patients with EES. 38 In addition, Sakin et al. 39 displayed that proximal-to-distal BI ratio [(mean Z1 + Z2)/(mean Z5 + Z6)] can be useful in diagnosing patients with laryngopharyngeal reflux (LPR) symptoms. Moreover, Chen et al. 40 found that proximal MNBI (15 or 17 cm above the LES) can not only identify patients with LPR, but also predict outcomes to anti-reflux therapy. However, some other studies noted that MNBI was not sufficient to evaluate patients with EES.41,42 Doo et al. 41 showed that there was no significant difference in the MNBI values of distal and proximal esophageal (Z6 and Z3, respectively) between patients with LPR and healthy controls. In addition, Zikos et al. 42 found that there was no correlation between distal/proximal MNBI and EES. Whether MNBI can improve the diagnostic rate of GERD patients or predict the response to anti-reflux therapy in patients with EES or atypical symptoms is an open question to be explored in future studies.
Correlation between reflux burden and MNBI
Previous studies showed that MNBI was significantly lower in patients with AET > 6% than in patients with AET 4–6% or in patients with AET < 4%.21,43 The proportion of abnormal MNBI was significantly higher in patients with AET > 6% or AET 4–6% than in patients with AET > 4%. 27 Ribolsi et al. 44 prospectively performed a multicenter study that enrolled 230 patients with dominant typical esophageal symptoms, which demonstrated that AET was negatively correlated with MNBI values. In addition, AET > 4% was significantly associated with abnormal MNBI values. 44 The correlation between AET and MNBI may be that the increased reflux burden results in the impaired integrity of esophageal mucosa, as shown by decreased MNBI values.
Concerns and future directions
The calculation of MNBI is easy to obtain from MII-pH monitoring. In addition, just like glycated hemoglobin A1c versus blood glucose measurement in diagnosing diabetes mellitus, we thought that MNBI might be more stable and reflect relatively longer periods of reflux when comparing with conventional parameters, such as AET and SAP/SI, etc. However, there are concerns about the reliability of the MNBI measurement. If the impedance sensors are not in close contact with the esophageal mucosa due to the presence of reflux episodes and swallows, 19 or calculation of MNBI is influenced by artifacts and pH drop, MNBI may be compromised. Given this, when analyzing the MNBI value, we should select three 10-min time periods with caution to avoid reflux episodes, swallows, artifacts, and pH drop. 17 Moreover, low MNBI can be observed not only in GERD patients, but also in the presence of eosinophilic esophagitis 45 and severe esophageal motility disorders, such as absent peristalsis and achalasia, 46 which should also be considered.
Notably, the spectrum and diagnostic criteria of GERD vary across different studies. RH is included in the GERD phenotype in the Rome III criteria. 47 However, it has been excluded from the GERD phenotype and included in the spectrum of functional disorders in Rome IV criteria. 35 In addition, the diagnostic criteria for GERD vary among studies. The Lyon Consensus proposed stricter criteria for GERD diagnosis, including advanced grades of EE (Los Angeles C or D esophagitis), AET > 6%, long-segment Barrett’s esophagus, or peptic esophageal stricture. 32 However, GERD was defined by lower AET thresholds (AET > 4%15,18,19,26 or AET > 3.2% 16 ) or defined by macroscopic evidence of esophageal mucosal injuries regardless of grades in some previous studies.4,15,26 Although previous studies had adopted different diagnostic criteria of GERD, they have consistently shown that MNBI can reflect esophageal mucosal integrity and can display the clinical value of MNBI for the diagnosis of GERD in patients with reflux symptoms.
In addition, because MNBI cannot be obtained from software analysis automatically, it takes extra minutes to calculate MNBI during the manual analysis of tracings. The previous study has claimed that artificial intelligence (AI) can accurately and instantaneously extract meaningful metrics from pH-impedance monitoring by automating the recognition, censoring, and removal of esophageal events. 48 We believe that MNBI may be automatically extracted by AI in the future.
Conclusion
As an objective and reproducible parameter for MII-pH monitoring, MNBI can not only improve the diagnostic rate of GERD in patients with reflux symptoms, but also predict the response to PPI or anti-reflux therapy in these patients. Therefore, MNBI should be routinely assessed using MII-pH monitoring.