
Abstract
Background:
The association between intraductal papillary mucinous neoplasms (IPMNs) and colorectal cancer (CRC) and polyps is controversial.
Objectives:
To compare the prevalence of CRC and colorectal polyps among patients with IPMN and matched average risk individuals.
Methods:
A match cross-sectional historical study comparing colonoscopy findings of 310 patients with IPMN cysts who underwent at least one colonoscopy examination from 2004 through 2019, with 310 age- and gender-matched average risk participants who underwent a screening colonoscopy. CRC and polyps were assessed in both groups. The prevalence and odds ratio were calculated.
Results:
CRC was diagnosed in 16 of 310 patients with IPMN (5.2%), and at least one polyp was detected in 96 patients (31%). The prevalence of CRC was greater among patients with IPMN than in matched individuals [5.2% versus 1.3%, p = 0.012, prevalence odds ratio (POR) 4, confidence interval (CI) 1.29–16.44]. The overall prevalence of polyps was not higher among patients with IPMN than in matched individuals (31% versus 26.8%, p = 0.291, POR 1.22, CI 0.85–1.76). However, the prevalence of colorectal adenomas with high-grade dysplasia was higher in patients with IPMN than in matched individuals (4.2% versus 1%, p = 0.02, POR 4.33, CI, 1.19–23.7). The prevalence of large polyps (i.e. more than 20 mm in size) was also greater in patients with IPMN than in matched individuals (6.1% versus 1.9%, p = 0.011, POR 3.6, CI, 1.29–12.40).
Conclusion:
Patients with IPMN have a significantly higher prevalence of CRC and advanced polyps than the average risk population. In view of our findings, we suggest that once the diagnosis of IPMN is made, special consideration of CRC should be undertaken.
Introduction
Pancreatic cysts are a common incidental finding on abdominal imaging. Their prevalence ranges from 2.4% to 13.5% in asymptomatic populations, and their incidence increases with age. 1 Intraductal papillary mucinous neoplasms (IPMNs) are the most common pancreatic cysts. Previous studies indicate an increased incidence of extra-pancreatic malignancies (EPMs) in patients with IPMNs compared to the general population2–7 as well as compared to non-IPMN cysts.2,3,8 The incidence of EPMs among patients with IPMN ranges from 10% to 52% according to previous studies.2–4,6,9–14 Gastric cancer2,3,5,6,15 and colorectal cancer (CRC)2–7,14,15 are the most common EPMs in patients with IPMN cysts.
It has been suggested that the increased incidence of EPMs in patients with IPMN is associated with the performance of repeated imaging studies for IPMN surveillance, which leads to incidental malignancies detection, or to common environmental, hereditary, or immunological factors. 3 The carcinogenic course of IPMNs and adenomatous colorectal polyps is similar in that both share a sequence of progression from adenoma with low-grade dysplasia through adenoma with high-grade dysplasia (HGD) to an invasive tumor. In addition, there may be common genetic alterations to IPMNs and the progression of adenomatous polyps in the colon, for example the existence of a K-ras mutation.16,17
So far, only few studies have addressed the prevalence of colorectal polyps in patients with IPMN, and the association between IPMN and CRC and polyps is still controversial.3,4,10,18 The aim of our study was to determine the incidence of colorectal polyps and cancer in patients with IPMN, compared to the general average risk population.
Methods
Study population
The study population included all (N = 310) patients aged 18 years and above, who underwent an endoscopic ultrasound examination (EUS) at Tel Aviv Sourasky Medical Center, who were diagnosed with an IPMN cyst, and who underwent at least one colonoscopy between 2004 and 2019. The control group included all average risk patients (N = 4408) who underwent a screening colonoscopy at Tel Aviv Medical Center between 2004 and 2019. Pregnant women, patients under 18 years old, patients with any gastrointestinal disease (including family history of CRC), and patients with poor preparation/incomplete colonoscopy were excluded. For each patient, data were retrieved from the first colonoscopy during the study period, to avoid a selection bias. A pairing was performed in a ratio of 1:1 between those with a pancreatic IPMN and those who underwent a screening colonoscopy (total N = 620). Pairing was done by sex and age (±1 year). Un-paired patients were excluded from the study (N = 0).
All data were retrieved from Tel Aviv Sourasky Medical Center computerized data.
Pancreatic cyst data were retrieved from the EUS examination report, cytology/pathology report, and laboratory results. The following parameters were collected: indication for EUS exam, cyst size, cyst location, presence of worrisome features and/or high-risk stigmata 19 (including mural nodule, thickened wall, intra-cystic mass, and pancreatic duct dilation), cyst fluid carcinoembryonic antigen level (ng/ml), cyst fluid amylase level (IU/l), cyst fluid cytology report, clinical decision, sonographic follow-up, and pathology if available. Cyst type, as well as mucinous versus non-mucinous distinction, were determined by two blinded pancreatobiliary experts from the advanced endoscopy unit at Tel Aviv Sourasky Medical Center, based on clinical, laboratory, and radiologic findings. Cysts were categorized into branch duct IPMN (BD-IPMN), main duct IPMN (MD-IPMN), and mixed-type IPMN.
Colorectal polyps and cancer data were retrieved from the first colonoscopy examination report and from the relevant pathology report. The following parameters were collected: indication for colonoscopy, polyp number, size, location, histology, and level of dysplasia.
Statistical analysis
Categorical variables were reported as frequencies and percentages. Age and age at EUS were reported as mean and standard deviation. Cyst size and amylase were skewed and reported as median and interquartile range. The two cohorts were matched according to age [age at colonoscopy (±1 year)] and gender. McNemar test was used to compare the categorical variables between the two matched groups, and Willcoxon test was used to compare the continuous and ordinal variables. All statistical tests were two-sided, and p < 0.05 was considered as statistically significant. SPSS software was used to conduct all statistical analysis (IBM SPSS statistics for windows version 25, IBM corp., Armonk, New York, USA, 2017).
Results
In all, 1762 patients were diagnosed with a pancreatic cyst in our medical center between 2004 and 2019, out of them 373 also underwent a colonoscopy examination. In all, 310 patients who were diagnosed with an IPMN on EUS were included in this study. There was no specific time relation between the two endoscopic procedures (the EUS could be done before or following colonoscopy). The median patient age was 70.1 years (63.9–77.4) (Table 1). EUS indications and findings are presented in Table 1.
IPMN characteristic.

CEA, carcinoembryonic antigen; FNA, fine needle aspiration.
Cyst detection modality: CT, computed tomography scan; ERCP, endoscopic retrograde cholangiography; EUS, endoscopic ultrasound; MRI, magnetic resonance imaging; US, ultrasound.
Pancreatic cyst type: BD, branch duct; Hx, history; IPMN, intraductal papillary mucinous neoplasm; MCN, mucinous cystic neoplasm; MPD, main pancreatic duct; pNET, cystic pancreatic neuroendocrine tumor; SCA, serous cystadenoma.
N/A, non-available
Cyst detection modality was documented only for cysts that were not detected on index EUS.
In total, 289 patients out of 310 (93.2%) were diagnosed with BD-IPMN, 18/310 (5.8%) with mixed-type IPMN, and 3/310 (0.9%) with MD-IPMN. Information regarding cyst fluid and cytology is presented in Table 1, and information regarding colonoscopy indications in patients diagnosed with pancreatic cyst is presented in Table 2.
Colonoscopy indications in patients diagnosed with IPMN (n = 310).
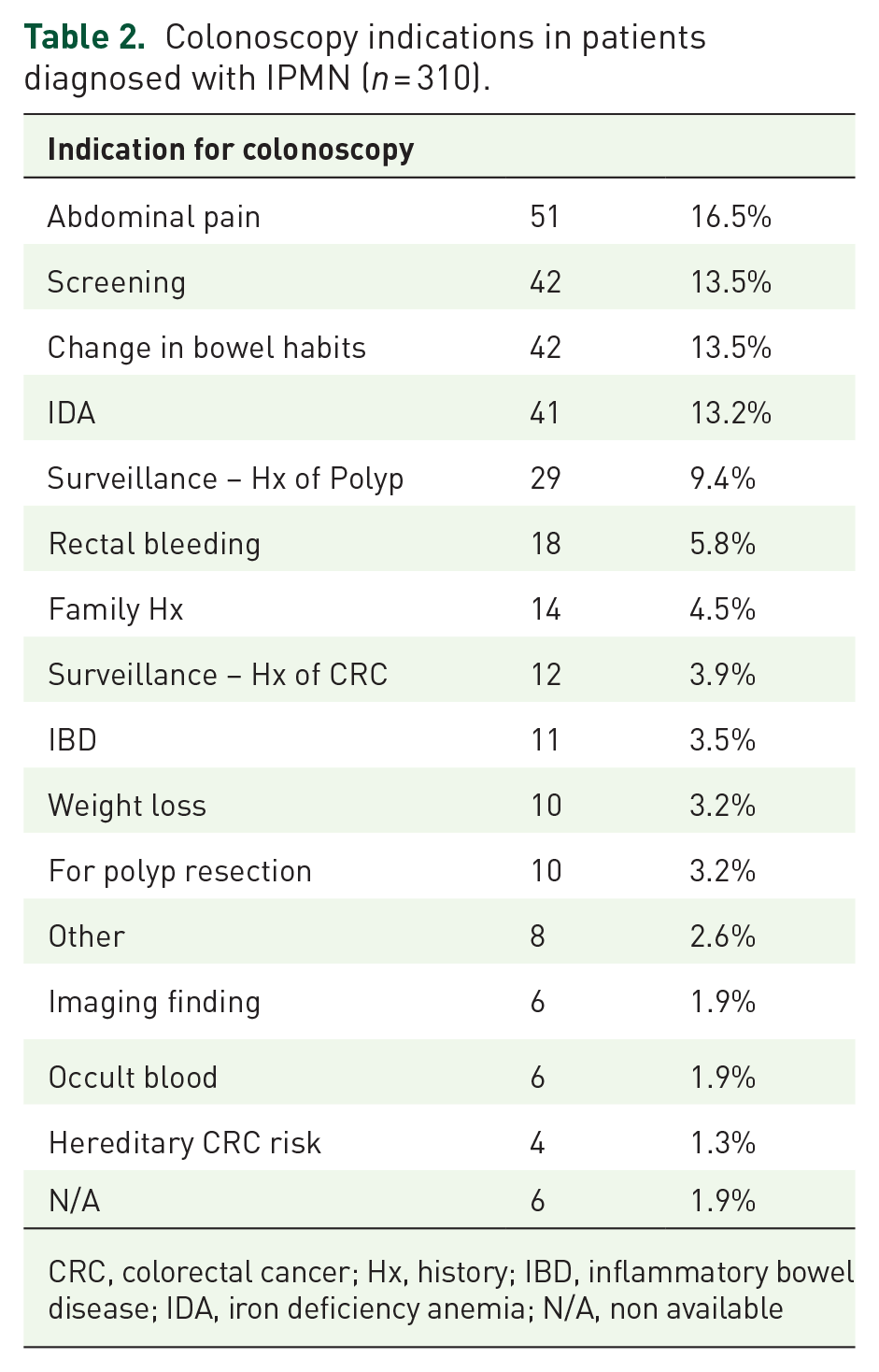
CRC, colorectal cancer; Hx, history; IBD, inflammatory bowel disease; IDA, iron deficiency anemia; N/A, non available
Among patients with IPMN cysts, the prevalence of CRC was significantly higher compared to age and gender paired controls: 16/310 (5.2%) versus 4/310 (1.3%), respectively [p = 0.012, prevalence odds ratio (POR) 4, confidence interval (CI) 1.29–16.44] (Table 3). The overall prevalence of colorectal polyps was similar among patients with IPMN compared to the paired group, 96/310 (31%) versus 83/310 (26.8%), respectively (p = 0.291, POR 1.22, CI 0.85–1.76) (Table 3). Interestingly, there was no significant difference in the prevalence of polyps between IPMN patients who had worrisome features and/or high-risk stigmata 19 , compared to the paired group, 14/40 (31.8%) versus 14/40 (31.8%), respectively (p > 0.999). In addition, no significant difference was found in the presence of CRC between these groups, 4/40 (9.1%) versus 1/40 (2.3%), respectively (p = 0.375).
Colonoscopy findings in patients with IPMN versus matched individuals.

CIS, carcinoma in situ; CRC, colorectal cancer; HGD, high-grade dysplasia; IPMN, intraductal papillary mucinous neoplasm; LGD, low-grade dysplasia; TA, tubular adenoma; TVA, tubule-villous adenoma; VA, villous adenoma.
The prevalence of advanced histological polyps classified as HGD adenomas was significantly higher in patients with IPMN-type pancreatic cyst, when compared to the paired group, 13/310 (4.2%) versus 3/310 (1%), respectively (p = 0.021, POR 4.33, CI 1.19–23.7) (Tables 3 and 4). In addition, the prevalence of large polyps (20 mm or more) was found to be significantly higher in patients with IPMN compared to the paired group, 19/310 (6.1%) versus 6/310 (1.9%), respectively (p = 0.011, POR 3.6, CI 1.29–12.4) (Tables 3 and 4).
Advanced polyps among IPMN patients versus matched individuals.

Significant associations (p value <0.05) appear in boldface.
CI, confidence interval; CIS, carcinoma in situ; HGD, high-grade dysplasia; IPMN, intraductal papillary mucinous neoplasm; LGD, low-grade dysplasia; POR, prevalence odds ratio.
Discussion
This current study assesses the prevalence of polyps and CRC in patients with IPMN, compared to an average risk, age- and gender-matched population. We have compared colonoscopy findings in IPMN patients to an average risk population of individuals, age and sex matched, while previous studies have compared their group of interest to individuals with pancreatic adenocarcinoma,3,10,16 individuals with other types of pancreatic cysts,2,3 or to the general population, age and sex matched.4,7,9,18,20
Our findings support previous studies observing an increased incidence of CRC in patients with IPMN.6,7,12 Notably, the results of our study indicate a significantly higher prevalence of advanced polyps, determined by size (larger than 20 mm) or by histology (HGD), among patients with pancreatic IPMN.
This study has several limitations: First, we compared polyps and cancer in the IPMN group, referred for a variety of colonoscopy indications (only 13.5% were of screening), to the average risk controls. Naturally, this may confound the result, and could potentially serve as a selection bias, as patients with history of ‘red flags’ are more likely to have findings on endoscopy. We did not compare them to consecutive patients since our center is a referral center for large polypectomies, which could have underestimated the difference between groups. Regardless, we aimed to examine the increased risk in patients with IPMN in general. Comparing IPMN to the average risk population serves to highlight the increased risk for neoplasia in these patients. IPMN is probably a marker for advanced findings, and so patients with colon cancer are more prone to be symptomatic. Our study design serves to delineate this difference. Second, there is missing data regarding the existence of pancreatic cysts in our control average CRC risk group. However, this limitation might actually strengthen the power of our results, since the control group might have harbored IPMNs that should have weakened our observation. Third, a high median age of 70.6 years of the cohort (63.1–77.2), could serve as a variable cofounder, since older age is a risk factor of malignancies, colorectal polyps and cancer, and of IPMN. Fourth, missing clinical data, including smoking and other potential risk factors for developing colorectal polyps and cancer, could have impacted our results. Fifth, lack of IPMNs histopathological specimens and genetic tests also limited our ability to investigate shared molecular mechanisms for IPMN and CRC. Moreover, we had a few cases of missing polyp’s histological data. Those cases were excluded from the final analysis to avoid bias. As a result, it is possible that the prevalence of advanced colorectal polyps is even higher than described in this work. As for the study design, it should be noted that this study is a cross-sectional study, so there is no information regarding the time relationship between the appearance of findings in the pancreas and colon. However, it is known from previous studies that EPMs can occur years following surgical IPMN resection. Therefore, a temporal relationship between processes is likely irrelevant.
The key finding suggests a strong association between CRC and advanced polyps and IPMN. This aspect is essential and relevant for surveillance programs and has been analyzed in very few studies. Pancreatic-oriented imaging modalities may misdiagnose and underestimate the prevalence of colorectal polyps, considering their low sensitivity for colonic luminal findings. Therefore, we relied on endoscopic findings, as colonoscopy is the gold standard for colorectal polyp identification. Kato et al. 21 suggested that EPMs are more frequent in malignant (7/14, 50.0%) than in benign (8/36, 21.6%) IPMN patients. We assessed the presence of worrisome features and/or high-risk stigmata, which are known as risk factors for cyst’s malignant development, in respect to the relevant colonoscopy findings, but found no such association. However, the number of IPMN cysts having worrisome features/high-risk stigmata was too small to reach a statistical significance.
In conclusion, this study demonstrates that among patients with IPMN, there is a significantly increased prevalence of CRC and advanced colorectal polyps compared to average risk population. Further work is needed to elucidate the underlying pathophysiology of these findings. Currently, there are no specific guidelines regarding the extent of colorectal screening programs for patients with pancreatic cysts. We suggest that patients with IPMNs be classified as a high-risk population for colorectal malignancy and offered a more rigorous colorectal surveillance program. The intensity of such a program should be determined by further studies.
Footnotes
Ethics approval and consent to participate
The study was approved by the local institutional ethics committee of Tel-Aviv Sourasky Medical Center (0780-19- TLV, 21/6/2020). Informed consent was waived by the ethics committee, due to the retrospective nature of this study. The reporting of this study conforms to the STROBE statement.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.