
Abstract
Background:
Endoscopic treatments are increasingly being offered for refractory gastroesophageal reflux disease (GERD). Three procedures have similar concepts and techniques: antireflux mucosectomy (ARMS), antireflux mucosal ablation (ARMA), and antireflux band ligation (ARBL); we have collectively termed them antireflux mucosal intervention (ARMI). Here, we systematically reviewed the clinical outcomes and technical aspects.
Methods:
The PubMed, Embase, and Cochrane Library databases were searched from inception to October 2021. The primary outcome was the clinical success rate. The secondary outcomes were acid exposure time, DeMeester score, need for proton pump inhibitors (PPIs), endoscopic findings, and adverse events.
Results:
Fifteen studies were included. The pooled clinical success rate was 73.8% (95% confidence interval (CI) = 69%–78%) overall, 68.6% (95% CI = 62.2%–74.4%) with ARMS, 86.7% (95% CI = 78.7%–91.9%) with ARMA, and 76.5% (95% CI = 65%–85.1%) with ARBL. ARMI resulted in significantly improved acid exposure time, DeMeester score, and degree of hiatal hernia. Furthermore, 10% of patients had dysphagia requiring endoscopic dilatation after ARMS or ARMA, and ARMS was associated with a 2.2% perforation rate. By contrast, no bleeding, perforation, or severe dysphagia was noted with ARBL. Severe hiatal hernia (Hill grade III) may predict treatment failure with ARMA.
Conclusions:
The three ARMI procedures were efficacious and safe for PPI-refractory GERD. ARMA and ARBL may be preferred over ARMS because of fewer adverse events and similar efficacy. Further studies are necessary to determine the optimal technique and patient selection.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is one of the most common gastrointestinal diseases, with a prevalence of approximately 10%–30%. 1 Although most patients respond to optimized medical therapy including proton pump inhibitors (PPIs),2,3 up to 40% remain symptomatic despite persistent PPI use, and nearly one-third develop relapse and require long-term PPI.4,5
Antireflux surgery is typically considered in patients with PPI-refractory symptoms or in PPI-dependent patients who do no desire long-term PPI use. 6 Long-term PPI use may increase risks of fracture, infection, and various gastrointestinal malignancies, such as gastric and colorectal cancer. 7 However, antireflux surgery is relatively invasive, and postoperative complications, such as dysphagia and gas bloating, are not uncommon.8,9 Antireflux endoscopic treatment is an emerging alternative for antireflux surgery. It aims to augment the lower esophageal sphincter (LES) through various techniques, such as radiofrequency ablation, 10 endoscopic fundoplication,11–13 and antireflux mucosectomy (ARMS).8,14,15
ARMS is performed using current standard devices for subcircumferential resection of the cardiac mucosa, and the ulcer healing process results in a tightened gastroesophageal junction (GEJ), which improves reflux symptoms. Since the pilot study in 2014, 16 an increasing number of reports have been published.8,14,15,17–23 Moreover, two variants of ARMS have been subsequently reported: antireflux mucosal ablation (ARMA)24–26 and antireflux band ligation (ARBL).27–29 The three procedures not only share the common mechanism of creating artificial ulcers and fibrosis at the GEJ by mucosal intervention but also use preexisting techniques and devices. They thus represent a specific type of antireflux endoscopic treatment, and we introduce a novel collective term – antireflux mucosal intervention (ARMI) – for these procedures.
However, most studies on ARMI procedures have included limited case numbers, and the optimal technique remains unclear. As the use of ARMI procedures has becomes more widespread, it is critical to evaluate their clinical efficacy, safety, and improvements of objective parameters, such as endoscopy and pH testing. Therefore, in this systematic review, we investigated the clinical outcomes and technical aspects of ARMI procedures.
Methods
Techniques of ARMI procedures
The ARMI procedures comprised ARMS, ARMA, and ARBL, although there were different descriptions and slight variations of the techniques among the studies. ARMS involves the resection of a substantial portion (typically 240°–270°) of the mucosa at the GEJ by either endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD). ARMA refers to endoscopic thermal ablation of the mucosa at the GEJ. By contrast, in ARBL, rubber bands are employed at the GEJ without resection to achieve tissue ischemia and subsequent mucosal sloughing.
Search strategy
We searched the PubMed, Embase, and Cochrane Library databases from inception to October 2021 by using an identical search strategy (summarized in Appendix 1). After excluding duplicate records, two authors (J.-H.Y. and C.-T.L.) conducted independent reviews of the included references to identify potentially eligible studies through predefined selection criteria (described in the next section). We also attempted to identify any additional study that was not included in the initial search process. In the case of discrepancies, consensus was made by mutual discussion or consultation with the corresponding author (W.-L.W.).
Selection criteria and data extraction
We included studies evaluating the clinical outcomes of PPI-refractory or PPI-dependent patients who underwent ARMI procedures. To reduce bias from the technical learning curve, we analyzed only reports including more than 10 cases in the cohort. Notably, only the most recent study from a specific group was considered eligible in the systematic review, because several groups continuously reported their updated outcomes as the cohort accumulated more cases. The other exclusion criteria were as follows: (1) combination with other antireflux procedures such as plication or suture, (2) animal studies, (3) non-English studies, and (4) lack of clinical outcomes (improvement of symptoms or changes in esophageal pH/motility tests).
For eligible studies, the following data were extracted: name of the first author, year of publication, number and characteristics of patients, study design, and treatment modality. We also recorded the clinical outcomes at baseline and postoperatively, including severity of symptoms, need for PPI, endoscopic findings, acid exposure time (AET), and DeMeester score. Perioperative metrics and adverse events were also recorded. All data were extracted as originally stated or after appropriate calculations. If the necessary data were unavailable, we attempted to contact the corresponding author for the necessary information.
Study outcomes, statistical analysis, and risk-of-bias assessment
The primary outcome in this systematic review was clinical success, which referred to the proportion of patients who had ⩾50% symptomatic improvement compared with baseline, and it was embraced in many included studies as the primary endpoint.14,15,19–21,24,29 The secondary outcomes were the changes in the following score: symptom score, AET, and DeMeester score; need for PPI postoperatively; procedure time; endoscopic findings; and adverse events.
In this review, meta-analysis was performed only for clinical success rate, proportion of PPI discontinuation, and adverse events after ARMI procedures, due to scarce data and heterogeneity of other outcome parameters. The analysis was performed using comprehensive Meta-Analysis Version 3.3.070 (Biostat, Englewood, NJ, USA) with random-effects models. Corresponding 95% confidence intervals (CIs) were used to evaluate the pooled outcomes. Heterogeneity was measured using the I2 statistic, which was considered statistically significant at >50% or if a chi-square test result indicated p < 0.1. Funnel plots were not used because of the limited number of studies within meta-analyses.
For the risk-of-bias assessment, the Newcastle–Ottawa scale was used for most included studies, which included nonrandomized cohorts. However, the Cochrane risk-of-bias assessment tool (ROB 1.0) was used for the only randomized control trial by Seleem et al. 27
Results
Baseline characteristics of the included studies and patients
After the review process with the predefined selection criteria, 15 studies were considered eligible for the review,8,14,15,17–22,24,25,27–30 (Table 1 and Figure 1): nine used ARMS,8,14,15,17–22 three used ARMA,24,25,30 and three used ARBL27–29 as the main procedure. Most studies were designed as single-arm cohort, except for three comparative studies – two with PPI27,28 and one with antireflux surgery. 8 A total of 691 patients with antireflux procedures (327 with ARMS, 161 with ARMA, and 203 with ARBL) were included in this review. The indication of antireflux procedures was PPI-refractory GERD in most studies except for Patil et al., 21 who enrolled PPI-dependent patients. These patients were typically nonobese (mean body mass index: 24.3–29.4), and most of them had hiatal hernia (357 of 494, 72.2%). All patients underwent endoscopy and a pH test at baseline; only two studies used AET > 6%20,24 as the threshold, whereas the others used >4.2%.14,15,28 All but one studies excluded patients with prior antireflux surgery, bariatric surgery, significant esophageal motility disorders, or large sliding hernia (>2 cm), yet Monino et al. 20 included three patients who underwent prior Nissen fundoplication or gastric bypass surgery.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
Baseline characteristics of patients among the included studies.

ARBL, antireflux band ligation; ARMA, antireflux mucosal ablation; ARMS, antireflux mucosectomy; EMRB, endoscopic mucosal resection with band ligation; EMRC, endoscopic mucosal resection with cap; ESD, endoscopic submucosal dissection; H-APC, hybrid argon plasma coagulation; IQR, interquartile range; NA, not available; NF, Nissen fundoplication; PPI, proton pump inhibitor; SD, standard deviation; TT knife, triangle tip knife.
Techniques of ARMI
For ARMS, most studies used either cap-assisted EMR,8,14,15,17,18,21 or band ligation-assisted EMR,8,19,20 and only a minority of patients underwent ESD.8,15,22 ARMA was performed using hybrid argon plasma coagulation 24 or an electrosurgical knife. 30 ARBL used bands in forward view, such as endoscopic variceal ligation with 28 or without clip fixation, 27 or in retrospective position with up to 10 bands. 29 The mean procedure time was shorter with ARBL (12.3 ± 3.2 min) 29 than with ARMS (35–54.7 min),8,14,15,19,20 and ARMA (29–35.6 min).24,25,30 Sumi et al. 15 reported a longer procedure time with ESD (129.7 ± 13.6 min) than with cap-assisted EMR with the ‘crescent’ (⩾ 270° of GEJ) resection (56.4 ± 24.5 min) or ‘butterfly’ (240° of GEJ) resection (38.5 ± 15.3 min).
Clinical outcomes of ARMI
Technical success and significant symptomatic improvement were claimed as 100% in all studies, regardless of the type of procedure. The pooled clinical success rate was 73.8% (95% CI = 69%–78%, Figure 2). Specifically, clinical success averaged 68.6% (95% CI = 62.2%–74.4%) among ARMS studies,14,15,19–21 86.7% (95% CI = 78.7%–91.9%) of the ARMA study at 6 months, 24 and 76.5% (95% CI = 65%–85.1%) of the ARBL study at 12 months. 29 Although only a few studies were available for this outcome, pooled analysis suggested that ARMA had a better clinical success rate than ARMS and ARBL (p < 0.001). Moreover, the improvement of symptom scores based on various clinical questionnaires lasted up to 12 months (Table 2). The pooled estimates suggested that 61.5% (95% CI = 54.6%–67.9%) could discontinue PPI and 87.8% (95% CI = 81.8%–92.0%) could reduce PPI at 6 months,8,14,15,19–22,24,28 whereas 55.9% could discontinue PPI and 68.1% (95% CI = 60.3%–74.9%) could reduce PPI at 12 months,15,21,24,27,29 (Supplementary Table 1). The pooled proportion of reflux esophagitis also reduced from 91.1% to 24.5% after the procedure.21,24,27,28

Pooled clinical success rate among studies with antireflux mucosal intervention (ARMI) procedures. Heterogeneity: I2 = 51.2%, τ2 = 0.107, p = 0.055.
Quality of life and symptom scores before and after antireflux mucosal surgery.

ARBL, antireflux band ligation; ARMA, antireflux mucosal ablation; ARMS, antireflux mucosectomy; CI, confidence interval; FSSG, frequency scale for the symptoms of GERD; GERD-HRQL, Gastroesophageal Reflux Disease–Health-Related Quality of Life; IQR, interquartile range; NA, not available; RDQ, Reflux Disease Questionnaire; RSI, reflux symptom index; Rx, endoscopic treatment.
Per-protocol analysis. Studies without available data are not included in the table.
Sumi et al. 15 and Hernández Mondragón et al. 24 reported the respective outcome for ARMS and ARMA up to 36 months. Both studies suggested sustained symptomatic improvement based on questionnaire evaluation; however, only 21 of 109 (19.2%) completed the follow-up in the ARMS study. However, 84 of 108 patients (77.7%) completed 36-month follow-up in the ARMA study; 78.6% of them stayed PPI free, and 95.2% did not develop erosive esophagitis.
Improvement of pH and reflux tests and hiatal hernia after ARMI
Significantly improved AET (Table 3) and DeMeester score (Supplementary Table 2) was found in nearly all studies with available data (six with ARMS, one with ARMA, and another with ARBL),14,15,17,18,21,24,25,28,30 up to 6 months. Moreover, two studies24,28 reported longer follow-up and demonstrated the improvement sustained up to 12 months with ARMA and ARBL and may be up to 36 months with ARMA. No study on ARMS reported the outcomes of pH testing beyond 6 months. In terms of reflux episodes, three18,27,28 out of four studies reported significant improvement, and the two studies with ARBL suggested a sustained response at 12 months. The remaining study by Sumi et al. 15 suggested a significant reduction of acid refluxes, but not nonacid and overall refluxes. Seleem et al. 27 was the only study to report a symptom index before and after the procedure, demonstrating a sustained improvement up to 12 months.
Acid exposure time before and after antireflux mucosal surgery.
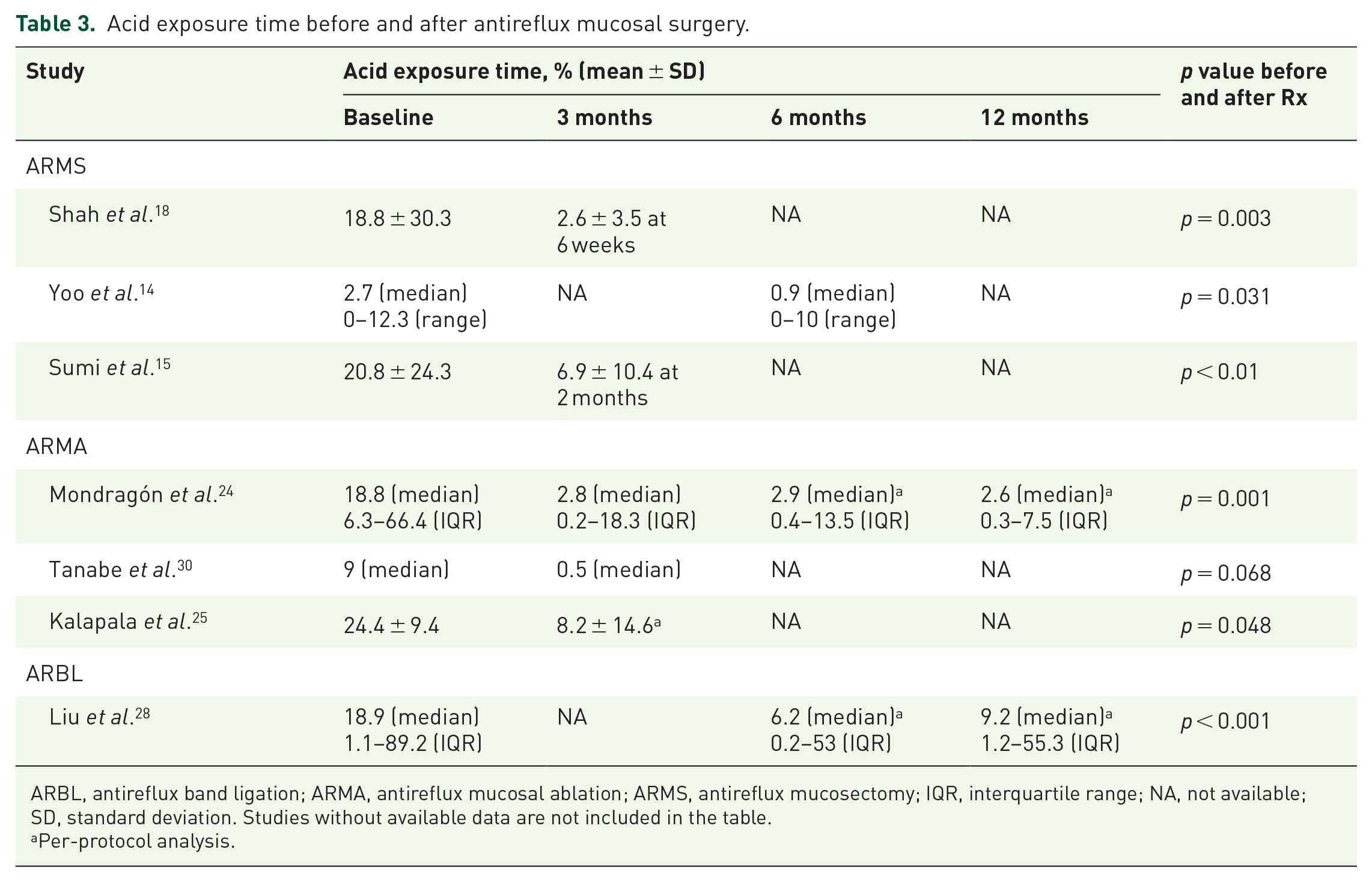
ARBL, antireflux band ligation; ARMA, antireflux mucosal ablation; ARMS, antireflux mucosectomy; IQR, interquartile range; NA, not available; SD, standard deviation. Studies without available data are not included in the table.
Per-protocol analysis.
Hiatal hernia was prevalent in the study population, ranging from 28% to 100% among the included studies. The extent of hiatal hernia and GEJ competency improved after ARMI in several studies regardless of the type of procedure (Supplementary Table 3),8,14,17,20,21,27–29 Yoo et al. 14 used EndoFLIP to demonstrate that GEJ distensibility significantly decreased at 6 months after ARMS (median distensibility index from 19 to 13, p < 0.001), indicating tightening of GEJ. Furthermore, resting LES pressure also became higher in two studies with ARMS and ARBL, respectively.14,28
Adverse events of ARMI
The adverse events were mainly bleeding (immediate or delayed), perforation, or dysphagia (Table 4). Notably, no study of ARBL reported such complications, whereas delayed bleeding (pooled incidence 1.6%) and perforation (pooled incidence 2.4%) were reported with ARMS.8,15,17,19–21 However, all cases, except one with perforation, could be managed endoscopically. Although Patil et al. 21 reported a 100% immediate bleeding rate in the cohort, all other studies reported a much lower occurrence, and only 0–3.7% required intraoperative hemostasis.
Adverse events of antireflux mucosal surgery.
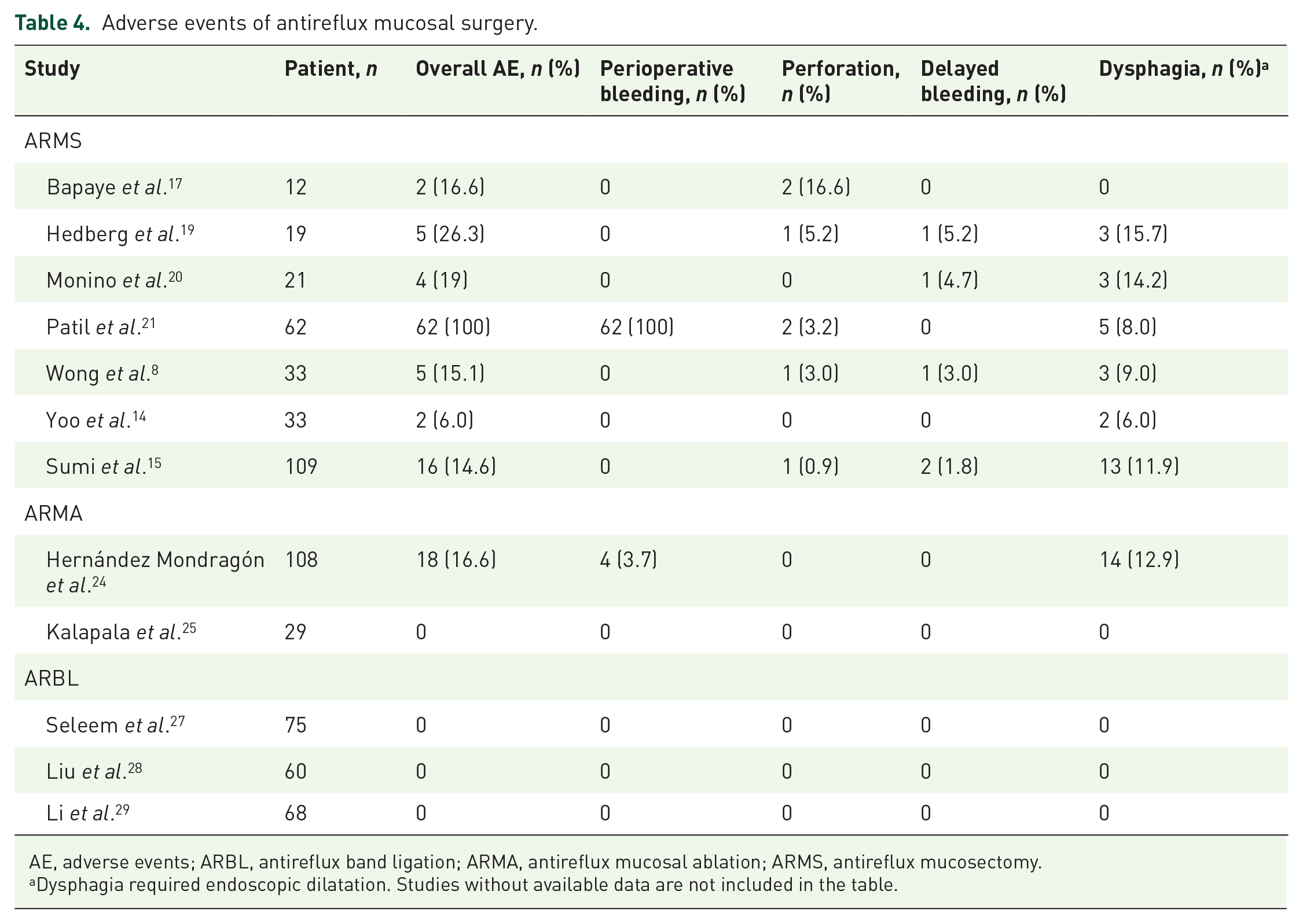
AE, adverse events; ARBL, antireflux band ligation; ARMA, antireflux mucosal ablation; ARMS, antireflux mucosectomy.
Dysphagia required endoscopic dilatation. Studies without available data are not included in the table.
Dysphagia was a relatively common complication in ARMS (pooled incidence 10.6%, 95% CI = 7.5%–14.8%, Supplementary Figure 1) and ARMA (pooled incidence 8.3%, 95% CI = 1.6%–32.9%). Remarkably, no case of dysphagia requiring endoscopic dilatation occurred with ARBL (p < 0.001 compared with other techniques). In studies with available data,8,15,19–21,24 39% of dysphagia cases were resolved after a single session of endoscopic dilatation, but another 39% of cases required ⩾3 sessions. Two studies8,15 found that the ‘butterfly’ modification of ARMS with sparing a space of both lesser and greater curvature may result in a lower rate of dysphagia (pooled incidence: 2.7% with butterfly and 14.9% with crescent resection).
Overall, 10.5% of patients underwent salvage antireflux procedures after ARMI.8,14,15,19–21,24,27,28 Most (63.6%) of the salvage procedures were repetitive endoscopic procedures, and the remaining procedures were antireflux surgery, including fundoplication and magnetic sphincter augmentation (Supplementary Table 4). Risk factors for treatment failure were reported in two studies: Sumi et al. 15 suggested older age (49.4 ± 15.8 of responders versus 60.2 ± 15.9 of nonresponders, 60.2 ± 15.9, p = 0.004), and Hernández Mondragón et al. 24 indicated that baseline severe hiatal hernia (Hill type III), normalization of hiatal hernia at 3 months, and AET < 4 at 3 months were significant risk factors.
Risk-of-bias assessment of the included studies
Most included retrospective studies had high risk bias due to the lack of a control group, and only two studies were considered high quality in this review8,28 (Supplementary Table 5). In addition, three studies17–19 enrolled <20 cases, and five studies17,18,22,25,30 had only abstracts, although two of them were follow-up reports of published studies.23,26 The only randomized control trial 27 was considered a high risk of bias owing to a lack of blinding to both participants and outcome assessment, along with the absence of detailed randomization and allocation concealment.
Discussion
In this systematic review, we found that ARMI procedures are effective and safe for both PPI-refractory and PPI-dependent patients. The clinical success rate exceeded 70% at 6 months, and more than half of patients could discontinue PPIs. Several studies have suggested that symptomatic improvement may last up to 12–36 months.8,15,24,27–30 Therefore, the clinical efficacy of ARMI procedures seems similar to that of radiofrequency ablation and endoscopic fundoplication, such as transoral incisionless fundoplication.31,32 However, unlike radiofrequency ablation, ARMI procedures can restore LES pressure and significantly improve hiatal hernia. 32 Compared with endoscopic fundoplication, the devices of ARMI procedures are generally simpler, thus potentially reducing cost and increasing accessibility, making ARMI a promising antireflux endoscopic treatment.
The occurrence of severe adverse events, including perforation and bleeding rates of ARMI, is also similar to that of transoral incisionless fundoplication in a previous meta-analysis (2.4%). 31 However, up to 10% of patients developed dysphagia after ARMI procedures, although it could be managed with just a few sessions of endoscopic dilatation. Notably, perforation was reported only with ARMS, possibly due to the intrinsic risk associated with endoscopic resection. By contrast, the complication rate with ARBL was impressively low. The safety profile may be an essential consideration when choosing among ARMI procedures.
In addition to symptomatic improvement, ARMI procedures led to significantly reductions in AET, DeMeester score, and amount of reflux esophagitis. These encouraging results are likely due to GEJ competency following ARMI-induced ulcer formation and subsequent fibrosis. However, increasing the extent and depth of intervention does not necessarily mean better outcomes, and the optimal technique also remains unclear. For instance, the modified ‘butterfly’ approach of ARMS with a lesser extent of resection appears to reduce postprocedural dysphagia with preserved efficacy.8,15 A study published after our review process suggests that 180° ARMS may have lower dysphagia than 270° ARMS, with similar efficacy. 33 Although ARMS techniques continue to evolve, it is slightly more invasive than ARMA and ARBL without significantly better outcomes. However, the large series by Hernández Mondragón et al. 24 demonstrated impressive outcomes of ARMA with hybrid argon plasma coagulation, and ARBL studies have also indicated it excellent safety profile without a high technical demand. Consequently, ARMA and ARBL might be preferable based on the current data. Nevertheless, randomized trials are warranted to compare the three types of procedures and determine the optimal technique.
Endoscopic treatment is a less invasive alternative to the more definite antireflux surgery. 34 The case-control study by Wong et al., 8 included in this systematic review, compared ARMS and Nissen fundoplication and concluded that ARMS has similar efficacy to Nissen fundoplication for up to 24 months but with more favorable perioperative outcomes and safety profiles. Although more comparative studies are warranted to validate the conclusion, our review indicated that ARMI procedures do not limit future antireflux surgeries, making them an attractive option for patients refractory to or dependent on PPI. However, most studies in the review did not include patients with prominent sliding hernias, which is considered a strong indication of antireflux surgery. Yoo et al. 14 suggested that patients with reflux hypersensitivity might benefit from ARMS. Thus, in future studies, the best candidates for the procedures should be identified by using pH/impedance and motility exams.
A strength of this systematic review is the thorough inclusion of up-to-date articles, with critical appraisal and analysis. Although another recent meta-analysis compared ARMS and ARMA, 35 we excluded studies with small sample sizes to reduce bias, and we also explored factors such as postoperative GEJ competency and risk factors for treatment failure in detail. Furthermore, the current analysis was comprehensive as we also included ARBL due to its similarity to ARMS in concept and technique, except that no resection is performed.
This study has several limitations. First, most of the included articles were retrospective and lacked control groups. Second, the outcome parameters were not complete in all studies because we only included the up-to-date report for each specific cohort, and a few lost-to-follow-up cases were not accounted for. Third, apparent clinical heterogeneity and marked variations in patient numbers and outcome parameters precluded performing meta-analyses for most outcomes. However, we analyzed the clinical success rate, PPI usage, and dysphagia rate to better demonstrate the efficacy and safety of ARMI procedures. Moreover, though nearly all studies claimed symptomatic improvement by questionnaire-based evaluation, we used the clinical success rate which was clearly defined (patients had ⩾50% symptomatic improvement compared with baseline) as the primary outcome, in order to have more validated assessment. Fourth, most of the studies analyzed included only PPI-refractory patients; only one involved PPI-dependent patients. Thus, the interpretation of outcomes for PPI-dependent patients should be done with caution. Finally, no included study investigated the feasibility of the procedures in patients who underwent sleeve gastrectomy, and only a few cases with prior antireflux surgery were included. 20 Nearly one-third of such patients developed GERD after surgery, and the response to radiofrequency ablation was unsatisfactory, possibly due to altered anatomy. 36 However, ARMI procedures may still provide improvement in symptomatic relief by tightening GEJ. 37 With more emerging studies and randomized controlled trials, more validated evidence and approaches for ARMI are required as part of GERD treatment.
In conclusion, the present systematic review indicates that ARMI procedures are efficacious and safe in PPI-refractory or PPI-dependent patients with GERD. The three procedures have similar efficacy, with ARMA and ARBL likely having fewer adverse events than ARMS. Further research is necessary to determine the optimal technique and candidates of the ARMI procedures.
Supplemental Material
sj-docx-1-tag-10.1177_17562848221094959 – Supplemental material for Antireflux mucosal intervention (ARMI) procedures for refractory gastroesophageal reflux disease: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848221094959 for Antireflux mucosal intervention (ARMI) procedures for refractory gastroesophageal reflux disease: a systematic review and meta-analysis by Jen-Hao Yeh, Ching-Tai Lee, Min-Hung Hsu, Chi-Wen Lin, Po-Jen Hsiao, Chien-Lin Chen and Wen-Lun Wang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-2-tag-10.1177_17562848221094959 – Supplemental material for Antireflux mucosal intervention (ARMI) procedures for refractory gastroesophageal reflux disease: a systematic review and meta-analysis
Supplemental material, sj-tif-2-tag-10.1177_17562848221094959 for Antireflux mucosal intervention (ARMI) procedures for refractory gastroesophageal reflux disease: a systematic review and meta-analysis by Jen-Hao Yeh, Ching-Tai Lee, Min-Hung Hsu, Chi-Wen Lin, Po-Jen Hsiao, Chien-Lin Chen and Wen-Lun Wang in Therapeutic Advances in Gastroenterology
Footnotes
Appendix
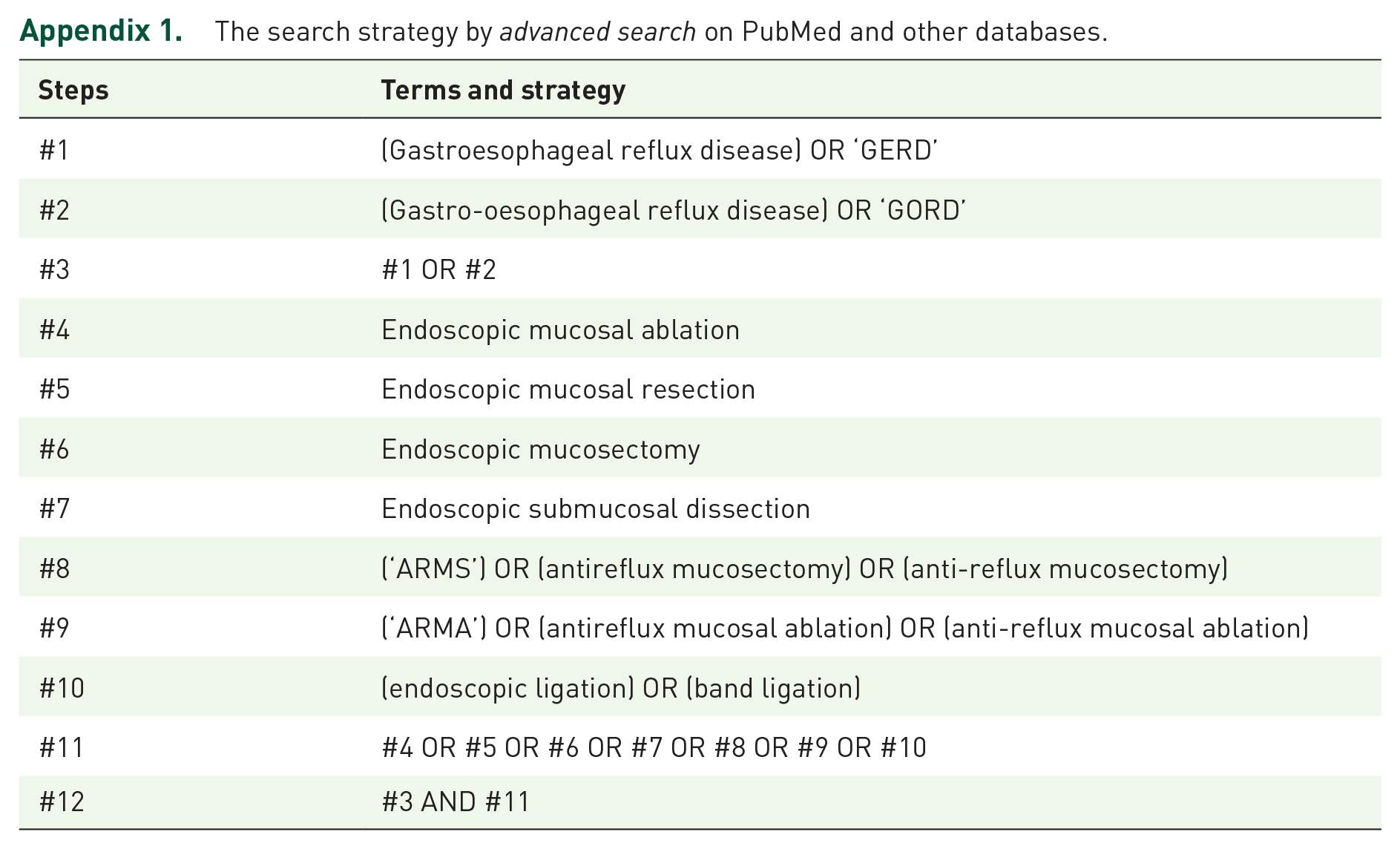
Appendix 1. The search strategy by advanced search on PubMed and other databases.
| Steps | Terms and strategy |
|---|---|
| #1 | (Gastroesophageal reflux disease) OR ‘GERD’ |
| #2 | (Gastro-oesophageal reflux disease) OR ‘GORD’ |
| #3 | #1 OR #2 |
| #4 | Endoscopic mucosal ablation |
| #5 | Endoscopic mucosal resection |
| #6 | Endoscopic mucosectomy |
| #7 | Endoscopic submucosal dissection |
| #8 | (‘ARMS’) OR (antireflux mucosectomy) OR (anti-reflux mucosectomy) |
| #9 | (‘ARMA’) OR (antireflux mucosal ablation) OR (anti-reflux mucosal ablation) |
| #10 | (endoscopic ligation) OR (band ligation) |
| #11 | #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 |
| #12 | #3 AND #11 |
Acknowledgements
We appreciate the inspiration and support of all members of the Taiwan Esophageal Consortium. This manuscript was edited by Wallace Academic Editing.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the EDAHP111012 project of E-Da Hospital granted to Dr Jen-Hao Yeh. The funder had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All data are extracted from the original reference articles.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.