
Abstract
Background:
Pancreatic cancer (PC) is a highly fatal malignancy with a global overall 5-year survival of under 10%. Screening of PC is not recommended outside of clinical trials. Endoscopic ultrasonography (EUS) is a very sensitive test to identify PC but lacks specificity and is operator-dependent, especially in the presence of chronic pancreatitis (CP). Artificial Intelligence (AI) is a growing field with a wide range of applications to augment the currently available modalities. This study was undertaken to study the effectiveness of AI with EUS in the diagnosis of PC.
Methods:
Studies from MEDLINE and EMBASE databases reporting the AI performance applied to EUS imaging for recognizing PC. Data were analyzed using descriptive statistics. The Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool was used to assess the quality of the included studies.
Results:
A total of 11 articles reported the role of EUS in the diagnosis of PC. The overall accuracy, sensitivity, and specificity of AI in recognizing PC were 80–97.5%, 83–100%, and 50–99%, respectively, with corresponding positive predictive value (PPV) and negative predictive value (NPV) of 75–99% and 57–100%, respectively. Types of AI studied were artificial neural networks (ANNs), convolutional neural networks (CNN), and support vector machine (SVM). Seven studies using other than basic ANN reported a sensitivity and specificity of 88–96% and 83–94% to differentiate PC from CP. Two studies using SVM reported a 94–96% sensitivity, 93%–99% specificity, and 94–98% accuracy to diagnose PC from CP. The reported sensitivity and specificity of detection of malignant from benign Intraductal Papillary Mucinous Neoplasms (IPMNs) was 96% and 92%, respectively.
Conclusion:
AI reported a high sensitivity with high specificity and accuracy to diagnose PC, differentiate PC from CP, and differentiate benign from malignant IPMN when used with EUS.
Keywords
Introduction
Pancreatic cancer (PC) is one of the most fatal cancers globally, with a 5-year overall survival rate of 9% for all stages and only 3% for Stage IV disease. There has been an over 50% increase in incidence and mortality over the last 25 years, and the burden may double in the next four decades. 1 It is the third leading cause of cancer mortality in the United States, with more than 45,000 deaths annually and is expected to become the second leading cause of cancer death. Despite these trends, there is insufficient evidence for current practice guidelines to recommend PC screening in asymptomatic individuals. However, certain high-risk groups, for example, patients with germline mutations in BRCA1, BRCA2, TP53, and Lynch syndrome with mismatch repair genes, may benefit from screening if highly sensitive and specific non-invasive tests were available. 2
Multiple modalities, such as CT scans, magnetic resonance imaging (MRI), and endoscopic ultrasound (EUS), are currently being used to diagnose PC. Among these, EUS is considered superior due to its ability to obtain high-quality images. 3 However, it has low sensitivity in differentiating benign from malignant Intraductal Papillary Mucinous Neoplasms (IPMNs). 3 In the presence of chronic pancreatitis (CP), EUS and endoscopic sonoelastography have a high sensitivity but a low specificity making the differentiation challenging, and cytologic diagnosis remains the gold standard. 4 Furthermore, EUS is operator-dependent, and less experienced endoscopists could miss the subtle difference between CP and PC because of the presence of concomitant scarring and calcification due to chronic inflammation. 5
Artificial Intelligence (AI) is a term applied to any computer system that has been developed to learn and emulate the biological brain. Machine learning (ML) is a form of AI that uses large amounts of data to find various patterns from it (Table 1). There are three types of ML – supervised learning, unsupervised learning, and reinforced learning. Supervised learning has been studied and applied to medicine, especially in diagnostics. Two types of supervised learning methods have been explored in EUS, which are artificial neural networks (ANNs), also called neural networks (NN), and support vector machine (SVM).6,7 Deep Learning (DL) is an advanced concept that stems from ANN and uses multiple complex layers of ANN, inspired by the neurons of the human brain. Convolutional neural networks (CNNs) are an example of a DL program that is based on visual signal processing by humans. 7 SVM is a type of supervised ML method where large amounts of data are inputted to generate two or more categories divided by boundaries. Although simpler and more generalizable than ANN, SVM takes longer to develop and requires a very large amount of data for ML.6,8
Various types of AI terminologies and their explanation.

During the past decade, significant advances have been made on the application of AI in the diagnosis and management of gastrointestinal diseases. Some of them include application of AI for increased accuracy and predicting survival in esophageal cancer, improved prognostic prediction in inflammatory bowel disease (IBD), prediction of nodal metastasis in early-stage colorectal cancer, and prognostic evaluation of PCs.9,10 Hence in this article, we performed a systemic review of the current published literature to assess the application of AI programs for EUS-mediated recognition of primary pancreatic malignancies, including differentiation between PC and CP.
Methods
Study selection
We searched MEDLINE and EMBASE databases (inception to 10 April 2021) using keywords and/or Medical Subject Headings (MeSH) for ‘pancreatic cancer’, ‘artificial intelligence’, ‘computer-aided’, ‘neural networks’, ‘deep learning’, ‘machine learning’, ‘computer-assisted diagnosis’ and ‘support vector machine’. The detailed search strategy is listed in the Supplementary file. Two authors (S.G. and H.G.) independently reviewed the references and selected studies for full-text screening. An additional search was done by reference screening of the selected articles. Studies were deemed fit for inclusion if they reported the performance of any form of AI applied to EUS imaging for recognizing PC. Studies were excluded if they used AI to gauge human performance only or did not report diagnostic sensitivity and specificity of AI in recognition of pancreatic malignancies. Diagnostic odds ratio (DOR) was calculated from the available data.
Data extraction and quality assessment
We extracted data regarding study design, patient population, type of AI used, reported outcomes, and limitations (Table 2). Data were extracted by one author (S.A.A.S.) and reviewed by a second author (S.G.). The Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool was used to assess the quality/risk of bias of studies included in this review. 11
Study characteristics.

AIP, autoimmune pancreatitis; ANN, artificial neural network; CAD, computer-aided diagnosis; CNN, convolutional neural network; DL, deep learning; EUS, endoscopic ultrasound; FNA, fine needle aspiration; IPMN, intraductal papillary mucinous neoplasm; MLP, multilayer perceptron; NP, normal pancreas; NN, neural network; NPV, negative predictive value; PC, pancreatic cancer; PDAC, pancreatic ductal adenocarcinoma; PNET, pancreatic neuroendocrine tumor; PPV, positive predictive value; Sn, sensitivity; Sp, specificity; SVM, support vector machine.
Results
A total of 1669 studies were identified from the initial search of all databases and reference screening, of which 24 were selected for full-text review (after removing duplicates) and 11 were included in the final analysis (Figure 1). There were a total of 2292 patients across all studies consisting of 1409 pancreatic malignancies with 1383 patients with PC, 3 with pancreatic neuroendocrine tumors (PNET), and 27 with malignant IPMN.12–22 Study characteristics are listed in detail in Table 2.
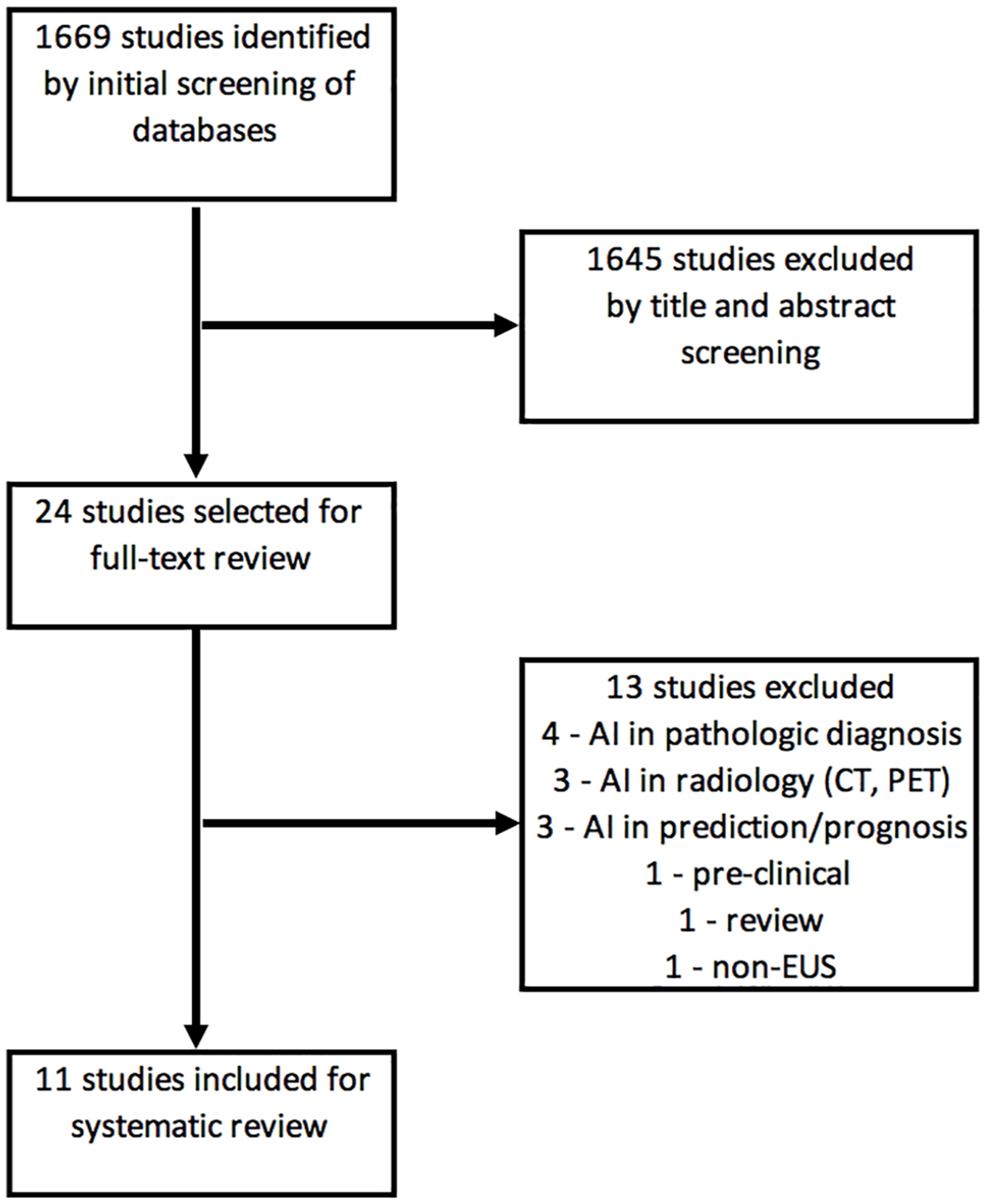
PRISMA flowchart.
Study design
Eight studies12–16,20–22 were retrospective in nature using images (still or video) from already performed EUS procedures. Three studies17–19 were conducted to collect images in real time to be fed into an AI system. Overall, 10 studies12,14–22 assessed the performance of AI to recognize PC, while one 13 studied the recognition of malignant IPMNs. All patients in all studies had a confirmed cytologic diagnosis of the condition studied, including CP and malignancy. Most studies lacked detailed data to create a 2 × 2 contingency table; hence a formal meta-analysis could not be performed.
EUS images used
Seven studies12,13,15,16,20–22 used still EUS images, of which two studies used data augmentation to increase the number of images several folds to be fed in the AI system. Three studies17–19 used video images, and one 14 used both still and video images.
Type of AI studied
SVM was used in two studies21,22 while nine studies used NNs12–20 – one used basic NN, 15 five used ANN12,16–19 [with two using multilayer perceptron (MLP)]12,18 while three studies used CNN.13,14,20
Overall performance of AI in pancreatic malignancy recognition
Among the 11 studies,12–22 the overall reported sensitivity of AI in recognizing malignancy of the pancreas ranged 83–100%, while specificity ranged 50–99% and accuracy 80–97.5%. The reported positive predictive value (PPV) and negative predictive value (NPV) ranged 75–99% and 57–100%, respectively. The DOR could be calculated for 10 studies, and it ranged 34–3003 (Table 3).
Performance of AI in diagnosis of pancreatic malignancies.

AI, Artificial Intelligence; ANN, artificial neural network; CNN, convolutional neural network; DOR, diagnostic odds ratio; NPV, negative predictive value; PPV, positive predictive value; SVM, support vector machine.
AI to differentiate PC from CP
Seven studies12,14,15,17–19,22 reported the diagnostic value of AI in differentiating PC from CP with a sensitivity and specificity ranging 88–100% and 50–94%, respectively. Excluding the study by Norton et al. 15 that used basic ANN, the sensitivity and specificity ranged 88–96% and 83–94%, respectively. One study 22 that used SVM to differentiate PC from CP reported the highest sensitivity of 96%, with 93% specificity and 94% accuracy. This study used a simple SVM classifier.
One study trained a CNN model with images from patients with PC, CP, and normal pancreas to identify PC with 90% sensitivity, 75% specificity with an AUC of 0.92. 20
AI to differentiate malignant from benign IPMNs
One study 13 reported using AI to differentiate benign from malignant IPMNs. It included 50 patients with IPMN with 23 malignant and 27 benign cases consisting of 3970 still images. Data augmentation was used to generate 508,160 images that were analyzed using the CNN system. The system reported 94% accuracy, 95.7% sensitivity, and 92.6% specificity to identify malignant IPMNs.
SVM and PC recognition
Two studies21,22 used SVM and reported accuracy, sensitivity, and specificity ranging 94–98%, 94–96%, and 93–99%, respectively, to recognize PC, with the highest DOR of all studies. The corresponding PPV and NPV ranged 92–99% and 97–98%, respectively. Both these studies were retrospective and used still images in the AI model.
CNN and PC recognition
Of the three studies13,14,20 that used CNN, two14,20 studied the diagnostic value of AI to recognize PC, while one 13 studied the differentiation of benign versus malignant IPMNs. The two studies14,20 evaluating PC recognition reported sensitivity, specificity, PPV, and NPV ranging 92–95%, 84–91%, 87%, and 91–97%, respectively. The third study 13 reported sensitivity, specificity, PPV, and NPV of 96%, 93%, 92%, and 96%, respectively. All three studies used still images from the EUS, while one 14 also included video images. Two13,20 of the three studies had small sample sizes of 50 and 139 patients and used data augmentation to generate a large dataset of images from the original images to create the AI algorithm.
ANN and PC recognition
Six studies12,15–19 using ANN (without DL) reported sensitivity, specificity, PPV, and NPV ranging 83–100%, 50–94%, 75–97%, and 57–100%, respectively. Three studies12,15,16 used still images to be fed in the AI system, while three others17–19 used video images for analysis. One study 16 divided patients by age and showed a higher sensitivity (93.3%) of AI in detecting PC in patients above 60 years of age compared to patients below 60 years of age where the sensitivity fell to 85.7% (age 40–60 years) and 87.5% in patients below 40 years of age.
Quality of included studies
The overall quality of studies was graded using the QUADAS-2 tool 11 (Figure 2). Four studies collected the index and standard test at the same time, while others were retrospective review of images. Although there is a low risk of bias for the performance of the reference test, there was a high risk of bias in several studies for the index test being performed unblinded. Being retrospective in design, several studies suggested high risk of patient selection bias. Overall, the quality of evidence was low to moderate, mostly due to a high or unclear risk of bias in patient selection.

QUADAS-2 analysis of study quality/risk of bias.
Discussion
EUS is a superior diagnostic modality than CT or MRI in the diagnosis of PC with high sensitivity (95%) but a rather low specificity (53%), especially in the presence of CP. 4 The cytologic diagnosis remains the mainstay of differentiating CP from PC. 23 Our systematic review suggests that AI may be used as a unique tool to augment the performance of EUS and improve its diagnostic ability for recognizing pancreatic malignancies even in the presence of CP, with improved sensitivity and specificity. Furthermore, the AI can be trained with still or video images or a combination of both. However, the performance of AI can vary depending on the type of the AI model used.
Different AI systems vary in complexity (Table 1). For instance, SVM is a type of supervised ML method where the data fed in the system are classified into two or more categories separated by a linear line for two categories and plans for more than two categories. The calculation for two categories separated by a linear line requires a fairly simple calculation. In addition, the dividing line may be soft to allow accommodation of anomalous readings. Although it is fairly simpler than NNs and more generalizable, SVM requires a large amount of data for ML.6,8
ANN is a form of AI where the system tries to mimic neural circuits in the human brain. The data pass through multiple layers connected by nodes, and each connection is given a certain weight, indicating the strength of the connection that the system can adjust as it learns. The system can also adjust for bias and provides output by making necessary corrections through forward- and back-propagation of the data through the layers.6,7
CNN is the most sophisticated AI system since it is designed to emulate the visual signals processed by the biological brain. It is more independent in its learning compared to SVM, which is supervised ML. Simplistically, the system extracts distinct features from the data, creates classifications, and applies specific filters to create multiple feature maps. Each image is subject to filtering giving it the name convolutional. A final layer combines the all-filter layers in a fully connected layer giving the final result.6,7
In our systematic review, the SVM methodology revealed the highest sensitivity, specificity, and diagnostic accuracy to distinguish PC from CP and normal pancreas with 94–98% accuracy, 94–96% sensitivity, and 93–99% specificity, respectively.21,22 CNN was also effective in making that determination, but the specificity ranged 84–87%.14,20 However, in the differentiation of benign versus malignant IPMNs, CNN performs better (with accuracy, sensitivity, and specificity of 94%, 95.7%, and 92.6%, respectively). 13 These numbers are higher compared to EUS alone per historic data. 23 ANN was more variable in performance, but when the study applying basic ANN was excluded, the specificity increased to 83–93%, again better than conventional EUS alone.
Few limitations exist for our systematic review. Most of the published literature included a small number of patients with a retrospective, non-randomized design. It remains to be seen if the performance of AI-assisted EUS in real time can match or exceed these numbers. Another drawback is that most images selected were recorded and reviewed by extremely experienced endoscopists before being fed in the AI system; hence, the generalized applicability of AI to endoscopists with all levels of experience also remains to be seen. In addition, studies were heterogenous in the types and methodologies of AI studied. Nevertheless, AI performed better than conventional EUS overall in differentiating PC from CP and non-cancer patients. SVM method turned out to be a simpler system than CNN and with its high performance seems promising in recognizing cancer in the presence of chronic pancreatic inflammation or screening for PC especially in high-risk individuals. However, further studies are needed, especially prospective and real time, to establish the role of AI in routine EUS procedures for endoscopists of all training levels.
If AI development continues at the current pace, it may be possible to use AI in the future to accurately differentiate PC from CP and other non-cancer conditions with EUS imaging alone without the need for pathological diagnosis. This would be especially helpful in PC screening in high-risk patients with germline mutations and genetic syndromes that places them at high risk of PC but currently have no consensus on effective screening.
Conclusion
AI technology is a promising adjunct to conventional EUS for recognizing PC, especially in the presence of CP. Of all the AI modalities under development, SVM reported the highest sensitivities, specificities, and DOR for recognition of PC. Being a simpler system than ANN and CNN, the SVM system seems worthy of further exploration in prospective studies, possibly as a quick screening tool, especially in high-risk individuals. However, further studies are needed for its refinement and for use in daily practice.
Supplemental Material
sj-docx-1-tag-10.1177_17562848221093873 – Supplemental material for Application of artificial intelligence in diagnosis of pancreatic malignancies by endoscopic ultrasound: a systemic review
Supplemental material, sj-docx-1-tag-10.1177_17562848221093873 for Application of artificial intelligence in diagnosis of pancreatic malignancies by endoscopic ultrasound: a systemic review by Hemant Goyal, Syed Ali Amir Sherazi, Shweta Gupta, Abhilash Perisetti, Ikechukwu Achebe, Aman Ali, Benjamin Tharian, Nirav Thosani and Neil R. Sharma in Therapeutic Advances in Gastroenterology
Footnotes
Authors statement
The article has been read and approved by all the authors that the requirements for authorship as stated earlier in this document have been met and that each author believes that the article represents honest work.
Ethical statement
As submitted or its essence in another version, this article is not under consideration for publication elsewhere. It will not be published elsewhere while under review by Therapeutic Advances in Gastroenterology. All authors have made substantive contributions to the study, and all authors endorse the data and conclusions.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hemant Goyal – Consultant for Aimloxy LLC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.