
Abstract
Clostridioides difficile infection is a leading cause of healthcare-associated infections with significant morbidity and mortality. For the past decade, the bulk of infection prevention and epidemiologic surveillance efforts have been directed toward mitigating hospital-acquired C. difficile. However, the incidence of community-associated infection is on the rise. Patients with community-associated C. difficile tend to be younger and have lower mortality rate. Rates of recurrent C. difficile infection overall have decreased in the United States, but future research and public health endeavors are needed to standardize and improve disease detection, stratify risk factors in large-scale population studies, and to identify regional and local variations in strain types, reservoirs and transmission routes to help characterize and combat the changing epidemiology of C. difficile.
Keywords
Introduction
Clostridioides difficile infection (CDI) is a leading cause of healthcare-associated infections with significant morbidity and mortality. CDI is associated with 15,000–30,000 deaths annually in the United States and acute inpatient costs exceeding $4.8 billion. 1 C. difficile is a spore-forming, anaerobic, gram-positive rod which causes disease through release of enterotoxin A and cytotoxin B. Certain strains, most notably NAP1/027, produce a markedly increased level of these toxins, which may contribute to its hypervirulence and association with severe disease manifestations. 2
In recent years, tremendous efforts have been directed at curbing healthcare-associated CDI worldwide. The Centers for Disease Control (CDC) in the United States launched its C. difficile surveillance program in 2009 and highlighted six key components of prevention in its 2012 Vital Signs report. 3 Globally, 28 countries/territories in four World Health Organization regions have also established guidelines for infection control, detection and surveillance. 4 As a result, there is promising evidence that CDI rates have declined in Europe since 2010 and the United States since 2015.1,5 However, CDI is increasingly detected in individuals with no prior hospitalizations or healthcare exposures, suggesting a rise in community-acquired CDI. 6 In addition, as many as 35% of patients will experience recurrent CDI (rCDI), with an increased risk of recurrence following each subsequent episode. This significantly impacts not only individual patients but also the healthcare system, as rCDI is associated with increased medical costs compared with primary episodes. Our objective is to review the burden and characteristics of community-acquired and rCDI, and to delineate the challenges posed by the changing epidemiology.
Community-acquired CDI
Rising incidence over the past decade
According to recent guidelines from the Society for Healthcare Epidemiology of America released in 2018, CDI cases are categorized as community associated (CA-CDI) if patients experienced diarrhea onset in the community or within 48 h after hospitalization and had not been discharged from a healthcare facility in the prior 12 weeks. 1 The population-based CA-CDI incidence was reported to be 20–40 per 100,000 people between 2005 and 2006, before more sensitive nucleic acid amplification tests for C. difficile diagnosis became available. 7 Overall, the incidence of CA-CDI has risen over the past decade. In the most recent survey from the CDC Prevention Emerging Infections Program, the estimated incidence of CA-CDI in the United States increased from 52.88 per 100,000 people in 2012 to 65.93 per 100,000 people in 2017. 8 Interestingly, while the absolute number of CA-CDI cases has increased from an estimated 170,000 in 2011 to 226,400 cases in 2017, there has been a slow downtrend in the total number total CDI cases nationally, from 476,400 in 2011 to 462,100 in 2017 (Figure 1). 6
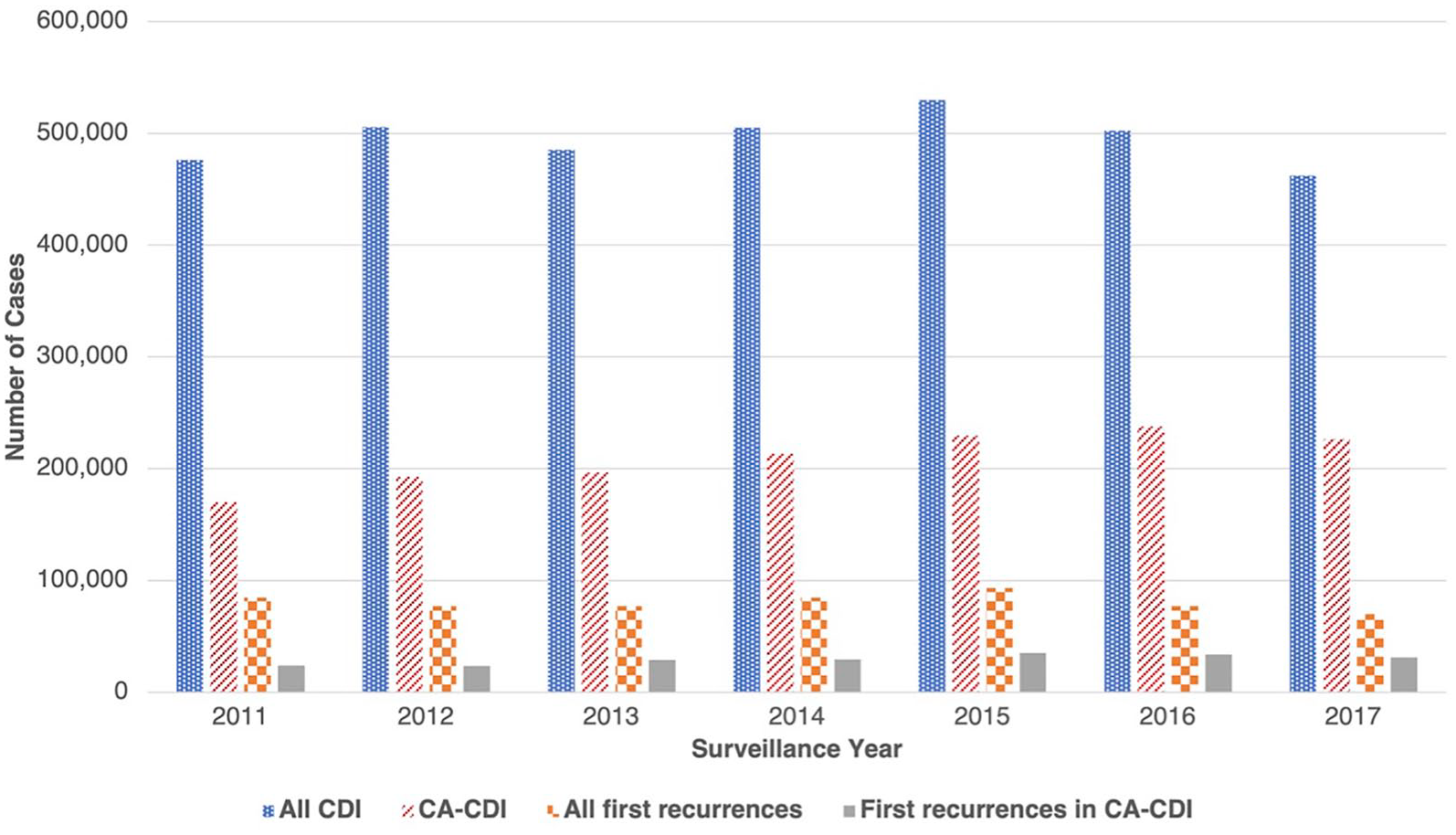
Estimated national burden of total Clostridium difficile infection (CDI), community-associated CDI, and recurrent CDI, 2011–2017, adapted from Guh et al. 6
The uptick of CA-CDI is consistent with previous studies in different regions in North America (Table 1).7,9 In a retrospective multicenter cohort study from 43 hospitals in Georgia, Florida, North Carolina, South Carolina, Virginia, and West Virginia, CA-CDI increased from 48.5% to 61.0% of all CDI cases.10,11 CA-CDI has also led to increasing hospitalizations in the United States, from 17.1 per 100,000 persons in 2011 to 21.7 per 100,000 persons in 2017. In contrast, healthcare-associated CDI (HA-CDI) hospitalizations have been declining (60.7 per 100,000 persons to 47.9 per 100,000 persons in 2017). 6 In Canada, CA-CDI has also increased in Quebec (from 0.51 to 0.69 per 100,000 population between 2008 and 2015) and Ontario (from 6.09 to 9.56 cases per 100,000 person-years between 2005 and 2015) during the overlapping time period while total CDI cases in the nation decreased.12–14
Comparison of total C. difficile infection (CDI) versus community-associated CDI (CA-CDI) in United States and Canada.

Global CA-CDI trends vary considerably when compared with the United States and Canada. During 2006 and 2017, the reported proportion of CA-CDI varied between 10.9% and 43.0% of all CDI cases in Japan, Italy, and Australia.5,12,15–17 The global discrepancy likely lies in surveillance methods. Cases of CA-CDI tend to be lower using hospital-based surveillance while reaching nearly 50% with population-based surveillance, given that nearly 75% of patients with CA-CDI are treated as outpatients.7,17 The worldwide burden of CDI in the community warrants further investigation.
Risk factors and mortality for CA-CDI
Patients diagnosed with CA-CDI tend to be younger with a significant proportion of patients (36%) reporting no antibiotic exposure during the 12 weeks prior to diagnosis (Table 2).1,9 In a population study by Khanna et al., 11 patients with CA-CDI were younger (median age of 50 versus 72 years) compared with patients diagnosed with hospital-acquired CDI (HA-CDI). In a 2015 surveillance study of national CDI burden in the United States conducted by the CDC, there was a larger proportion of younger patients (age <65 years) with CA-CDI than HA-CDI (56.2% versus 30.5%). 9 Patients with CA-CDI tend to have lower estimated mortality rates compared with HA-CDI, ranging from 0.09% in 2011 to 0.07% in 2017.6,18 In a single-center retrospective study in France, CA-CDI was weakly associated (p = 0.047) with more severe disease based on a composite score compared with hospital-associated infections; however, there was no difference in mortality. 19 More prospective studies are needed to elucidate if the outcomes of patients with CA-CDI differ significantly from their counterparts with HA-CDI.
A comparison of risk factors and other characteristics in healthcare-associated C. difficile infection (CDI) versus community-acquired CDI versus recurrent CDI.

Antibiotic use has long been associated with increased risks of CDI [odds ratio (OR) 3.55, 2.56–4.94]. 22 As mentioned earlier, a larger portion of patients had no prior exposure to antibiotics in CA-CDI compared with HA-CDI. In a meta-analysis in the United States and a retrospective study in Britain, the proportions of CA-CDI patients without antibiotic exposure are approximately 21%–38%, compared with 6%–20.3% in HA-CDI.11,17,23 In terms of the classes of antibiotics, Brown et al. 22 found that clindamycin [OR = 16.80, 95% confidence interval (CI) 7.48–37.76], fluoroquinolones (OR = 5.50, CI 4.26–7.11) and carbapenems (OR = 5.68, CI 2.12–15.23) are the most likely to be associated with CDI, while macrolides (2.65, CI 1.92–3.64) and penicillins (OR = 2.71, CI 1.75–4.21) are still problematic but less so. 22
Among the medications that are suspected culprits for increasing risk for CDI, proton pump inhibitors (PPIs) have drawn extensive scrutiny. However, the association of PPIs in CA-CDI specifically has not been well studied. In a large prospective study from 2009 to 2011 of 984 patients with CA-CDI in eight US states, 31% of patients without prior antibiotic exposure reported PPI use. 17 In a case-control study of CA-CDI cases in a registry in United Kingdom between 1994 and 2004, exposure to PPI during the 90 days before index date was correlated with increased risk of CA-CDI with an OR of 3.5. 28 However, while these studies suggest an association with PPI, there is a need for further, large-scale studies to better understand the relationship between PPI and CA-CDI.
Multiple chronic medical conditions have been associated with increased risk of CA-CDI, including cardiac disease (OR 4.87), chronic kidney disease (OR 12.12) and inflammatory bowel disease (IBD) (OR 5.13). 29 Among these, interest has grown in particular on exploring the relationship between IBD and development of CDI. 1 A population-based study of an IBD registry in Manitoba between 2005 and 2014 found the incidence of CDI to be 512 per 100,000 person-years for ulcerative colitis, 377 for Crohn’s Disease, and 99 for non-IBD patients. 30 Importantly, it is unclear if some of these patients may be colonized with C. difficile in the setting of an IBD flare instead of having an actual infection. 31 In a retrospective study of 1006 patients with IBD diagnosed with CDI, 56% were diagnosed with CA-CDI. Interestingly, among this sub-group, only 16% had steroid use within 1 month prior to CDI diagnosis, and only 30% of patients were exposed to an antibiotic. 32 A prospective study of IBD patients in clinical remission with no recent hospitalization or antibiotic use were found to have higher rates of asymptomatic carriage of C. difficile compared with healthy controls (8.2% versus 1.0%). One potential explanation for the higher incidence of CDI in the IBD population without higher rates of antibiotic exposure is via disruption of the normal microbiome leading to decreased microbiota diversity and richness. Prior studies demonstrated that patients with IBD have alterations in their microbiome as a result of chronic inflammation even before treatment compared with healthy controls, including increased levels of Enterobacteriaceae, Pasteurellacaea, Veillonellaceae and Fusobacteriaceae, and decreased abundance in Erysipelotrichales, Bacteroidales and Clostridiales. 33 The altered microbiome produces less butyrate which maintains gut mucosal integrity and more sialic acid, which is essential for C. difficile catabolism, resulting in a state of dysbiosis which increases susceptibility to CDI.34–36 This dysbiotic state has been well described in CDI patients without IBD. 37 Medications used to treat IBD may also play a role in increased CDI rates for patients with IBD. 32 A meta-analysis on risk factors of CDI in patients with IBD showed that only treatment with biologics and antibiotic use within the previous 30 days of diagnosis confers increased risk of CDI. 38 However, while more than half of the studies in this meta-analysis diagnosed CDI by immunoassay or polymerase chain reaction (PCR), a large proportion used ICD10 codes; therefore, there may be discrepancies in diagnostic accuracy in this analysis. Future studies are needed to differentiate and stratify risk factors for CA-CDI in patients with IBD.
Community reservoirs, strain types and colonization
As the majority of patients with CA-CDI have no prior hospital or antibiotic exposure, multiple studies have attempted to elucidate possible routes of transmission. It has been proposed that many C. difficile reservoirs exist in the community including humans, 39 animals (e.g. ribotype 078 in pigs and cattle), 26 food sources, 40 and the environment (e.g. ribotype 014, 015 and 078 in wastewater plants). 27 A recent analysis of more than 224,000 CDI cases from a large national insurance enrollee database found exposure through family members as the greatest factor for the increased incidence of CA-CDI. 41 A meta-analysis from North America on the relationship of toxigenic C. difficile colonization and subsequent infection found 14.8% of long-term care residents were asymptomatic carriers of toxigenic strains. 42 Another meta-analysis explored the colonization rates of patients upon admission to hospitals and found the global rate to be 8.1%.42,43 Healthy infants are commonly colonized with both toxigenic and non-toxigenic C difficile strains and contact with children <2 years old may be a risk factor for CA-CDI. 44 Interestingly, colonization of non-toxigenic strains may be protective against development of CDI by alteration of host microbiome, as seen in a study of patients with cystic fibrosis. 45 However, colonization of toxigenic strains is still associated with higher risks of infection.43,46
In addition to community reservoirs, several studies have employed sequencing to determine if particular C. difficile strains are responsible for CA-CDI transmission. The most common strain types associated with CA-CDI in United States are ribotypes 027, 106, 014, 002 and 020. 6 The incidence of ribotype 027, previously the most prevalent strain in both HA-CDI and CA-CDI in North America, has been declining since 2011, while ribotype 106 has become the predominant strain since 2014.6,9 A study in Europe found instead five distinct ribotype clusters with no strain dominating the continent; for example, ribotypes 356 and 018 were detected predominantly in Italy, while ribotype 027 was prevalent in Hungary, Italy, Germany, Romania and Poland. 47 Given the different clustering in various regions, it is hypothesized that specific strains circulate in the community locally via community-specific routes. A small prospective study in Canada suggested that the strains associated with CA-CDI are indistinguishable from hospital-acquired CDI. 48 Overall, it remains unclear at this time if specific strain types have contributed more to the rising incidence of CA-CDI. The identification of regional clustering will potentially allow scientists to establish local routes of infection and resistance patterns, which would potentially impact infection control efforts and treatment selection.
Real-world CDI transmission rates outside of healthcare facilities remains an understudied epidemiologic question. In a study using a Markov model built with data extracted from national databases, the transmission rate from a person with CDI to an uncolonized individual in the community was estimated to be 0.1% compared with 0.05% from an asymptomatic colonized person to an uncolonized one. An uncolonized person was estimated to have a probability of 0.12% per day of acquiring CDI in the community, compared with 2.3% in the hospital and 0.37% in a long-term care facility. 49 Despite these findings, the proportion of CA-CDI is rising, and the growing pool of colonized individuals is likely contributing. Future epidemiologic studies will be crucial to understand the mechanisms of community transmission to mitigate its spread.
Recurrent C. difficile infections
CDI recurrence is defined as symptom onset and positive assay result following interim resolution of symptoms with standard of care treatment of a primary episode in the previous 2–8 weeks. 1 However, given that several testing methods are used for clinical detection, reported incidences may not accurately reflect true infections (Supplemental Table 1). PCR tests do not differentiate C. difficile colonization from C. difficile infection. 50 A positive test for CDI must be assessed in clinical context. Also, different testing methods may have varying sensitivities based on ribotype. Guh et al. 51 found that toxin enzyme immunoassay is more sensitive for detecting certain strains, while nucleotide acid amplification testing is not affected by strain types. 51 This has implications in terms of our ability to accurately assess disease burden and epidemiology, and impacts development of tailored approaches to combating C. difficile.
Ma et al. 20 reported that the annual incidence rate of CDI recurrence increased from 0.0107 to 0.0309 per 1000 person-years between 2001 and 2012. 20 More recently, recurrent cases started to decrease during the past decade. In the United States, the estimated number of first recurrent episodes decreased from 93,400 to 69,800 between 2011 and 2017, with incidence dropping from 19.7 per 100,000 to 12.0 per 100,000 over the same time period. 6 The decrease in incidence rate is likely multifactorial, including vigilant antibiotic stewardship, improved testing algorithms and treatment recommendations. Nonetheless, it is estimated that 10–30% of patients in the United States with CDI will still experience at least one recurrent episode, comparable to findings from other regions.5,15,18,52 In the 2020 surveillance by Guh et al., 6 the number of CA-CDI recurrences has been consistently lower than recurrences in HA-CDI, by approximately 21% in 2016 and 2017. This difference is probably due to the younger age of patients and less exposure to healthcare facilities in the CA-CDI population. It is important to note that not all epidemiologic studies routinely distinguish HA-CDI versus CA-CDI when calculating rCDI. Further investigation is needed to understand the burden of recurrent infections in each environment.
Relapse and reinfection
Recurrent CDI cases can be subdivided into relapse and reinfection. A relapse originates from the same strain as the initial infection, while reinfection is caused by a new strain (Table 2). Accurate classification between the two allows for rigorous evaluation of risk factors and treatment effectiveness. Several studies have sought to characterize the epidemiology of relapse versus reinfection for rCDI. Using whole-genome sequencing, Sim et al. 53 determined that 15.8% of the rCDI at a single center were due to reinfection, and one in three such cases would have been misclassified as relapse. 53 Given that whole-genome sequencing may not be widely available or practical, there has been interest in determining an appropriate timeline of recurrence that would help distinguish between relapse and reinfection. In a single-center cohort study conducted in Switzerland, Durovic et al. 54 found that a time cutoff of 20 weeks resulted in acceptable discrimination between relapse and reinfection [receiver operating characteristic (ROC) area under the curve (AUC) 0.741]. Another study conducted in West Australia concluded that a cutoff of 12 weeks yielded a comparable distinction threshold (ROC AUC 0.61). 18 Current clinical guidelines define rCDI as within 8 weeks of successful treatment, regardless of relapse or reinfection. 1 Sequencing C. difficile strains on a patient level to distinguish relapse or reinfection can potentially aid clinical decision-making but faces numerous barriers for widespread adoption.
Early versus delayed recurrence
There are limited data comparing the rates of early versus delayed CDI recurrence in the general population. A single-center study of 120 patients in Korea found that 19.2% of patients developed recurrence within 8 weeks, 19.5% experienced delayed recurrence 8 weeks after initial treatment and 31% experienced a recurrence after 60 months. Risk factors for delayed recurrence include age ⩾70 years, whereas nasogastric tube insertion, PPI and H2-blocker treatment has been associated with both early and delayed recurrence. 55
Risk factors for CDI recurrence
Several risk factors have been identified for rCDI including host factors such as demographics, comorbidities, previous episodes of CDI, as well as medications and environmental factors. In general, older age and female gender have been associated with increased risk for recurrent infections.20,21,54 A meta-analysis showed that age >65 years is an independent risk factor for rCDI (relative risk 1.63). 56 Multiple retrospective studies and cohort studies in North America have shown that women are at increased risk for rCDI compared with men.20,53 Medical conditions such as chronic renal insufficiency (OR 1.59), immunosuppression (OR 9.64) and IBD (HR 1.63) increase the risk of recurrence as well.15,20,57,58 The potential mechanisms of how each of these conditions and others increase risk of rCDI is beyond the scope of this review. A prior history of CDI also increases risk of rCDI episodes, with studies showing that 20% of patients recur after a single episode, 40% after two episodes and 65% after three episodes.52,56,59
Certain medications are associated with increased risk of rCDI. Conflicting data exist on the role of PPI in rCDI. A strong association between PPIs and rCDI was observed in a retrospective study of 45,341 patients with CDI in the United States (OR 1.14). 20 A similar correlation was found in a prospective study (OR 3.75). 60 However, a 6-year retrospective study in Italy did not find a significant correlation between PPI use and increased risk for recurrence (OR 0.94, CI 0.23–3.85). 15 Corticosteroids (OR 1.15) and antibiotics other than those used for CDI treatment (OR 1.79) have also been associated with recurrent infections. 20
Apart from host factors, many studies have examined if specific strains are associated with increased recurrence. Ribotype 027 has been associated with recurrent infections in cohort studies in the United States and the Netherlands.21,54 Infection with other ribotypes, such as F014-020, were more commonly seen in patients with a single episode of CDI. 61 Several other ribotypes are associated with recurrent diseases in other regions (such as ribotype 001 in Sweden and ribotype 014/020 in West Australia).18,62 The presence of multiple strains during the first CDI episode may also be a risk factor for recurrence. 61
Mortality in CDI recurrence
There are conflicting reports regarding mortality associated with rCDI. In a study of inpatient hospitalizations between 2003 and 2009 at one academic tertiary care center, rCDI was associated with a 33% increased risk of mortality at 180 days compared with patients who do not experience a recurrence. 63 However, more recent studies have shown a lower mortality rate in rCDI compared with the initial infection. In a retrospective study of the US veteran population from 2003 to 2014, 30-, 60- and 90-day mortality rates were significantly lower in first CDI recurrence as well as in second recurrence compared with the primary episode (p < 0.0001). 25 Another large study from 128 US Veteran Affairs facilities between 2010 and 2014 confirmed these findings, observing a higher 30-day mortality rate for initial CDI (10.6%) versus first recurrence (8.3%, p < 0.001) and second recurrence (4.2%, p = 0.004). 64 Risk factors for increased mortality include advanced age, PPI use within 7 days before CDI treatment, and any non-CDI related antibiotic use prior to, concurrent with or after C. difficile episode. 64
Treatment for rCDI
Treatment regimens for rCDI vary depending on the number of recurrences and severity of the current episode. For nonfulminant recurrent episodes, vancomycin pulsed taper or fidaxomicin are the recommended antibiotic therapies. Crook et al. 65 found fidaxomicin to be superior to vancomycin in preventing recurrence in a meta-analysis of two large randomized trials [Relative Risk (RR) 0.54, 95% CI 0.42–0.71]. Fecal microbiota transplant (FMT) can be considered after two recurrences. 1
FMT has garnered strong interest for its potential in prevention of CDI recurrence. In a recent small randomized study comparing FMT, fidaxomicin and vancomycin for the treatment of rCDI, significantly more patients who underwent FMT remained symptom-free at 8 weeks post-treatment (p = 0.009 for FMT versus fidaxomicin; p = 0.001 for FMT versus vancomycin). 66 In another prospective study of 19 patients, the efficacy rate of FMT was 85%, and the post-treatment stool analysis showed significantly increased bacterial diversity compared with the pre-FMT specimens. 67 In a meta-analysis of randomized controlled trials (RCTs) for prevention of rCDI, FMT was found to be superior to oral vancomycin in the prevention of rCDI. 68 Recent cost-effectiveness studies have shown FMT to dominate all other strategies for the treatment and prevention of rCDI. 69 However, the reported range of efficacy rates of FMT have been wide, and the more recent RCTs have shown lower efficacy rates than the open-labeled studies. 70 The quality of data is limited by variations in methodologies, including lack of control arms, difference in antibiotic suppressive therapies, and selections of CDI diagnostic assays, all of which likely contribute to the discrepancy. 68
Bezlotoxumab, a monoclonal antibody against C. difficile toxin B, has also been studied as an option to reduce risk of recurrence, with the MODIFY I and II trials demonstrating significant efficacy in preventing CDI recurrence over placebo (RR 0.62, 95% CI, 0.51–0.75). 71 Scaling of these newer strategies to treat rCDI will likely impact the epidemiology and incidence in the next decade. Further studies will be helpful to guide positioning of various therapies in our armamentarium for treating rCDI, balancing efficacy, safety and cost-effectiveness.
COVID-19 and CDI
Lastly, there have been ongoing efforts to monitor the trend of CDI during the COVID-19 pandemic. The published data so far showed that there has not been an increase in the rate of CDI despite rising high-risk antibiotic exposures because of COVID-19.72,73 In some centers, there has been a reduction in HA-CDI cases.74,75 Multiple factors potentially contributed to the decrease. Among them, one important aspect has been improved infection prevention measures such as higher compliance in hand hygiene and isolation precautions.74,76 Only one small study specifically commented on CA-CDI versus HA-CDI, finding that six out of 38 CDI cases were community-onset, and two out of 38 were rCDI. 76 In that study, COVID-19 patients with CDI had worse outcome than those without CDI, including longer hospital stay (35 days versus 19.4 days, p < 0.01) and lower rates of full recovery without complications (50% versus 64.9%, p = 0.01). 76 However, most of these cases were hospital-onset, and the trend in CA-CDI has not been clearly delineated. Further studies are needed to explore the interplay between COVID-19 and CDI, especially given the exposure to steroids and antibiotics in patients who received treatment for COVID-19.
Conclusion
Despite an overall decrease in CDI rates worldwide in the last decade, community-associated cases are increasing while the rates of recurrence of CDI are steady. CA-CDI accounts for almost 48% of annual cases in the United States and ranges from 10% to 43% of total cases across global regions. Continued efforts directed at improving disease detection and tracking are needed to help identify community reservoirs and understand patterns of transmission. While rCDI cases have decreased in the United States, rCDI remains a leading cause of significant healthcare morbidity and global economic burden. Importantly, the risk factors and disease characteristics of CA-CDI and rCDI differ regionally, calling for rigorous future investigations of various host factors, pathogen ribotypes, local reservoirs and transmission vectors specific to each region. Standardization of laboratory testing for the detection of CDI is critical to accurately characterize true infections versus colonization. With the availability of highly sensitive tests such as whole-genome sequencing, our understanding of CDI pathogenesis, transmission and colonization will continue to evolve over the next decade.
Supplemental Material
sj-docx-1-tag-10.1177_17562848211016248 – Supplemental material for Epidemiology of community-acquired and recurrent Clostridioides difficile infection
Supplemental material, sj-docx-1-tag-10.1177_17562848211016248 for Epidemiology of community-acquired and recurrent Clostridioides difficile infection by Yichun Fu, Yuying Luo and Ari M Grinspan in Therapeutic Advances in Gastroenterology
Footnotes
Conflict of interest statements
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.